Salivary Biomarkers in Caries Affected and Caries Free Children
El-kwatehy WM1,2, Youssef AR3,4*
1 Department of Community Dentistry, Faculty of Dentistry, Mansoura University, Egypt.
2 Department of Preventive Dentistry, Faculty of Dentistry, Umm Al-Qura University, Saudi Arabia.
3 Department of Microbiology and Immunology, Faculty of Medicine, Suez Canal University, Egypt.
4 Department of Basic and Clinical Oral Sciences, Faculty of Dentistry, Umm Al-Qura University, Saudi Arabia.
*Corresponding Author
Abdel-Rahman Youssef,
Department of Microbiology and Immunology,
Faculty of Medicine, Suez Canal University, Egypt.
E-mail: armyoussef@yahoo.com
Received: September 05, 2016; Accepted: October 22, 2016; Published: October 26, 2016
Citation: El-kwatehy WM, Youssef AR (2016) Salivary Biomarkers in Caries Affected and Caries Free Children. Int J Dentistry Oral Sci. 3(10), 348-352. doi: dx.doi.org/10.19070/2377-8075-1600071
Copyright: Youssef AR© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Dental caries is a major health problem among school children. Antimicrobial peptides (AMPs) in saliva are part of host innate immunity. AMPs may play a significant role in defense or vulnerability to dental caries.
Objective: The aim of this study was to evaluate the relationship between different salivary biomarkers and caries risk assessment.
Methods: Oral examinations were performed on 80 school children. Unstimulated whole saliva was collected from 40 caries-free and 40 caries-affected children to evaluate the saliva flow rate, pH, total protein concentration, total antioxidant, α-defensin and cariogenic microorganisms.
Results: There were significant differences between caries free and caries affected children in relation to salivary pH and α-defensin. In addition, the percentage of children with streptococcus mutans or lactobacilli ≥ 105 cfu/ml was significantly higher in caries affected children compared to caries free children. However, there were no significant differences between the two groups regarding to saliva flow rate, total protein and total antioxidant.
Conclusion: Children with caries experience had low levels of α-defensin and salivary pH and greater numbers of streptococcus mutans and lactobacilli. These findings could lead to new tools to screen and assess caries susceptibility in children.
2.Introduction
3.Materials and Methods
3.1.Subjects
3.2.Saliva Samples
3.3.Salivary streptococcus mutans and lactobacill Levels Assessment
3.4.Protein and Antioxidant Assessment
3.5.Antimicrobial Peptide (α-defensin) Asessment
3.6.Statistical Analysis
4.Results
4.1.α-defensin
4.2.Salivary pH and Flow Rate
4.3.Salivary Total Protein and Total Antioxidant
4.4.Salivary streptococcus mutans and lactobacill Levels
5.Discussion
6.Acknowledgements
7.References
Keywords
Caries; Streptococcus Mutans; Lactobacilli; Salivary Biomarkers; α-Defensin.
Introduction
Saliva plays a crucial role in the health of the mouth and any changes in quantity or quality of saliva may affect the oral health status. It is generally accepted that saliva play an important role in the pathogenesis of dental caries [1, 2]. Whole human saliva contains arrays of immunoglobulin and non immunoglobulin defense factors. The major components of the non immunoglobulin group are antimicrobial peptides (AMPs), antioxidant, lysozyme, lactoferrin, agglutinins, histidine rich protein and anionic protein [3, 4].
Several studies have investigated the correlation between concentrations of the predominant protein components in saliva and dental caries [5-10]. Mandel et al., [5], found no difference in parotid saliva proteins identified by paper electrophoresis between caries-resistant and caries-active adults. Conversely, Balekjian et al., [6] using gel electrophoresis found that a caries-rampant group exhibited a significant reduction in the proportion of cationicmigrating proteins and a significant increase in amylase compared with a caries-resistant group. Although the results of these studies are inconclusive, there is evidence that similar proteins in saliva from caries-active and caries-free persons may have different levels of biological activity [10].
Saliva flow rate is considered a potential risk factor when the unstimulated salivary flow rate is lower than 0.30 mL/min [11-13].
