Ketofol as a Balanced Anesthetic for Procedural Sedation and Analgesia (PSA) in the Obese Oral Surgery Patient: a Commentary
Lee KC1*, Lee BC2
1 College of Dental Medicine, Columbia University, New York, USA.
2 Resident, Department of Anesthesiology, Columbia University Medical Center, New York, USA.
*Corresponding Author
Kevin C. Lee, BA,
College of Dental Medicine,
Columbia University, 622 W 168th Street,
New York, NY 10032, USA.
Tel: 3014424571
Email: kcl2136@cumc.columbia.edu
Received: January 13, 2016; Accepted: February 09, 2016; Published: February 10, 2016
Citation: Lee KC, Lee BC (2016) Ketofol as a Balanced Anesthetic for Procedural Sedation and Analgesia (PSA) inthe Obese Oral Surgery Patient: a Commentary. Int J Dentistry Oral Sci. 03(2), 190-192. DOI : dx.doi.org/10.19070/2377-8075-1600040
Copyright: Lee KC© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
A hallmark of oral and maxillofacial surgery is the administration of sedation and general anesthesia in the office setting. As part of their training, oral surgeons are required to function as anesthesia residents for a minimum of 5 months with commensurate levels of responsibility. The oral surgeon treats a variety of patients and must take increasing care to avoid and manage any untoward anesthetic events. “Ketofol” is a moniker for ketamine and propofol administered either independently or as a single-syringe admixture. Ketofol is hypothesized to possess the ideal profile for sedation because of the balance provided by both agents. This commentary aims to present the risks and benefits of ketofol and apply this knowledge to a patient population who may benefit the most from the combination.
2.Commentary
3.Acknowledgements & Declarations
4.References
Keywords
Ketamine; Propofol; Ketofol; Sedation Dentistry; Dental Anesthesia.
Commentary
The goal of moderate “conscious sedation” is to achieve muscular relaxation and analgesia while simultaneously maintaining both a purposeful response to verbal commands and spontaneous ventilation without the need for ventilatory support. Although body mass index (BMI) is not necessarily correlated with postoperative complications in dentoalveolar surgery [1], that does not mean that care should not be taken to closely evaluate and monitor the obese patient perioperatively. As a consequence of body habitus, obesity is a condition that may present with a variety of cardiorespiratory comorbidities including but not limited to extrinsic restrictive lung disease, upper airway obstruction, and decreased tolerance to hemodynamic instability [2, 3]. This poses a dilemma for the oral surgeon because some of the most commonly used agents for procedural sedation and analgesia (PSA) promote pharyngeal collapse, decrease respiratory drive, and depress hemodynamic parameters.
“Ketofol” is a moniker for ketamine and propofol administered either independently or as a single-syringe admixture. Ketofol has been advocated as the ideal PSA combination because the need for lower doses of each agent combined with the opposing actions of both agents theoretically decreases the incidence of dose-related side effects (Table 1). No single PSA agent is ideal for every situation encountered in the management of morbidly obese patients [4]. Therefore, PSA for obese patients should be achieved through balanced sedation. Propofol is a general anesthetic that acts at the GABA-B receptor to enhance chloride ion channel activity. It is favored in the outpatient setting because of its rapid onset and short duration of action [5]. In sedating doses, propofol produces adequate amnesia and has been shown to have antiemetic properties. The primary disadvantages of propofol are that it depresses both mean arterial blood pressure and respiratory drive in a dose-dependent manner. In addition, propofol’s inability to provide analgesia prevents it from being the sole anesthetic medication for any stimulating procedure. Ketamine is a dissociative anesthetic that is thought to produce its effects primarily through noncompetitive inhibition of the NMDA receptor. Like propofol, it provides amnesia in a dose-dependent manner, but has the added benefits of analgesia and preservation of respiratory and airway reflexes. The primary disadvantages of ketamine are that it can induce sympathomimetic reactions, raise intracranial pressures, and worsen nausea/emesis. At higher doses or with rapid infusions, ketamine can paradoxically cause respiratory depression, but this effect is generally uncommon when used for PSA. Ketamine is also classically associated with a frightening emergence phenomenon that is thought to occur more commonly in adults as a result of its structural resemblance to phencyclidine (PCP). However, both midazolam and propofol may be used to treat or prevent this phenomenon. Therefore, it would follow that ketofol should offer the benefits of both agents, while reducing the adverse effects of either agent alone. This is especially important in obese patients where fluctuations in hemodynamic parameters may not be tolerated and where decreased muscle tone in the supine position may collapse soft tissues of the oropharynx, leading to rapid hypoxia in this patient population with an already reduced functional residual capacity (FRC).
