Parent Beliefs about Infant Teething and Mothers’ Practices: A Survey of Tunisian Parents
Rekik Y1*, Ben Daya M1, Jemmali B2
1 Resident in Pediatric Dentistry, La Rabta Hospital, Tunisia.
2 Professor in Pediatric Dentistry, Head of Dentistry Department, La Rabta Hospital, Tunisia.
*Corresponding Author
Rekik Yacine,
Faculty of Dental Medicine of Monastir, Tunisia.
Dentistry department, La Rabta Hospital, Tunis, Tunisia.
Third year resident in Pediatric dentistry, University of Monastir, Tunisia.
Tel: 0021622327743
E-mail: rek.yacine@gmail.com
Received: May 05, 2017; Accepted: May 24, 2017; Published: May 26, 2017
Citation: Rekik Y, Ben Daya M, Jemmali B (2017) Parent Beliefs about Infant Teething and Mothers’ Practices: A Survey of Tunisian Parents. Int J Dentistry Oral Sci. 4(5), 476-480. doi: dx.doi.org/10.19070/2377-8075-1700093
Copyright: Rekik Y©2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aim: The purpose of this study was to find the relation between local and systemic manifestations during primary teeth eruption in the region of Tunis, Tunisia.
Materials And Methods: A cross sectional descriptive study involving 300 children aged from 6 months to 6 years was conducted. Questionnaires were distributed to all mothers and were used to inquire on the local and systemic symptoms associated with teething and measures used to decrease signs and pain they described. Data entry and analysis were done using an SPSS program version 23.0.
Results: Teething symptoms were reported in 90.3% (271/300) of the children. The most common findings were Fever (60.7 %) and drooling (57%), the least common symptom observed in the study was jugal erythema (16%). 42% of mothers took some action to resolve teething symptoms. Giving an object to chew (32.7%) was the most common method used.
Conclusion: Many local and systemic symptoms were found during primary teeth eruption. Most manifestations were found during eruption of the primary incisors.
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Conclusion
7.Acknowledgement
7.References
Keywords
Deciduous Teeth; Tooth Eruption; Child; Symptoms; Tunisia.
Introduction
Teething is a natural physiological process in which the tooth moves from its developmental site to its functional position in the oral cavity [1].
Eruption of primary teeth is considered as a turning point during child development. Indeed, it is related to general and oral symptoms which can cause worry and disturbance to the parents [2]. And they feel unconfident to relieve the pain of the child.
Sleep disturbance, fever, decreased appetite, diarrhea, increased salivation, irritation of the gums and agitated mood are the complaints most associated with teething [3].
Within reach, no publication showing symptoms associated with teething among Tunisians was reported. The aim of this study was to report a survey of local and general symptoms associated with teething and the related mothers’ practices. The results may be used to raise awareness among health professionals and advise parents about infant teething.
Materials and Methods
A cross sectional study was conducted among mothers escorting children aged from six months to six years old at the Pediatric Dentistry department and Pediatrics department at the university hospital La Rabta, Tunis, Tunisia. The sample size was pre-determined to be 300 subjects. The study was conducted over a 2-month period: February and March 2017. About 5 to 8 mothers per day, who came with the aim of routine follow-up, were invited to participate in our study. The study was done by the principal author in the consultations room at the Pediatric Dentistry department and the treatments room at Pediatrics department.
Structured questionnaires were made to inquire on local and systemic symptoms associated with teething and measures taken by mothers if their children get those symptoms. The questions concerned the child (sex, age), local teething symptoms (Red and inflamed gums, local gingival swelling, pain, drooling and jugal erythema) and systemic teething symptoms (Anxiety, fever, Diarrhea, Constipation, sleep disturbance, decreased in appetite, vomiting, prolonged digits or objects sucking and diaper rash).
A lack of an oral consent by the parent, presence of a permanent tooth, systemic disease as well as a physical or mental disability.
The collected information was analyzed using an SPSS program version 23.0. Chi square test was used to determine if there is a significant relationship between two variables. P < 0.05 was chosen as a level of significance.
Results
The study group included 300 children (140 boys and 160 girls), and their mothers. Age characteristics of children were included in Table 1. The mean age for boys was 3.96 ± 1.58 and 4.02 ± 1.78 for girls. Children were born between 2010 and 2016. Sorted by year, the largest number of the sample was born in 2013 who were sixty-two children (20.6%).