However, some investigators found no correlation between salivary flow rates or pH and dental caries [14, 15].
The development of dental caries may be affected by disparity between free radicals levels and antioxidants in saliva. Antioxidants combat the adverse effects of any reaction that cause excessive oxidations by neutralizing the toxicity of free radicals and cytokines, and reduction in antioxidant levels leads to oxidative stress [16].
It has been shown that total protein and total antioxidant in saliva increased with caries activity [15]. Moreover, a higher total antioxidant capacity (TAC) was observed with dental caries in deciduous but not in permanent teeth [17-20] and TAC increased with the age of the children [21, 22].
Defensins are important antimicrobial peptides in innate and adaptive immune response pathways [23]. The salivary α-defensins, a mixture of HNP1, 2, 3 (HNP1–3) are elevated in patients with oral inflammation [24]. Levels of HNP1–3 vary in healthy individuals ranging from undetectable to ~12 μg/ml [24, 25]. The presence of α- defensins in saliva is most likely derived from neutrophils and is a reflection of gingival or mucosal inflammation and loose or exfoliating teeth [26]. Several groups evaluated the possible correlation between caries prevalence in children and salivary concentrations of the antimicrobial peptides beta-defensin-3 (hBD-3), alpha-defensins HNP1-3 and the cathelicidin LL37 [26, 27]. They found that the median salivary levels of hBD-3, LL37, and HNP1-3 were in the microgram/ml range but were highly variable in the population. While levels of LL37 and hBD-3 did not correlate with caries experience, the median HNP1-3 levels were significantly higher in children with no caries than in children with caries. The low salivary levels of HNP1-3 may represent a biological factor that contributes to caries susceptibility and the possibility for using it as caries risk assessment tool, there have been relatively few studies assess the relationship between salivary α-defensin and its usage as a risk assessment tool, so the present study was carried out to determine the relationship between dental caries status and different salivary biomarkers including total protein, total antioxidant and α- defensin, salivary pH, saliva flow rate, levels of streptococcus mutans and lactobacill.
Materials and Methods
After receiving the written approval from the concerned school authorities and informed consent from the parents, a total of eighty healthy school children, from both genders (equal distribution), with an age ranging from 6 to 12 years old were selected to participate in this study. Children with systemic diseases, or those who were using any medications or mouth rinses during the last two months before saliva collection were excluded. The study population consists of 40 caries-free and 40 caries-affected individuals. The intra-examiner calibration was done by the researcher according to WHO Basic Method 1997 [28] to reduce the intra-examiner variability. Dental caries was scored according to World Health Organization criteria 1997 [28] using deft, defs, DMFT and DMFS indices [29-31].
Unstimulated whole saliva samples were collected as described previously by Chiappin et al., [32] to determine the salivary flow rate, pH, total protein, total antioxidant, antimicrobial peptide (α-defensin), streptococcus mutans and lactobacill levels. Subjects were instructed not to eat for one hour prior to the sampling. The saliva is allowed to droll into a clean container continuously for 5 minutes. The volume of unstimulated saliva was measured and the flow rate (ml/min.) was calculated. Salivary pH values were measured before storage of saliva using a hand–held pH meter according to manufacturer's instructions (HORIBA Ltd, Japan). 0.1% Nonidet P40 was added to each saliva sample and stored at – 80°C for further analysis.
The levels of streptococcus mutans and lactobacill were assessed before storage of saliva using CRT bacteria (Caries Risk Test) kits (Vivadent, Schaan Liechtenstein, Germay) according to manufacturer's instructions.
The total salivary protein level was measured by an autoanalyser (Technicon RAXT, USA) according to Biuret method [33]. The determination of the total antioxidant of saliva was performed by the reaction of antioxidants in the sample with a defined amount of exogenously provide hydrogen peroxide (H2O2) according to manufacturer's instructions (Biodiagnostic, Dokki, Giza, Egypt).
The antimicrobial peptide (α–defensin) level of the samples was measured by ELISA according to manufacturer's instructions (Hycult Biotechnology, Uden, The Netherland).