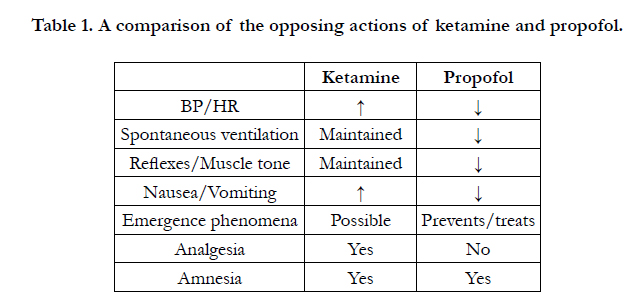

Table 1. A comparison of the opposing actions of ketamine and propofol.
Much of the evidence supporting ketofol in PSA arises from the emergency medicine literature because it is often necessary to perform painful procedures efficiently and humanely in the emergency department (ED) [6]. Two studies have been published in the oral surgery literature on ketofol. Cillo [7] found that for outpatient dentoalveolar surgery continuous IV infusions of 10:1 propofol-ketamine ratio adequately maintained hemodynamic stability and produced a faster recovery time than both 5:1 and 3:1 ratios. Kramer et al [8] reported that, compared to ketofol, continuous infusions of propofol-remifentanil demonstrated similar sedation and hemodynamic/respiratory profiles with the added benefit of a shorter recovery time. Kramer et al [8] conducted their study on American Society of Anesthesiologists (ASA) class I and II adults and therefore their population may not represent those who might benefit the most from ketofol. The hemodynamic effects of ketofol are clinically unimportant in healthy patients because the observed blood pressure differences are trivial [9, 10] and do not alter ED interventions for hypotension [10, 11]. Propofol-induced hypotension is essentially always transient in patients without serious underlying disease [9, 10]. In oral surgery, propofol is an extensively used sedative agent while ketamine is infrequently used in adults and often reserved for its analgesic and sympathomimetic properties. Additionally, remifentanil is typically preferred when further analgesia is desired. PSA is appropriate for ASA classes I, II, and III, while patients of classes ≥ IV are likely better suited for treatment in the operating room [12]. However, this does not contraindicate PSA for all obese patients. In obese patients infused with propofol, the oral surgeon may consider titrating ketamine as an analgesic alternative to remifentanil not only because of the theoretical benefits to airway reflex, respiratory drive, and hemodynamic stability, but also because the prolonged analgesic effects of ketamine will last throughout the immediate postoperative period.
In summary, there is insufficient evidence in the oral surgery literature to conclude that ketofol is superior to either agent alone or either agent used in combination with a different agent. Oral surgeons using ketofol may prefer separate syringes versus admixtures of ketofol because of the ability to finely titrate propofol and ketamine independently. The use of ketofol is not without its risks. PSA doses of ketamine are typically not sufficient to cause respiratory depression. However, when either ketamine or ketofol is administered as a bolus, the risk of respiratory depression increases. Mittal et al [13] found that ketofol, when bolused for PSA, produced a greater incidence of respiratory depression than propofol alone. In that study, the relatively rapid dosing regimen of ketamine possibly offset any protective effect provided by the reduction in total propofol usage. Alternatively, it may be that such a protective effect does not exist [14]. Although a systemic review of the emergency medicine literature suggests that ketofol does indeed improve cardiorespiratory stability and is an appropriate substitute for propofol, more research is needed confirm the consistency of these findings [15]. The majority of the existing evidence on ketofol has been gathered from healthy pediatric populations. Future studies enrolling obese adults, who are prone to the adverse effects of sedation agents and who may benefit the most from ketofol, are needed. Additionally, the optimal dosing regiment and ratio of ketofol still require investigation.
