Buccal Bifurcation Cyst: A Diagnosis Not to Miss
Omami G*, Firas Al Yafi
1 Assistant Professor, Department of Oral Health Practice, University of Kentucky College of Dentistry, Rose Street, Lexington, KY, USA.
2 Fellow, Periodontology and Implantology, University of Kentucky College of Dentistry, Rose Street, Lexington, KY, USA.
*Corresponding Author
Galal Omami,
Assistant Professor,
Department of Oral Health Practice,
University of Kentucky College of Dentistry, USA.
Tel: (859) 323-8901
Fax: (859) 323-9136
Email: Galal.Omami@uky.edu
Received: December 02, 2015; Accepted: January 02, 2016; Published: January 05, 2016
Citation: Omami G, Firas Al Yafi (2016) Buccal Bifurcation Cyst: A Diagnosis Not to Miss. Int J Dentistry Oral Sci. 03(1), 181-184.DOI : dx.doi.org/10.19070/2377-8075-1600038
Copyright: Omami G© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
2.Case Report
3.Discussion
4.Differential Diagnosis
4.1.Periodontal abscess
4.2.Radicular cyst
4.3.Dentigerous cyst
4.4.Langerhans’ cell histiocytosis
5.Conclusion
6.References
Introduction
Buccal bifurcation cyst (BBC) is a rare odontogenic cyst of unknown etiology. It typically develops on the buccal aspect of the permanent mandibular first and second molars in younger patients (8 to 16 years old). Common clinical signs are the lack of or a delay in eruption of a mandibular first or second molar, swelling in the affected mandibular molar region, and an increase in periodontal pocket depth. Specific radiographic features include a radiolucent lesion on the buccal aspect of the tooth, tilting of the involved molar, and periosteal reaction on the buccal surface. However, the histopathologic features are inconclusive. In this report, we present a case of BBC with special emphasis on the characteristic radiographic features and differential diagnosis.
Case Report
A 15-year-old boy presented to the Urgent Care Clinic of the University of Kentucky College Of Dentistry, Lexington, with a chief complaint of a 2-day history of pain associated with mild fever and swelling on the lower right side of the face. Patient’s medical history was negative. On extraoral examination, there was a localized, firm and tender swelling of the right lower cheek. The overlying skin looked slightly erythematous. Intraoral examination was remarkable for partially erupted mandibular right second molar with the only lingual cusps tips protruding through the apparently inflamed overlying mucosa; however, the contralateral second molar was fully erupted. No carious cavity was clinically detected, however, the tooth was tender to percussion. The buccal probing depth was 11 mm with no purulent discharge. As the tooth was partially erupted with acute local inflammation, it was not possible to assess the vitality. No lip paresthesia was reported. On initial panoramic examination, there was a well-defined round corticated unilocular radiolucent lesion associated with the roots of the second molar (Figure 1). Cone-beam CT imaging showed the lesion had caused expansion and perforation of the buccal cortical plate associated with periosteal new bone formation, it has also caused lingual tipping of the second molar roots (Figures 2, 3, 4). The overall estimated dimensions were 18 x 12 x 14 mm.
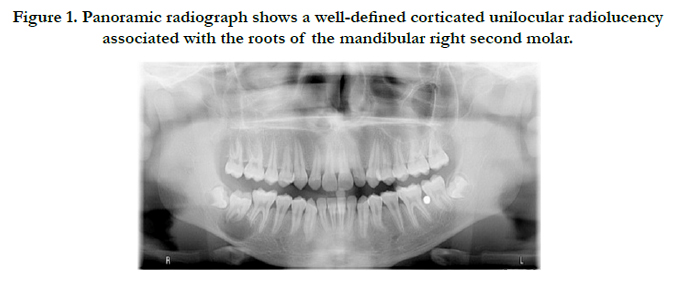

Figure 1. Panoramic radiograph shows a well-defined corticated unilocular radiolucency associated with the roots of the mandibular right second molar.
