A New Procedure Reduces Laboratory Time to 6 Hours for the Elaboration of Immediate Loading Prostheses with a Titanium Frame Following Implant Placement
Huard C, Bessadet M, Nicolas E, Veyrune JL*
Clermont University, University of Auvergne, CROC EA4847, BP 10448, F-63000 Clermont-Ferrand, France & CHU de Clermont-Ferrand, Service d'Odontologie, F-63000 Clermont-Ferrand, France.
*Corresponding Author
Jean-Luc VEYRUNE,
Clermont University, University of Auvergne, CROC EA4847, BP 10448, F-63000 Clermont-Ferrand, France & CHU de Clermont-Ferrand, Service d'Odontologie, F-63000 Clermont-Ferrand, France.
Tel: +0 33 473177382
Email: jean-luc.veyrune@inserm.fr
Received: May 12, 2016; Accepted: June 10, 2016; Published: June 13, 2016
Citation: Huard C, Bessadet M, Nicolas E, Veyrune JL (2016) A New Procedure Reduces Laboratory Time to 6 Hours for the Elaboration of Immediate Loading Prostheses with a Titanium Frame Following Implant Placement. Int J Dentistry Oral Sci. 3(6), 268-272.DOI : dx.doi.org/10.19070/2377-8075-1600054
Copyright: Veyrune JL© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Good primary stability and no micromovements during the healing stage are the two main factors predicting successful osseointegration. Therefore, the international literature on immediate loading emphasizes the importance of using a rigid framework on an interim acrylic prosthesis to bind the implants for 48 to 72 hours after implant placement. This report describes the procedure of the Euroteknika “all in bar” system which can shorten this time to 6 hours. The cast was prepared with the abutment replica and mounted on an articulator by the dental laboratory. The abutments with winglets were arranged on tetra abutments in order to create the frame. The frame was finished using laser welding to join the winglets together. Teeth were then mounted according to the validated diagnostic set-up, fixed on the frame with a self-polymerized resin, and set in the mouth. The “all in bar” frame containing abutments with winglets constitutes a rigid milled titanium frame which is obtained without using an outside milling center. The advantages of such a procedure would be to reduce the toothless period of patients while providing the excellent implant stability required for good osseointegration.
2.Clinical procedure
3.Discussion
4.Conclusion
5.References
Introduction
Good primary stability and no micromovements during the healing stage are the two main factors predicting successful osseointegration [1]. Traditionally, it was recommended to leave implants free from stress for 3 to 4 months at the mandible and for 6 to 8 months at the maxilla to reduce implant encapsulation [2]. In 1990, the first longitudinal study suggested that implants could be loaded immediately or at an earlier stage at the mandible [3]. This procedure has since been widely implemented at both the mandible and the maxilla with success rates similar to those of delayed loading [4, 5]. The international literature on immediate loading emphasizes the importance of using a rigid framework on an interim acrylic prosthesis to bind the implants for 48 to 72 hours after implant placement [6, 7]. This report describes the procedure of the Euroteknika “all in bar” system which can shorten this time to 6 hours.
Clinical procedure
The “all in bar” procedure was constructed around an articulator based on study models (Figure 1). The prosthetic space had to be defined as precisely as possible. A splint was fitted on a duplicated diagnostic set-up to allow the practitioner to freely place all the implants in the prosthetic space defined previously (Figure 2a and 2b). Then, an open individual photo-curing resin tray was produced to facilitate the positioning impression of the Tetra implant abutments placed on Naturactis implants.
