Pfeiffer Syndrome Type 1: A Case Report
Kocak GE, Saruhanoglu A, Yaltirik M, Koray M*
Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Istanbul University, Istanbul, Turkey.
*Corresponding Author
Dr. Meltem Koray,
Associate Professor, Faculty of Dentistry,
Department of Oral and Maxillofacial Surgery Çapa,
Istanbul University, 34093, Fatih, Istanbul, Turkey.
Tel: 00905055116448
Fax: 2125312230
E-mail: mkoray@istanbul.edu.tr
Received: February 23, 2018; Accepted: March 23, 2018; Published: March 24, 2018
Citation:Kocak GE, Saruhanoglu A, Yaltirik M, Koray M. Pfeiffer Syndrome Type 1: A Case Report. Int J Dentistry Oral Sci. 2018;5(3):626-629. doi: dx.doi.org/10.19070/2377-8075-18000122
Copyright: Koray M©2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Pfeiffer syndrome is a rare syndrome which is defined by Pfeiffer in 1964 is autozomal dominant and characterized with variable severity of brachycephalic skull, regressed midface, expansion in hands and feet, broad thumb and big toes syndactyly. This syndrome is defined as a rare syndrome with autosomal, dominantly inherited. Genetic mutations are rare but possible. The syndrome plays a role of craniosynostosis of coronal, lambdoid and occasionally sagittal suturas. Eyes are seen puffy due to shallow orbital structure and resulted by maxillary hipoplasia (ocular proptosis). Hipertelorism and down sloping palpebral fissures are common and strabismus is often seen. Intelligence is normal. In this case report, we aim to present the performed rimary teeth extractions and following up in 4 years old girl with type 1 Pfeiffer Sydrome.
2.Introduction
3.Case Report
4.Discussion
5.References
Keywords
Pfeiffer Syndrome; Syndactyly; Craniosynostosis; Congenital Anomalies.
Introduction
Pfeiffer's syndrome (PS) is a rare, autosomal dominant, variableseverity acrocephalic skull characterized by Pfeiffer in 1964, characterized by a declined midface, hands and feet, and large thumb and large foot syndactyly [1]. PS is characterized by the appearance of skull and leg anomalies in eight individuals from three quadrants [2].
PS, which is seen in 100,000 cases, is usually described as a syndrome with a craniosynostosis of coronal sutures, a large hand and a toe, and a rare, autosomal, dominant transition syndrome [3]. Genetic mutations are rarely possible. Patients have premature fusion of the coronal and lambdoid sutures and occasionally ofthe sagittal sutures, leading to an abnormal skull shape [2].
Characteristically, clinical images include; turribrakisefali (sharp rounded head shape, pronounced and protruding forehead) and maxillary hypoplasia, exophthalmos, small zygoma and undeveloped maxilla. Sometimes partial soft tissue as syndactyly also could be seen in the hand [2]. Eyes seem swollen due to shallow orbitas that is caused by maxiller hypoplasia (ocular propitosis). Hypertelorism and downward sloping palpebral fissures are common and strabismus is seen. Intelligence is normal. The broad hand and toes are characteristic for the syndrome. It is reported with a review of literature the first neonate in Korea with PS who had bicoronal craniosynostosis, bilateral syndactyly of fingers and toes [1].
Other characteristics of PS are; lower ear lobes and finger anomalies. Intra oral features include mandibular prognathism, malocclusion, cleft pseudo-palate and bifid uvula, enlargement of the alveolar bone, high palatal arch, and crowded teeth [4, 5]. Cohen classified PS into three clinical subtypes according to phenotype severity. Type 1 (classical) PS includes individuals with mild findings of normal neurological and mental development. Type 1 (classical) PS may be dominant. Type 2 PS, clover leaf skull, broad hands and feet, severe exophthalmos, central nervous system involvement, elbow ankylosis or synostosis. Type 3 PS, similar to Type 2. The only difference is that the clover leaf skull is not visible. Type 2 and 3 cause premature death due to severe neurological complications and various vascular problems [6]. In this case report, we aimed to present a case of 4-year-old girl who had Type 1 PS in our clinic.
Case Report
As a result of physical examination performed in a 4-year-old girl who applied to our clinic due to dental problems, turribrachycephaly, maxillary hypoplasia, ocular propitosis, hypertelorism, strabismus, exophthalmos were detected (Picture 1). According to patient record, it was understood that the mother of the patient gave birth her 1.800 g weight and 48 cm height with cesarean section. Her mother has normal pregnancy period and her mother and father have 1st degree relative marriage. Post-natal infants have a diagnosis of PS due to turribrachycephaly, maxillary hypoplasia, ocular proptosis, hypertelorism, strabismus, exophthalmos. It wasn’t found soft tissue syndactyly and wide hands and feet that seen in the PS, and the intelligence of the case was reported to be normal (Figure 2, 3). The intraoral clinical and radiological examination revealed that oral hygiene was not good and had quite a lot caries and loss of teeth (Figures 4, 5 and 6). Primary teeth, which have wide caries and defects, were extracted under local anesthesia (Figures 7 and 8) and 2% NaF gel application was performed for prophylaxis in order to prevent new caries. The case is still under control.