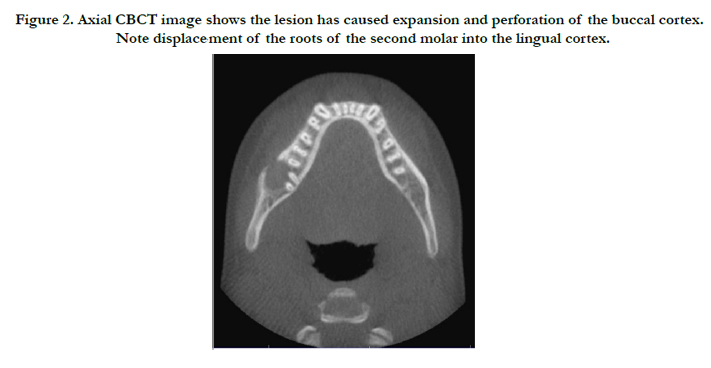
Figure 2. Axial CBCT image shows the lesion has caused expansion and perforation of the buccal cortex. Note displacement of the roots of the second molar into the lingual cortex.
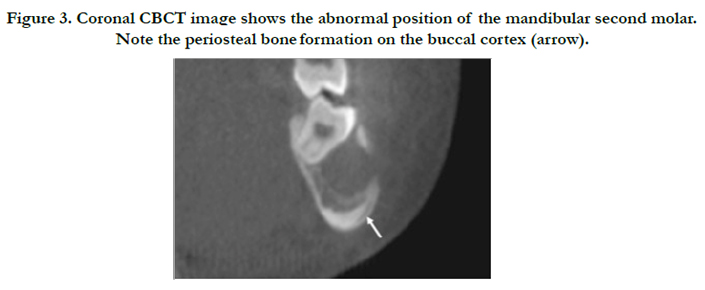
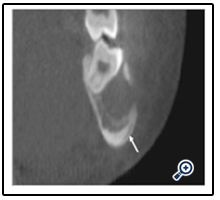
Figure 3. Coronal CBCT image shows the abnormal position of the mandibular second molar. Note the periosteal bone formation on the buccal cortex (arrow).
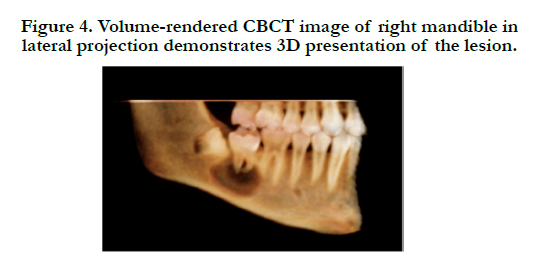

Figure 4. Volume-rendered CBCT image of right mandible in lateral projection demonstrates 3D presentation of the lesion.
Discussion
The 1992 WHO Histological Typing of Odontogenic Tumors defined the buccal bifurcation (paradental, inflammatory collateral, mandibular infected buccal) cyst as an inflammatory odontogenic cyst arising on the lateral aspect of a vital tooth as a result of an inflammatory process in the periodontal pocket [1]. The pathogenesis of BBC is unclear, however, it has been suggested that BBC is derived from the epithelial cell rests of Malassez in the periodontal membrane of the buccal bifurcation of the mandibular molars. The etiology of cystic degeneration is unknown, however, inflammation is believed to be the stimulus. BBC represents 3.0% of all cysts of the jaws and 3.7% of odontogenic cysts [2]. Lesions most often presenting a few years after the eruption of the associated tooth with slight male predominance [3]. They typically affect the permanent mandibular first and second molar teeth although third molar may also be affected. However, the first molar is involved more frequently than second molar. Bilateral lesions have been reported in 26% of all BBC cases [4]. A common sign is the lack or delayed eruption of the associated tooth, however, swelling is the most likely clinical presentation. The involved tooth is vital, a sign which rules out a radicular cyst. Radiographically, the lesion is often superimposed on the buccal root bifurcation as well-demarcated unilocular radiolucency, often with a corticated margin. The periodontal ligament space is not widened and the lamina dura is intact around the roots. Buccal expansion usually is apparent. If the cyst is secondarily infected, periosteal new bone formation is seen on the adjacent buccal cortex. The associated tooth is usually tilted so that the apices are displaced into the lingual cortical plate and the occlusal surface toward the buccal aspect. This accounts for the lingual cusps tips being positioned higher than the buccal tips, this finding that is best illustrated on occlusal projections [5]. Histologically, the cyst is indistinguishable from the radicular cyst [6]. However, the diagnostic features are the young age of the patients, the mandibular molar site, the buccal periostitis, the vital pulp, the continuity of the apical lamina dura and the tipping of the involved tooth.