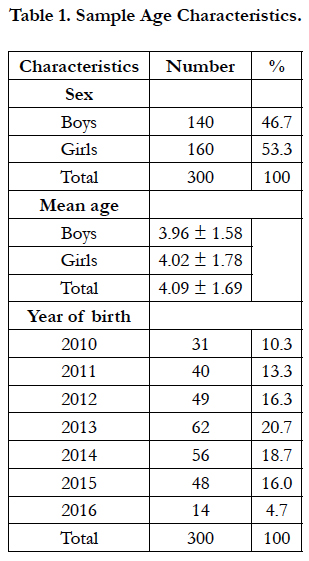

Table 1. Sample Age Characteristics.
Local and systemic symptoms associated with teething are conferred respectively in Table 2 and Table 3. We did not mention general or local symptoms in twenty-nine children (9.7%). Teething symptoms were reported in 90.3% (271/300) of the children. Each manifestation appeared alone or in combination with others. The local symptoms frequently reported were drooling (57%), pain (56.3%), red and inflamed gums (41%), local gingival swelling (38%) and jugal erythema (16%). These symptoms were clearly more important during the eruption of the incisors and canines than during the eruption of the molars. In fact, the eruption of the incisors and canines caused salivation and pain respectively in 35 % and 34% of the cases, whereas 22 % and 22.3 % during the eruption of the molars.
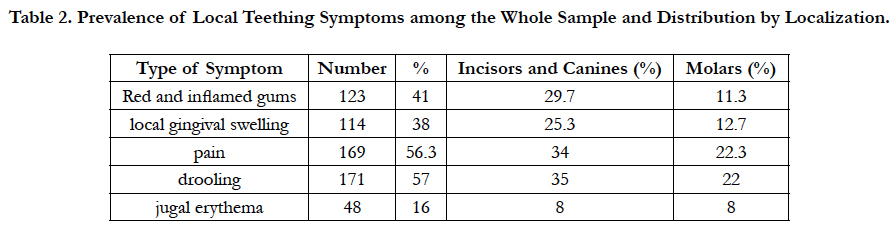
Table 2. Prevalence of Local Teething Symptoms among the Whole Sample and Distribution by Localization.
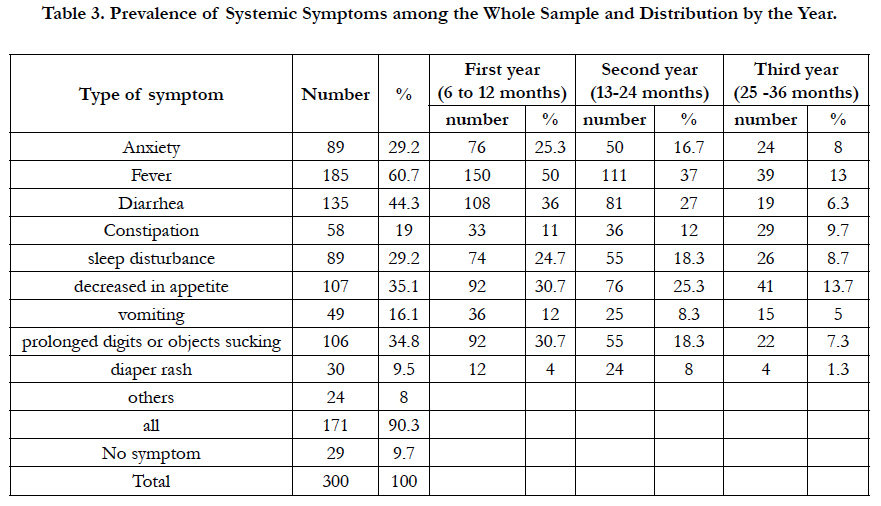
Table 3. Prevalence of Systemic Symptoms among the Whole Sample and Distribution by the Year.
The most frequent general manifestations were: Fever (60.7 %), diarrhea (44.3 %), decreased in appetite (35.1 %), prolonged digits or objects sucking (34.8 %), Anxiety (29.2%), sleep disturbance (29.2%), constipation (19%), vomiting (16.1%) and diaper rash (9.5%).
Others clinical manifestations were found in 29 children (8%). They were mainly a urinary tract infection and skin rash. There was one case of otitis.
General symptoms were more frequent in the first year (6 and 12 months). Fever was found in the first year in 50% of the cases versus 37% in the second year and 13% in the third year. The diarrhea was also present in 36% of the cases in the first year versus 27% in the second year and 6.3% in the third. During the second year, only three symptoms were more frequent which were constipation (12%), diaper rash (8%) and jugal erythema (7.9%). On the other hand, no symptoms were more important in the third year.
According to 271 (90.3%) mothers, deciduous teeth eruption was accompanied with symptoms. Less than half of them (42%) took some action in order to decrease clinical signs and relive their children’s pain (Table 4).