Data were analyzed using SPSS. Qualitative data were presented as numbers and percent while quantitative data were presented as mean ± standard deviation and tested for normality distribution by Kolmogorov–Smirnov test and found to be of parametric distribution, so independent t-test was used to compare between two groups for quantitative data, Chi – square test was used for comparison between groups for qualitative data, and Tow Way ANOVA test was used for comparison between dependant and independent variables, P< 0.05 was considered to be statistically significant [34].
Results
The level of α-defensin in the saliva was measured to investigate its correlation with caries (Table 1). We found that α-defensin was significantly higher in saliva of caries free children compared to caries affected children (p=0.041).
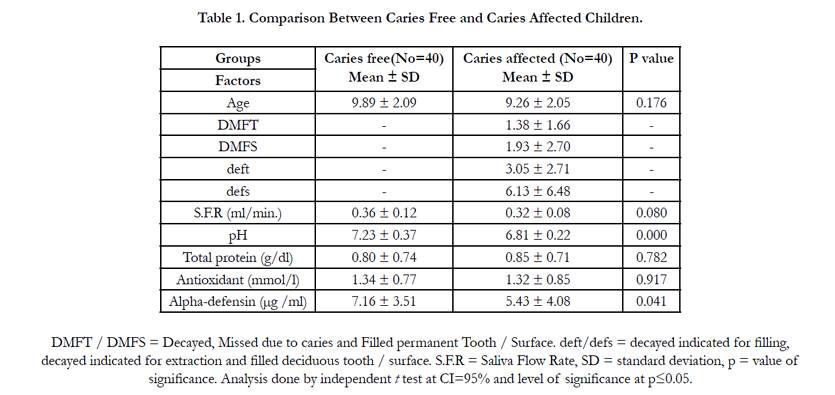

Table 1. Comparison Between Caries Free and Caries Affected Children.
salivary pH (Table 1) was significantly lower in caries affected children compared to caries free children (p =0.000) while saliva flow rate was comparable in both groups (p=0.080).
As can be seen in Table 1, both caries affected and caries free groups had similar level of total protein (p=0.782) and total antioxidant (P=0.917) and age was not contributing factor (p=0.176).
As can be seen in Figure 1, the percentage of children with streptococcus mutans or lactobacilli ≥ 105 cfu/ml was significantly higher in caries affected children compared to caries free children (p=0.000 for both).
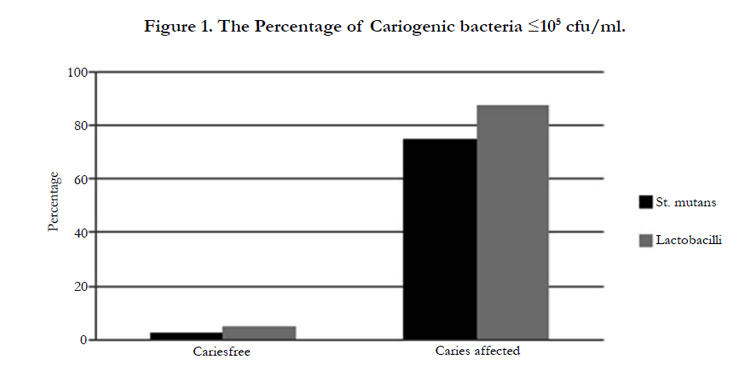
Figure 1. Percentage of Children with Cariogenic Bacteria ≥ 105 cfu/ml.
Discussion
Saliva is an important body fluid containing various microbes and host biological components that could be used for caries risk assessment. Currently, dental caries is mainly treated by restorative approaches, which do not always generate optimal satisfactory results. Caries risk assessment allows for the estimation of the probability of caries incidence, i.e., number of new cavities or incipient lesions in a certain time period, as well as the probability of the changes in the size or activity of caries lesions [35]. An accurate caries risk assessment can identify patients at high caries risk for preventive therapies and improved treatment effectiveness. Therefore, more attention has been given to this topic lately [36]. The collection of saliva samples is non-invasive, safe, and inexpensive. It seems likely that testing methods can be developed which can be used in dental practice to provide a foundation for the recognition of potential biomarkers of the disease [4]. Saliva flow rate is considered a potential risk factor when the unstimulated salivary flow rate is lower than 0.30 mL/min [11-13].