Enucleation of the cyst with preservation of the associated tooth is the treatment of choice [7]. However, periodontal probing with daily irrigation of the buccal pocket (i.e., micro-marsupialization) has been successfully reported for small lesions [8]. Spontaneous resolution has also been reported [9]. BBCs don’t tend to recur.
Differential Diagnosis
Periodontal abscess is a localized purulent inflammation in the soft tissue wall of a deep periodontal pocket. It occurs more often in molar sites [10]. Periodontal abscess formation is usually due to the marginal closure of a deep periodontal pocket that prevents proper drainage, or a foreign body impaction into a previously healthy periodontal tissues. However, it sometimes arises in preexisting periodontal disease due to subgingival flora and host resistance alterations especially in diabetic patients [10]. The clinical symptoms of acute lesion include severe pain, swelling/tenderness of the surrounding gingiva, sensitivity of the affected tooth to percussion and increased tooth mobility. The involved tooth is typically vital unless complicated by a perio-endo lesion. The abscess usually drains through the pocket opening or less often through a fistula. The radiographic examination is ranging from a normal appearance of the interdental bone (acute lesions), a widening of the periodontal ligament space, to a well-defined area of bone loss over the midroot region of the tooth. Periodontal abscess is treated by thorough scaling and root debridement with soft tissue curettage.
Radicular cysts are the most common cysts of the jaws and arise from the epithelial remnants in the periodontal ligament as a result of periapical periodontitis following necrosis of the pulp. Lesions are located most commonly at the apices of the involved teeth (apical radicular cyst), but may also be found on the lateral aspects of the roots in relation to lateral accessory root canals (lateral radicular cyst). Furthermore, a radicular cyst which continues to grow in the jaw after removal of the offending tooth is referred to as residual radicular cyst. Most radicular cysts are found in the anterior maxilla [11]. They usually are asymptomatic unless secondarily infected. The associated tooth is essentially nonvital. Radiographically, the outline of a radicular cyst usually is curved or circular reflecting the intracystic osmotic pressure. The periphery typically has a well-defined cortical border continuous with the lamina dura around the associated tooth. If a radicular cyst is large, cortical expansion, displacement and resorption of the roots of adjacent teeth may occur. A radicular cyst is surgically enucleated with extraction or endodontic treatment of the associated tooth.
A dentigerous cyst is one that encloses the crown of an unerupted tooth by expansion of its follicle, and is attached to its cementoenamel junction. It is the most common developmental odontogenic cyst, accounting for about 20% of all cysts of the jaws [12]. The pathogenesis of this cyst is uncertain, but apparently it develops by accumulation of fluid between the reduced enamel epithelium and the tooth crown. The most common site is mandibular third molar region followed by maxillary permanent canine, mandibular premolars, and maxillary third molars. Dentigerous cysts are often asymptomatic and are incidentally discovered during routine radiographic examination most frequently in patients between 10 and 30 years of age [12]. Radiographically, a dentigerous cyst typically has a well-defined cortex with a curved or circular outline reflecting its expensile growth pattern. The internal aspect is completely radiolucent except for the crown of the involved tooth. It has a propensity to displace and resorb adjacent teeth. Three radiological variations of dentigerous cyst may be recognized. The central variant where the crown is enveloped symmetrically, the lateral type in which the cyst appears on one aspect of the crown, and the circumferential variant as the entire tooth appears to be enveloped by cyst. Dentigerous cysts are treated by surgical enucleation along with removal of the unerupted tooth. Large cysts may be treated by marsupialization before enucleation.