Ketofol is hypothesized to possess the ideal profile for sedation. Olson et al [16] demonstrated that among anesthesia providers one of the primary barriers to using ketofol was a lack of education. The combination of ketofol is one that is relatively new and unconventional, but with the proper education and guidelines may see an increase in use.
Acknowledgements & Declarations
No funds were received in support of this work. No benefits in any form have been or will be received from any commercial party related directly or indirectly to the subject of this manuscript.
References
- Waisath TC, Marciani RD, Waisath FD, James L (2009) Body mass index and the risk of postoperative complications with dentoalveolar surgery: a prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol 108(2): 169-173.
- Joshi GP, Ahmad S, Riad W, Eckert S, Chung F (2013) Selection of obese patients undergoing ambulatory surgery: a systematic review of the literature. Anesth Analg 117(5): 1082-1091.
- Tsai A, Schumann R (2016) Morbid obesity and perioperative complications. Curr Opin Anaesthesiol 29(1): 103-108.
- Aantaa R, Tonner P, Conti G, Longrois D, Mantz J, et al. (2015) Sedation options for the morbidly obese intensive care unit patient: a concise survey and an agenda for development. Multidiscip Respir Med 10(1): 8.
- Casagrande AM (2006) Propofol for office oral and maxillofacial anesthesia:the case against low-dose ketamine. J Oral Maxillofac Surg 64(4): 693-695.
- Godwin SA, Caro DA, Wolf SJ, Jagoda AS, Charles R, et al. (2005) Clinical policy: procedural sedation and analgesia in the emergency department. Ann Emerg Med 45(2): 177-196.
- Cillo JE Jr (2012) Analysis of propofol and low-dose ketamine admixtures for adult outpatient dentoalveolar surgery: a prospective, randomized, positive- controlled clinical trial. J Oral Maxillofac Surg 70(3): 537-546.
- Kramer KJ, Ganzberg S, Prior S, Rashid RG (2012) Comparison of propofol- remifentanil versus propofol-ketamine deep sedation for third molar surgery.Anesth Prog 59(3): 107-117.
- Miner JR, Moore JC, Austad EJ, Plummer D, Hubbard L, et al. (2015) Randomized, double-blinded, clinical trial of propofol, 1:1 propofol/ketamine, and 4:1 propofol/ketamine for deep procedural sedation in the emergency department. Ann Emerg Med 65(5): 479-488.e2.
- Green SM, Andolfatto G, Krauss BS (2015) Ketofol for procedural sedation revisited: pro and con. Ann Emerg Med 65(5): 489-491.
- Andolfatto G, Abu-Laban RB, Zed PJ, Staniforth SM, Stackhouse S, et al. (2012) Ketamine-propofol combination (ketofol) versus propofol alone for emergency department procedural sedation and analgesia: a randomized double-blind trial. Ann Emerg Med 59(6): 504-512.e1-2.
- American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists (2002) Practice Guidelines for Sedation and Analgesia by Non-Anesthesiologists. Anesthesiology 96(4): 1004-1017.
- Mittal N, Goyal A, Gauba K, Kapur A, Jain K (2013) A double blind randomized trial of Ketofol versus propofol for endodontic treatment of anxious pediatric patients. J Clin Pediatr Dent 37(4): 415-420.
- David H, Shipp J (2011) A randomized controlled trial of Ketamine/propofol versus propofol alone for emergency department procedural sedation. Ann Emerg Med 57(5): 435-441.
- Jalili M, Bahreini M, Doosti-Irani A, Masoomi R, Arbab M, et al. (2016) Ketamine-propofol combination (ketofol) vs propofol for procedural sedation and analgesia: systematic review and meta-analysis. Am J Emerg Med.
- Olson AN, Rao WR, Marienau ME, Smischney NJ (2015) Period Prevalence of Ketamine-Propofol Admixture "Ketofol" in the Operating Room among Anesthesia Providers at an Academic Medical Center. Med Sci Monit 21: 1737-1744.