This study demonstrates that the salivary flow rate do not correlated to dental caries. This result is in agreement with previous studies [37, 38]. On contrast, other studies found that lower salivary flow rates play a significant role in caries development [39, 40].
In the present study we have shown that salivary pH was significant lower in caries affected children compared to caries free children (p =0.000). These results demonstrated that salivary pH can be used as indicator for caries risk assessment. Other studies support our finding as they have reported that larger quantities and faster rates of acid production in caries active individuals than that in caries-free individuals [41, 42]. There is strong evidence showing that salivary buffering capacity protects the tooth from dental caries [43] and low buffering capacity is usually associated with caries development because of its impaired neutralization of plaque acids and reduced remineralization of early enamel lesions [44-46]. This association between low caries levels and high salivary buffering capacity has been demonstrated [47, 48] and individuals with a high salivary buffer capacity are often cariesresistant [11].
Oxidative stress may play an important role in the onset and the development of several inflammatory oral pathologies and dental caries [49]. In the current study, salivary total antioxidant was not significantly higher in children with caries. Our result was similar to results of other studies. Preethi et al., [18] have shown that the role of salivary antioxidant in dental caries is less clear. In addition, Tulunoglu et al., [15] have shown non-significantly higher TAC in caries active children.
In the present study salivary total protein was higher in caries affected children compared to caries free children but the difference was statistically non significant. These findings were in agreement with Roa et al., [50] who found no difference in total protein levels between caries-free and caries-active adults. On contrast, Preethi et al., and Dodwad et al., [18, 51] have shown that total proteins were significantly higher in caries active in comparison to caries free children.
Salivary α-defensin is part of antimicrobial innate immunity. The results of the present study shows statistically significant higher concentration of α-defensin in caries free than caries affected children. Thus, this inverse correlation between α-defensin concentration and dental caries experience could be useful measure for caries risk assessment in children. Similar correlation was reported by previous studies [26, 27, 52]. On the contrary, Toomarian et al., [53] found no significant differences in α-defensins levels between childhood caries and caries free preschool children.
streptococcus mutans and lactobacill play an important role in the pathogenesis of dental caries. We demonstrated that the number of children with streptococcus mutans or lactobacilli ≥105 cfu/ml was significantly higher in caries affected children compared to caries free children. These findings are supported by previous studies [54-59].
In conclusion, children with caries experience had low levels of α-defensin and salivary pH and greater numbers of streptococcus mutans and lactobacilli. These findings could lead to new tools to screen and assess for caries susceptibility in children.
Acknowledgements
We would like to thank the school authority for their cooperation. Also we thank Dr Gamal Younis for his help and support.
References
- Lenander-Lumikari M, Loimaranta V (2000) Saliva and dental caries. Adv Dent Res. 14: 40–47.
- Stookey G (2008) The effect of saliva on dental caries. J Am Dent Assoc. 139: 11S–17S.
- Van Nieuw Amerongen A, Bolscher J, Veerman E (2004) Salivary proteins: protective and diagnostic value in cariology? Caries Res. 38(3): 247–253.
- Sausan Al, Zubaidah H, David B (2012) Potential uses of human salivary protein and peptide analysis in the diagnosis of disease: a review. Arch Oral Biol. 57(1): 1-9.
- Mandel I, Zorn M, Ruiz R, Thompson RH, Ellison SA (1965) The proteins and protein-bound carbohydrates of parotid saliva in caries-immune and caries-active adults. Arch Oral Biol. 10(3): 471-475.
- Balekjian A, Meyer T, Montague M, Longton R (1976) Electrophoretic patterns of parotid fluid from caries-resistant and caries-susceptible individuals. J Dent Res. 54(4): 850-856.