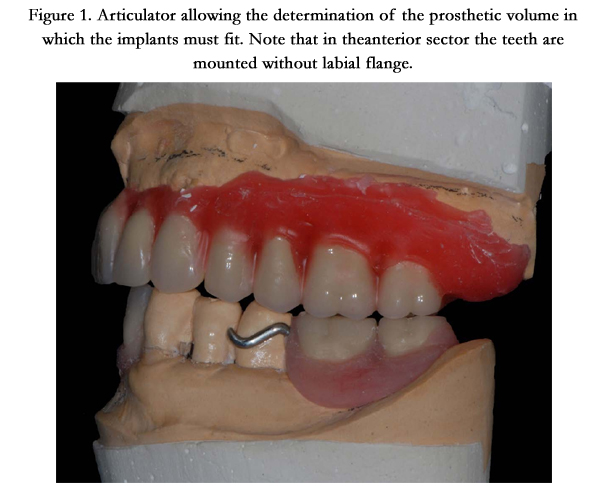
Figure 1. Articulator allowing the determination of the prosthetic volume in which the implants must fit. Note that in the anterior sector the teeth are mounted without labial flange.
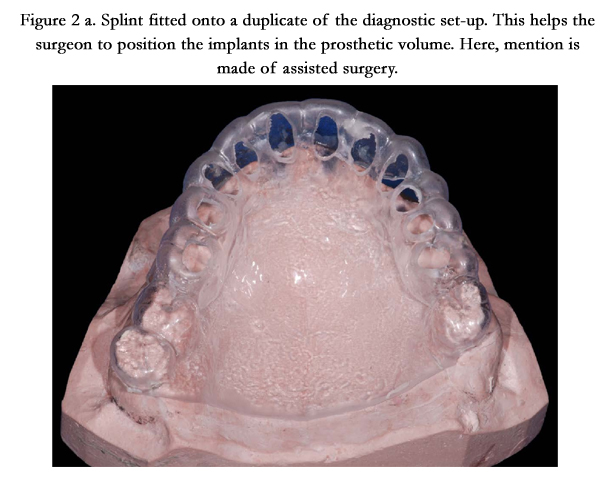
Figure 2 a. Splint fitted onto a duplicate of the diagnostic set-up. This helps the surgeon to position the implants in the prosthetic volume. Here, mention is made of assisted surgery.
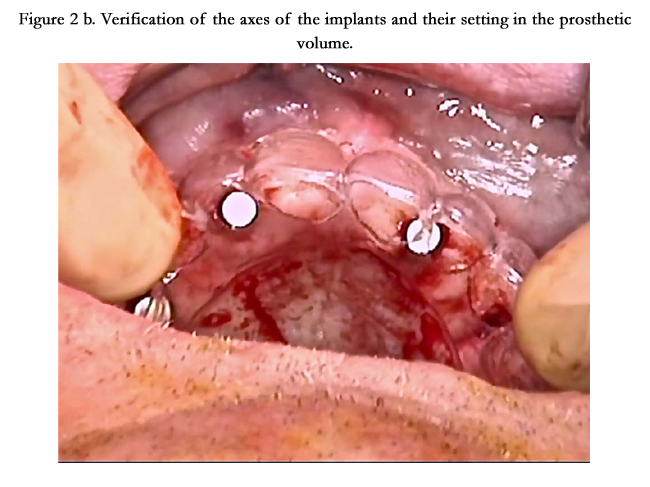
Figure 2b. Verification of the axes of the implants and their setting in the prosthetic volume.
Implants were placed with the splint that was perforated in front of the sites selected based on clinical examination and panoramic X-ray or con-beam images. The axis of the implants was perfectly perpendicular to the occlusal plane to facilitate the construction of the bar. This step was essential when using Tetra standard abutments that did not allow axis realignment: abutment winglets were therefore always perpendicular to the implant axis. However, it is sometimes necessary to use Tetra angulated abutments to avoid anatomical obstacles or an over-palatal or too lingual screwing axis. Whatever the case, the abutment axis should not point in the mesio-distal direction, which would oblige the dental laboratory technician to rework the winglets to make them parallel to the occlusal plane. In addition to the loss of time, the vertical dimension of the frame would be reduced.
Impressions for abutment positioning were performed by encased transfer with elastomeric polyether material (Impregum®) (Figure 3).