Langerhans’ Cell Histiocytosis (LCH) is a spectrum of disorders characterized by proliferation of Langerhans cells that are accompanied by varying numbers of eosinophils, lymphocytes, plasma cells, and multinucleated giant cells. However, LCH is currently regarded as a myeloid neoplasm [13]. The spectrum of LCH includes the eosinophilic granuloma of bone (solitary or multiple), Hand-Schüller-Christian disease (chronic disseminated) and Letterer- Siwe disease (acute disseminated). Eosinophilic granuloma (EG) of bone occurs most often in teenagers [14]. In the jaws, the disease may cause painful bony swelling, a soft tissue mass, and bone destruction. Gnathic lesions occur most often in the posterior mandible. However, alveolar lesions commonly start in the midroot region of the teeth. Radiographically, EG appear as well defined, non-corticated, radiolucent lesions. As bone destruction progresses in a circular shape, it may give the impression that a segment of the alveolar process has been scooped out; as a result, the teeth appear to be standing in air “floating teeth’. However, the lesion does not displace teeth. Periosteal new bone may be laid down, either as a single linear band or laminated if there are multiple layers [15]. Surgical curettage of EG can provide local control of the disease.
Conclusion
BBC typically occurs in the buccal furcal area of an erupting permanent mandibular first and second molar teeth. The diagnosis is established by correlation of clinical and radiographic findings. The pathognomic sign of a BBC is the tipping of the involved tooth so that the root tips are pushed into the lingual cortical plate of the mandible and the occlusal surface is tipped toward the buccal aspect. Surgical enucleation of the cyst with maintenance of the involved tooth is the treatment of choice. Therefore, knowledge of the characteristic features of BBC is important for proper diagnosis and management. This article should be a useful reference and learning aid for dentists and dental students.
References
- Kramer IR, Pindborg JJ, Shear M (1992) Histological typing of odontogenic tumors. World Health Organization. (2nd edtn), Springer, Berlin. 40.
- Shear M, Speight P (2007) Cyst of the oral and maxillofacial regions. (4th edtn), Wiley-Blackwell, US. 143.
- Philipsen HP, Reichart PA, Ogawa I, Suei Y, Takata T (2004) The inflammatory paradental cyst: a critical review of 342 cases from a literature survey, including 17 new cases from the author’s files. J Oral Pathol Med 33(3): 147-155.
- Corona-Rodriguez J, Torres-Labardini R, Velasco-Tizcareno M, Mora- Rincones O (2011) Bilateral buccal bifurcation cyst: case report and literature review. J Oral Maxillofac Surg 69(6): 1694-1696.
- White SC, Pharoah MJ (2014) Oral Radiology: Principles and Interpretation. (7th edtn), Elsevier, Canada. 338.
- Neville B, Damm DD, Allen CM, Chi AC (2015) Oral and maxillofacial pathology. (4th edtn), WB Saunders, Philadelphia. 712.
- Shohat I, Buchner A, Taicher S (2003) Mandibular buccal bifurcation cyst: enucleation without extraction. Int J Oral Maxillofac Surg 32(6): 610-613.
- Lizio G, Corinaldesi G, Bianchi A, Marchetti C (2011) Successful resolution of juvenile paradental cysts after marsupialization in five consecutive patients. Aust Dent J 56(4): 427-432.
- Zadik Y, Yitschaky O, Neuman T, Nitzan DW (2011) On the Self-Resolution Nature of the Buccal Bifurcation Cyst. J Oral Maxillofac Surg 69(7):e282-284.
- Herrera D, Roldan S, Sanz M (2000) The periodontal abscess: a review. J Clin Periodontol 27(6): 377-386.
- Shear M (1985) Cysts of the jaws: recent advances. J Oral Pathol 14(1): 43-59.
- Shear M (1994) Developmental odontogenic cysts. An update. J Oral PatholMed 23(1): 1-11.
- El Demellawy D, Young JL, de Nanassy J, Chernetsova E, Nasr A (2015) Langerhans cell histiocytosis: a comprehensive review. Pathology 47(4): 294-301.
- Bartnick A, Friedrich RE, Roeser K, Schmelzle R (2002) Oral Langerhans cell histiocytosis. J Cranio-maxillofac Surg 30(2): 91-96.
- Dagenais M, Pharoah MJ, Sikorski PA (1992) The radiographic characteristics of histiocytosis X. A study of 29 cases that involve the jaws. Oral Surg Oral Med Oral Pathol 74(2): 230-236.