- Cowman R, Schaefer S, Fitzgerald R, Rosner D, Shklair IL, et al.,(1979) Differential utilization of proteins in saliva from caries-active and caries-free subjects as growth substrates by plaque-forming streptococci. J Dent Res.58(10): 2019-2027.
- Cowman R, Baron S, Fitzgerald R, Danziger JL, Quintana JA, et al.,(1982) Growth inhibition of oral streptococci in saliva by anionic proteins from two caries-free individuals. Infect Immun. 37(2): 513-518.
- Rosan B, Appelbaum B, Golub E, D Malamud, D Mandel (1982) Enhanced saliva-mediated bacterial aggregation and decreased bacterial adhesion in caries-resistant versus caries susceptible individuals. Infect Immun. 38(3):1056-1059.
- Cowman R, Baron S, Fitzgerald R, Stuchell RE, Mandel ID, et al.,(1983) Comparative growth responses of oral streptococci on mixed saliva or the separate submandibular and parotid secretions from caries-active and cariesfree individuals. J Dent Res. 62(9): 946-51.
- Larmas M (1992) Saliva and dental caries: Diagnostic tests for normal dental practice. Int Dent J. 42(4): 199–208.
- Ansai T, Yamashita Y, Shibata Y, Katoh Y, Sakao S, et al., (1994) Relationship between dental caries experience of a group of Japanese kindergarten children and the results of two caries activity tests conducted on their saliva and dental plaque. Int J Paediatr. 4(1): 13–17.
- Fenoll-Palomares C, Munoz-Montagud J, Sanchiz V, Herreros B, Benages A, et al., (2004) Unstimulated salivary flow rate, pH and buffer capacity of saliva in healthy volunteers. Rev Esp Enferm Dig. 96(11): 773–783.
- Michael W, Dorthea A, Connie C, Kathryn M (1997) Parotid saliva protein profiles in caries-free and caries-active adults. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 83(2): 244-251.
- Tulunoglu O, Demirtas S, Tulunoglu I (2006) Total antioxidant levels of saliva in children related to caries, age, and gender. Int J Pediatr Dent. 16(3): 186–191.
- Draper H, Hadley M (1990) Malondialdehyde determination as index of lipid peroxidation. Methods Enzymol. 186: 421– 431.
- Uberos J, Alarcon J, Penalver M, Molina-Carballo A, Ruiz M, et al., (2008) Influence of the antioxidant content of saliva on dental caries in an at-risk community. Br Dent J. 205-214.
- Preethi B, Reshma D, Anand P (2010) Evaluation of flow rate, pH, buffering capacity, calcium, total proteins and total antioxidant capacity levels of saliva in caries free and caries active children: an in vivo study. Indian J Clin Biochem. 25(4): 425–428.
- Mahjoub S, Ghasempour M, Gharage A, Bijani A, Masrourroudsari J, (2014) Comparison of total antioxidant capacity in saliva of children with severe early childhood caries and caries-free children. Caries Res. 48(4): 271–275.
- Muchandi S, Walimbe H, Bijle M, Nankar M, Karekar P, et al.,(2015) Comparative evaluation and correlation of salivary total antioxidant capacity and salivary pH in caries-free and severe early childhood caries children. J Contemp Dent Pract. 16(3): 234–237.
- Hegde A, Rai K, Padmanabhan V (2009) Total antioxidant capacity of saliva and its relation with early childhood caries and rampant caries. J Clin Pediatr Dent. 33(3): 231–234.
- Kumar D, Pandey R, Agrawal D (2011) An estimation and evaluation of total antioxidant capacity of saliva in children with severe early childhood caries. Int J Pediatr Dent. 21(6): 459–464.
- Gardner MS, Rowland MD, Siu AY, Bundy JL, Wangener DK, et al.,(2009) Comprehensive defensin assay for saliva. Anal Chem. 81(2): 557-566.
- Mizukawa N, Sugiyama K, Ueno T, Mishima K, Takaqi S, et al., (1999) Levels of human defensin-1, an antimicrobial peptide, in saliva of patients with oral inflammation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 87(5): 539–543.