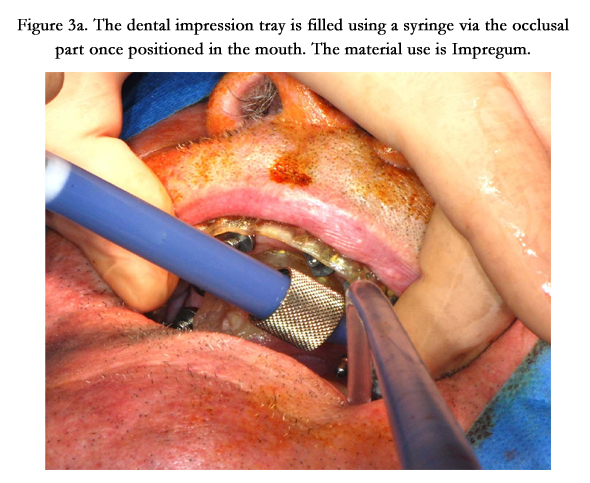
Figure 3a. The dental impression tray is filled using a syringe via the occlusal part once positioned in the mouth. The material use is Impregum.
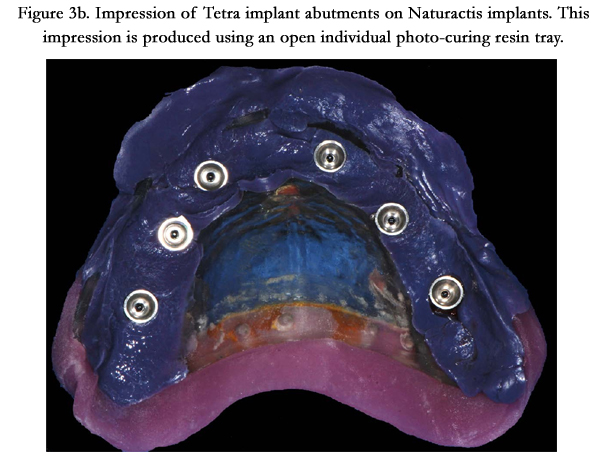
Figure 3b. Impression of Tetra implant abutments on Naturactis implants. This impression is produced using an open individual photo-curing resin tray.
Occlusal/bite registration depends on clinical conditions. When possible, the maximum intercuspation serves as reference. Otherwise, the retruded contact position defined at the time of prosthetic planning would be transferred.
The cast was then prepared with the abutment replica and mounted on an articulator by the dental laboratory. The abutments with winglets were arranged in order to create the frame. These abutments were designed to be flexible in the horizontal direction, facilitating their shaping into the arch form. The height of the winglet provides great rigidity in the vertical direction. Winglets are adjusted in height when necessary in relation to the prosthetic
space available. The frame is then finished using laser welding to join the winglets together (Figure 4a and 4b). A rigid milled titanium frame is thus obtained without using an outside milling center. This frame has the same advantages with respect to abutment adjustments and metal quality as those obtained with a casting technique. Although it was not our choice in this case, it is also possible to bind the winglets together with resin. To our knowledge no biomechanical evaluation of this type of assembly had been performed previously.
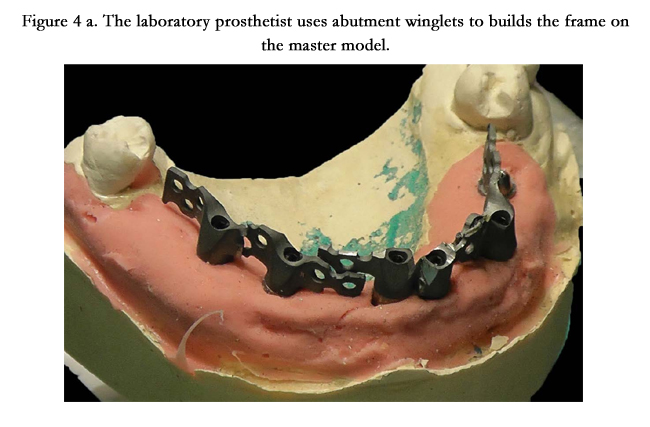

Figure 4 a. The laboratory prosthetist uses abutment winglets to builds the frame on the master model.