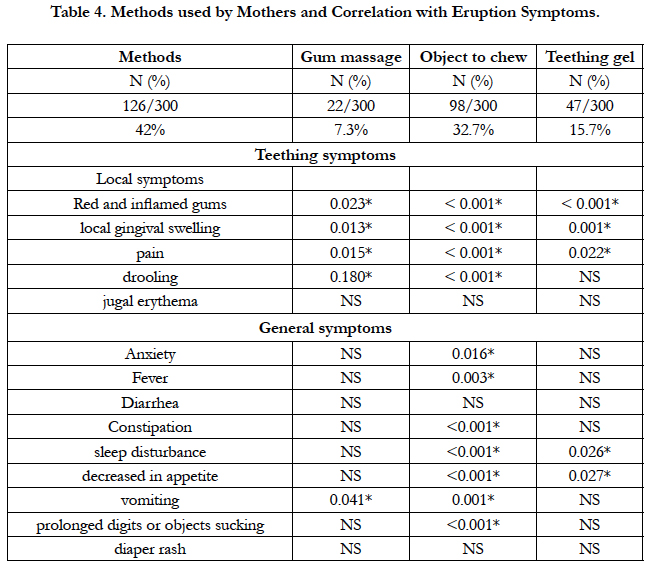
Table 4. Methods used by Mothers and Correlation with Eruption Symptoms.
As reported by the mothers: 7.3% (n=22) practiced gum massage of some sort, 32.7% (n=98) gave the child an object to chew, 15.7% (n=47) applied a teething gel. The actions taken were selfprescribed by mothers.
The object to chew was a teething ring brought from chemistry. They were two types, either simple or filled with liquid that must be cooled and given to the child.
A statistically significant positive correlation was noted between using gum massage and red and inflamed gums (p=0.023), local gingival swelling(p=0.013), pain(p=0.015), drooling(p=0.180) and vomiting (p=0.041). The use of an object to chew have a statistical signification with all the symptoms except jugal erythema, Diarrhea and diaper rash. And using a teething gel was statistically significant with Red and inflamed gums (p=<0.001), local gingival swelling (p=0.001), pain (p=0.022), sleep disturbances (p=0.026) and vomiting (p=0.027).
Concerning mothers' attitudes toward children whose year of birth is > 2013 and ≤ 2013 (Table 5), mothers whose children are older used more frequently methods to decrease symptoms (66.7%) than mothers of younger children (33.3%), this is not statistically significant.
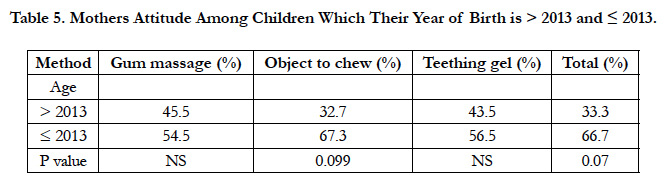
Table 5. Mothers Attitude Among Children Which Their Year of Birth is > 2013 and ≤ 2013.
Discussion
Our study reported that 90.3% of children with deciduous teeth eruption manifested general and local symptoms. This finding was in accordance with the result of previous studies which showed a prevalence of 80 to 90% [4]. These symptoms appeared alone or with others local or systemic.
Parents represent a source that can be relied on. In fact, they follow the development of children and witness any change in behavior, mood, or health. So, they can detect any related problem [5].
Similar to previous reports, the most frequent symptoms during primary tooth eruption are fever, diarrhea, gum swelling, irritation and redness of the gums [6]. They also reported a variety of other symptoms. In our study, fever was the first symptom (60.7%) which is in accordance with the findings of GaliIi et al., [7], Carpenter [8], and Jaber et al., [4]. Then, it was followed by drooling (57%), pain (56.3%) and diarrhea (44.3%).
Fever was associated with teething and the mean daily temperature in days of non-eruption was between 36.90°C and 37.10°C, and on the eruption day 37.60°C [5].
The period of teething coincides with many changes in the baby’s physiology. We notice a reduction of the immunity and an increase of infectious diseases like respiratory tract infections, urinary tract infections, middle ear infections, etc.[9]. In fact, infants lose maternal antibody protection against bacteria and viruses while a newly pierced gingiva around an erupting tooth is in progress which offers a convenient viral infection site [10].
Bennet and Brudno [11] suggested that fever during teething was caused by the human teething virus (HT virus). It remains in a latent state until its activation through eruptive movements. The human teething virus is responsible of a primary infection, provoking fever and other symptoms such as gingival inflammation and pain.