Figure 1. 4-year-old girl turribrakisephaly, maxillary hypoplasia, ocular propitosis, hypertelorism, strabismus, exophthalmos.
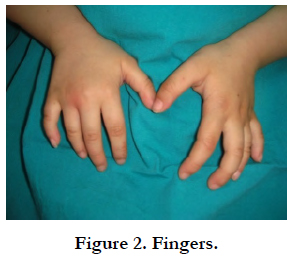

Figure 2. Fingers.
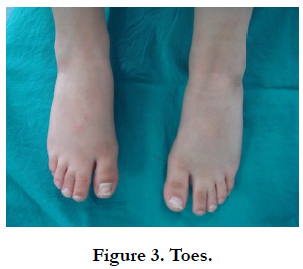

Figure 3. Toes.
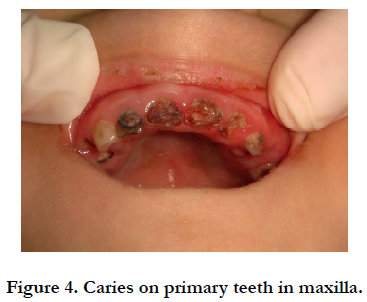

Figure 4. Caries on primary teeth in maxilla.
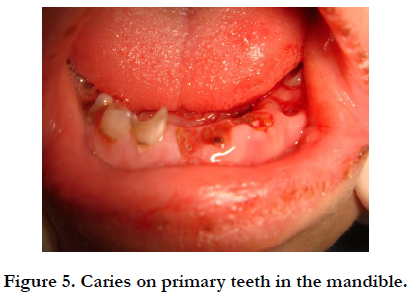

Figure 5. Caries on primary teeth in the mandible.
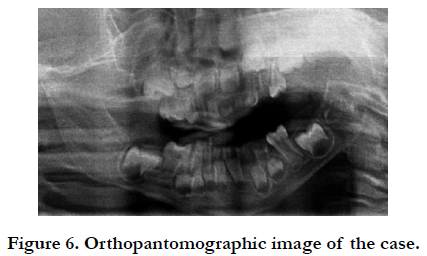
Figure 6. Orthopantomographic image of the case.
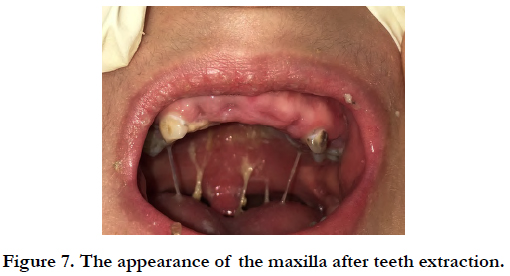

Figure 7. The appearance of the maxilla after teeth extraction.
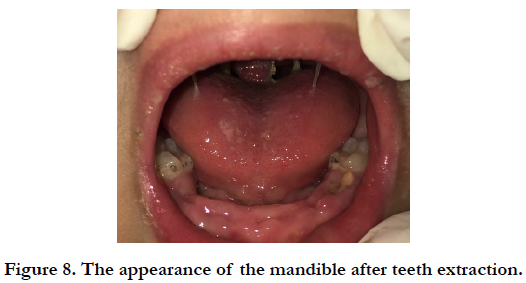