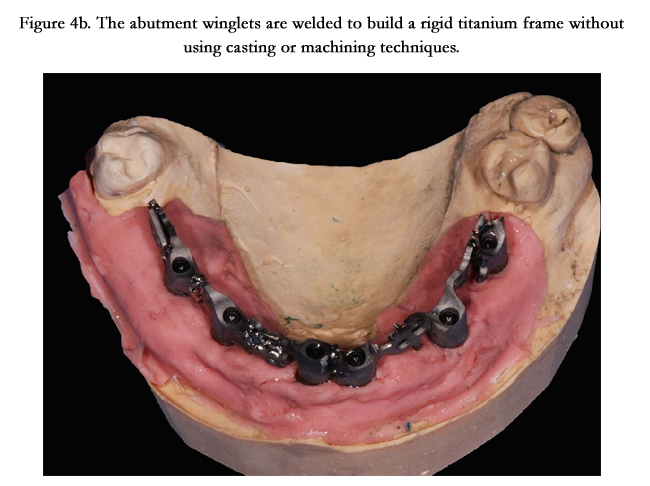

Figure 4b. The abutment winglets are welded to build a rigid titanium frame without using casting or machining techniques.
Before setting up the denture teeth, the metal of the frame metal was covered by an opaque layer which facilitated resin adhesion.Teeth were then mounted according to the validated diagnostic set-up: after wax removal, teeth were fixed on the frame with, in this case, a self-polymerized resin, and set in the mouth (Figure 5 and 6).
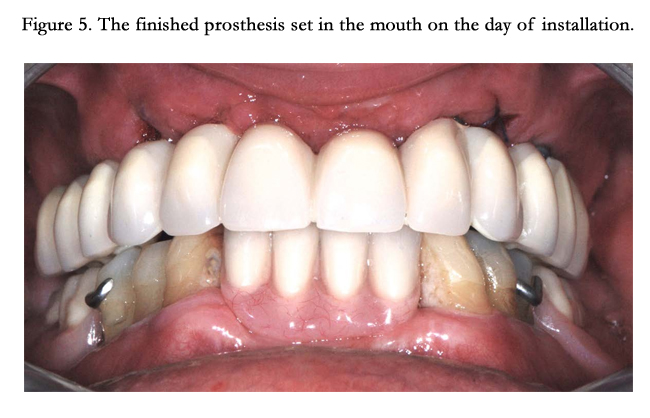

Figure 5. The finished prosthesis set in the mouth on the day of installation.
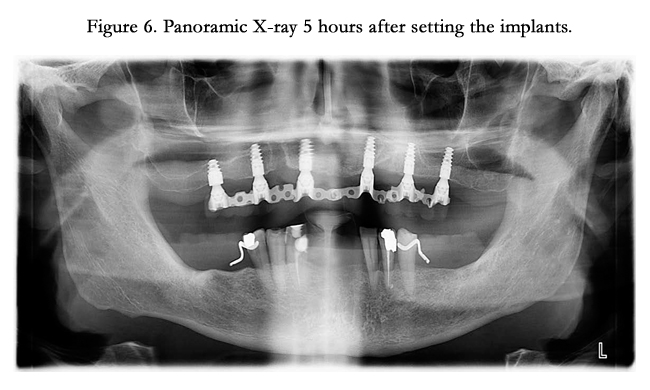
Figure 6. Panoramic X-ray 5 hours after setting the implants.
Discussion
This “all in bar” procedure has many advantages. Firstly, it can ensure frame passivity when used in immediate loading on a complete prosthesis, although during screwing of the prosthesis, it is possible for the implants to move slightly and reposition themselves according to the rigid frame.