There was statistically significant result on comparison between diarrhea and prolonged digits or objects sucking. There was a concordance respectively for diarrhea and object chewing during the first year (36%-30.7%), second year (27%-18.3%) and third year (6.3%-7.3%). Foster and Hamilton [12] suggested that diarrhea during tooth eruption was associated with the contamination of the baby’s fingers or objects put into the mouth.
Regarding the local signs, the most frequent was drooling (57%), mostly in Incisors and Canines followed by pain (56.3%). Teething stimulates salivation. It became generally an excessive reaction when an unusual phenomenon is happening in the mouth. It is the case of deciduous tooth which is gradually pushing toward the gum's surface, and it can start months before the eruption. The canine eruption seems to be the most difficult due to the presence of the canine tip as well as the mesial and distal angle. Drooling at the age of 4 or 5 months could have been associated with dental eruption, but it also could have been a sign of the normal activity of the salivary glands [12].
The clinical manifestations associated with the teething process decreased with age. Most symptoms were found between the ages of 4 to 12 months. After that, a reduction was noticed in the second and the third year.
Pharmacological strategies for teething generally aim to achieve analgesia, anesthesia, sedation or a combination of these [13]. The use of a cold teething ring is intended to decrease the gums inflammation and consequently the pain. It causes localized vasoconstriction. Chewing an object gives further relief by applying pressure to the gums.
Limitations of our study were represented by the subjectivity of the parents’ observations. It is difficult to identify and separate the signs and symptoms related to dental eruption. This was due to the extended period of time of the teething and the numberless infections that can affect the baby.
In addition, some symptoms need more specific examination, such as diarrhea that may be caused by infection and, without a virology study the diagnostic is not conclusive.
On the other hand, more recent studies revealed that most systemic teething symptoms are due to other causes [14]. Teething cannot cause fever greater than 38.9°C. The belief that teething causes systemic symptoms is unfounded, but localized symptoms and low-grade fever may be seen [15].
Conclusion
The study sample was selected from the people visiting one health institute. This of course, may not be representative of whole population. Further research is needed on larger populations and should include specific examination tools.
On the basis of the results of our study, we arrived at the following conclusions: a) fever was the most prevalent sign followed by drooling and pain. b) Most signs appeared during the eruption of the primary incisors. c) We recommend for Tunisian mothers: - No confusion between dental eruption and early childhood illness. - No medication because teething is physiological. - Information on dental eruption for mothers (age, chronology and complications).
Acknowledgement
The authors would like to thank Mr Rached Hassen, English editor, for his help in proof reading the article.
References
- Cahill DR, Marks SC Jr (1980) Tooth eruption: evidence for the central role of the dental follicle. 9(4): 189–200.
- Wilson PH, Mason C (2002) The trouble with teething-misdiagnosis and misuse of a topical medicament. Int J Paediatr Dent. 12(3): 215–218.
- Ramos-Jorge J, Pordeus IA, Ramos-Jorge ML, Paiva SM (2011) Prospective longitudinal study of signs and symptoms associated with primary tooth eruption. Pediatrics. 128(3): 471-476.
- Jaber L, Cohen IJ, Mor A (1992) Fever associated with teething. Arch Dis Child. 67(2): 233–234.
- Squires J, Bricker D, Heo K, Twombly E (2001) Identification of socialemotional problems in young children using a parent-completed screening measure. Early Child Res Q. 16(4): 405–419.
- Kawia HM, Kahabuka FK (2009) Symptoms associated with teething in Tanzania. Pediatric dent J. 19(1): 9–14.
- Galili G, Rosenzweig KA, Klein H (1969) Eruption of primary teeth and general pathologic conditions. ASDC J DentChild. 36(1): 51–54.
- Carpenter JV (1978) The relationship between teething and systemic disturbances. ASDC J Dent Child. 45(5): 381-384.
- Wake M, Hesketh K, Allen M (1999) Parent beliefs about infant teething: a survey of Australian parents. J Paediatr Child Health. 35(5): 446-449.
- Seward MH (1971) Local disturbances attributed to eruption of the human primary dentition. A survey. Br Dent J. 130(2): 72-77.
- Bennet HJ, Brudno DS (1986) The teething virus. Pediatr Infect Dis. 5(4): 399-401.
- Roshan NM, Sakeenabi B (2012) Teething disturbances; prevalence of objective manifestations in children under age 4 months to 36 months. Med Oral Patol Oral Cir Bucal. 17(3): 491-494.
- Meer Z, Meer A (2011) Teething trouble and its management in children. Intl J Dent Clin. 3(2): 75-77.
- McIntyre G, McIntyre G (2012) Teething troubles? Br Dent J. 192(5): 251-255.
- Markman L (2009) Teething: Facts and Fiction. Pediatr Rev. 30(8): 59-64.