Figure 8. The appearance of the mandible after teeth extraction.
Discussion
Although the incidence of PS is unknown, it is reported to be 1 in 100,000 [2]. It has also been reported that cases with Type 1 PS have good prognosis. Patients with Type 2 and Type 3 prognosis have reported early death in spite of aggressive medical and surgical treatment [1]. Our case was Type 1 PS and the clinical findings were relatively acceptable in comparison with other types. The etiology of PS is not entirely clear, but it is thought to be a craniofacial syndrome and mutations in the fibroblast growth factor receptor (FGFR). It is known that FGFR 2 and FGFR 1 receptors are caused by mutations in exons IIIa and IIIc [7]. Some studies have reported that these mutations originate from the chromosome 8p11.22-P12 in the FGFR1 gene and from the chromosome 10q25-q26 in the FGFR2 gene [8]. These mutations are thought to be related to the older ages of the parents. These mutations are associated with the fact that sperm have a selective advantage for survival, especially for men [9]. Her parents have 1st degree relative marriage. The syndrome is caused due to that reason according to our estimation. Bannink et al., reported that obstructive sleep apnea developed in approximately 50% of patients with Apert, Crouzon, or PS due to moderate hypoplasia [10]. Boutros et al., reported in patients with Apert, Crouzon, and PS, a narrowed cranial tendon caused narrowed condylar area, and mandibular anomalies appeared in the form of decreasing bicondylar width and bigonial width is normal [11]. In our case, only turribrachycephaly, maxillary hypoplasia, ocular proptosis, hypertelorism, strabismus, exophthalmos have been observed and still following to detect possible anomalies. Patients that referred in the dentist clinic are often healthy individuals; patients with the syndrome are rare. These types of syndromes, which could not be solved in private dental clinic, are mostly directed to Oral and Maxillofacial Surgery clinics. As with all syndromes, individuals with PS have specific characteristics such as turribrakisephaly, maxillary hypoplasia, ocular propitosis, hypertelorism, strabismus, exophthalmos. For this reason, to direct his/her family correctly, having respectable knowledge about the PS by dentists is a must.
References
- Park MS, Yoo JE, Chung J, Yoon SH. A case of Pfeiffer syndrome. J Korean Med Sci. 2006 Apr 1;21(2):374-8.
- Vogels A, Fryns JP. Pfeiffer syndrome. Orphanet J Rare Dis. 2006 Dec;1(1):19.
- Giancotti A, D'Ambrosio V, Marchionni E, Squarcella A, Aliberti C, La Torre R, et al. Pfeiffer syndrome: literature review of prenatal sonographic findings and genetic diagnosis.J Matern Fetal Neonatal Med. 2017 Sep; 30(18):2225-2231.doi:10.1080/14767058.2016.1243099.PubMed PMID: 27762162.
- Stoler JM, Rosen H, Desai U, Mulliken JB, Meara JG, Rogers GF. Cleft palate in Pfeiffer syndrome. J Craniofac Surg. 2009 Sep;20(5):1375-7. PubMed PMID: 19816260.
- Jain RR, Rabb MF. The Difficult Pediatric Airway. In: Hagberg CA, editors. Benumof and Hagberg's Airway Management. 3rd ed. Philadelphia: Saunders; 2013. p. 723-760.
- Cohen MM. Pfeiffer syndrome update, clinical subtypes, and guidelines for differential diagnosis. Am J Med Genet. 1993 Feb 1;45(3):300-7. PubMed PMID: 8434615.
- Teebi AS, Kennedy S, Chun K, Ray PN. Severe and mild phenotypes in Pfeiffer syndrome with splice acceptor mutations in exon IIIc of FGFR2. Am J Med Genet. 2002 Jan 1;107(1):43-7. PubMed PMID: 11807866.
- Plomp AS, Hamel BC, Cobben JM, Verloes A, Offermans JP, Lajeunie E, Fryns JP, de Die‐Smulders CE. Pfeiffer syndrome type 2: further delineation and review of the literature. Am J Med Genet. 1998 Jan 23;75(3):245-51. PubMed PMID: 9475590.
- Goriely A, McVean GA, Röjmyr M, Ingemarsson B, Wilkie AO. Evidence for selective advantage of pathogenic FGFR2 mutations in the male germ line. Science. 2003 Aug 1;301(5633):643-6. PubMed PMID: 12893942.
- Bannink N, Nout E, Wolvius EB, Hoeve HL, Joosten KF, Mathijssen IM. Obstructive sleep apnea in children with syndromic craniosynostosis: longterm respiratory outcome of midface advancement. Int J Oral Maxillofac Surg. 2010 Feb;39(2):115-21. PubMed PMID: 20056390.
- Boutros S, Shetye PR, Ghali S, Carter CR, McCarthy JG, Grayson BH. Morphology and growth of the mandible in Crouzon, Apert, and Pfeiffer syndromes. J Craniofac Surg. 2007 Jan;18(1):146-50. PubMed PMID: 17251854.