Secondly, implants are considered to have good primary stability when a rigid frame is used for immediate loading [8, 9]. So far, the literature has suggested binding the implants together with a resin frame. However, the elasticity coefficient of this frame remains much higher than that of a metallic frame, which leads practitioners to use a titanium frame despite the 48 to 72 hours waiting time necessary before setting up the prosthesis. The “all in bar” frame containing abutments with winglets retained the same rigidity properties for implant stability during the bone healing phase while considerably reducing the time between implant placement and loading.
Furthermore, using abutments with winglets avoided titanium casting, a delicate step requiring good expertise from the dental laboratory technician. A second advantage is the fact that frame milling can be done internally and does not involve an outside center, which would require more time and increase costs.
Abutments with slim winglets contained perforations at their extension with a diameter large enough to allow covering the metal by the resin and should reinforce resistance to fracture. Furthermore, this resistance will increase if the screwing pits are on the lingual or palatal side, as the resin would have more space between the bar and the prosthetic teeth. This could lead to reducing the number of resin fractures which are usually frequent in this type of procedure. This hypothesis remains to be proven during the prosthetic follow-up.
For patients, the placement of implants and setting-up of the prosthesis could take place within the same day. In the case of a post-extractional immediate loading procedure, patients would only be toothless for a few hours. Whatever the case, they would benefit from the comfort of having a fixed prosthesis rapidly without wearing a transitional denture, thus favoring good osteointegration.
Finally, using winglet abutments allows any dental laboratory to rapidly prepare implant supported complete overdentures with a rigid frame. We think that it is better to use a laser welder under an argon atmosphere. Nevertheless, satisfying results are also obtained when resin is used to bind the winglets to each other.
Conclusion
The advantages of such a procedure would be to reduce the toothless period of patients while providing the excellent implant stability required for good osseointegration.
Furthermore, frames would be prepared at a very competitive cost that would facilitate greater public access to implant supported prosthetic treatments.
However, increased attention should be paid by the dental surgeon to the placement of the implants inside the prosthetic volume and preferably perpendicular to the occlusion plane, in order to ensure esthetic and functional outcomes, as well as sustainable restorations.
References
- Albrektsson T, Brånemark PI, Hansson HA, Lindström J (1981) Osseointegrated titanium implants. Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop Scand 52(2): 155-170.
- Brunski JB, Moccia AF Jr, Pollack SR, Korostoff E, Trachtenberg DI (1979) The influence of functional use of endosseous dental implants on the tissueimplant interface. I. Histological aspects. J Dent Res 58(10): 1953-1969.
- Schnitman PA, Wohrle PS, Rubenstein JE (1990) Immediate fixed interim prostheses supported by two-stage threaded implants: Methodology and results. J Oral Implantol 16(2): 96-105.
- Roccuzzo M, Bunino M, Prioglio F, Bianchi SD (2001) Early loading of sandblasted and acid-etched (SLA) implants: a prospective split-mouth comparative study. Clin Oral Implants Res 12(6): 572-578.
- Rismanchian M(1), Attar BM, Razavi SM, Shamsabad AN, Rezaei M (2012) Dental implants immediate loading versus the standard 2-staged protocol: an experimental study in dogs. J Oral Implantol 2012 38(1): 3-10.
- Drago CJ, Lazzara RJ (2006) Immediate occlusal loading of Osseotite implants in mandibular edentulous patients: a prospective observational report with 18-month data. J Prosthodont 15(3): 187-194.
- Degidi M, Nardi D, Piattelli A (2013) A six-year follow-up of full-arch immediate restorations fabricated with an intraoral welding technique. Implant Dent 22(3): 224-231.
- Degidi M, Daprile G, Piattelli A (2012) Implants inserted with low insertion torque values for intraoral welded full-arch prosthesis: 1-year follow-up. Clin Implant Dent Relat Res 14 Suppl 1: e39-45.
- Ghoul WE, Chidiac JJ (2012) Prosthetic requirements for immediate implant loading: a review. J Prosthodont 21(2): 141-154. doi: 10.1111/j.1532-849X.2011.00819.x.