- Goebel C, Mackay L, Vickers E, Mather LE (2000) Determination of defensin HNP-1, HNP-2, and HNP-3 in human saliva by using LC/MS. Peptides. 21(6): 757–765.
- Tao R, Jurevic R, Coulton K, Tsutsui MT, Roberts MC, et al., (2005) Salivary antimicrobial peptide expression and dental caries experience in children. Antimicrob Agents Chemother. 49(9): 3883–3888.
- Dale B, Tao R, Kimball R, Jurevic R (2006) Oral antimicrobial peptides and biological control of caries. BMC Oral Health. 6(1): S1-S13.
- World Health Organization (1997) Oral health surveys – basic methods. (4th edn), Geneva: World Health Organization.
- Klein H, Palmer C, Knustson J (1938) Studies on dental caries(I) Dental status and dental needs of elementary school children . Puplic Health Report. 35: 751.
- Grubbel A (1944) Measurements of dental caries prevalence and treatment services for deciduous teeth. J Dent Res. 23(3): 163.
- Jackson D, James P, Slack G (1963) An investigation into the use of indices devised for clinical measurement of caries degree. Arch Oral Biol. 8(2): 55- 64.
- Chiappin S, Antonelli G, Gatti R, De Palo E (2007) Saliva specimen: A new laboratory tool for diagnostic and basic investigation. Invited critical review. Clinica Chimica Acta. 383(1-2): 30–40.
- Mortisuka M, Kitasako Y, Barrow M, Ikeda M, Tagami J, et al., (2006) Quantitative assessment for stimulated saliva flow rate and buffering capacity in relation to different ages. J Dent. 34: 716 – 720.
- SPSS (Statistical Package Social Science) version 14 (2014) SPSS incorporation, Chicago (ILL).
- Fontana M, Zero D (2006) Assessing patients’ caries risk. J Am Dent Assoc. 137(9): 1231–1239.
- Krasse B (1985) Caries risk. A practical guide for assessment and control. Quintessence Pub. Chicago, USA.
- Parvinen T, Larmas M (1981) The relation of stimulated salivary flow rate and pH to lactobacillus and yeast concentrations in saliva. J Dent Res.60(12): 1929–1935.
- Cunha-Cruz J, Scott J, Rothen M, Mancl L, Lawhorn T, et al.,(2013) Salivary characteristics and dental caries: Evidence from general dental practices. J Am Dent Assoc. 144(5): 31–40.
- Diaz de Guillory C, Schoolfield JD, Johnson D, Yeh CK, Chen S, et al., (2014) Co-relationships between glandular salivary flow rates and dental caries.Gerodontology. 31(3): 210-219.
- Papas AS, Joshi A, MacDonald SL, Curro FA, Pretara-Spanedda P, et al., (1993) Caries prevalence in xerostomic individuals. J Can Dent Assoc. 59(2): 171-174, 177-179.
- Loesche W (1986) Role of Streptococcus mutans in human dental decay. Microbiol Rev. 50(4): 353–380.
- Animireddy D, Reddy Bekkem VT, Vallala P, Kotha SB, Ankireddy S, et al., (2014) Evaluation of pH, buffering capacity, viscosity and flow rate levels of saliva in caries-free, minimal caries and nursing caries children: An in vivo study. Contemp Clin Dent. 5(3): 324-328.
- Leone C, Oppenheim F (2001) Physical and chemical aspects of saliva as indicators of risk for dental caries in human. J Dent Educ. 65(10): 1054–1064.
- Krasse B (1990) Microbiological and salivary risk factors. Risk assessment in dentistry. University of North Carolina, Chapel Hill, N.C.
- Tukia-Kulmala H, Tenovuo J (1993) Intra- and inter-individual variation in salivary flow rate, buffer effect, lactobacilli, and mutans streptococci among 11- to 12-year-old schoolchildren. Acta Odont Scand. 51(1): 31–37.
- Vehkalahti M, Nikula-Sarakorpi E, Paunio I (1996) Evaluation of salivary tests and dental status in the prediction of caries increment in caries-susceptible teenagers. Caries Res. 30(1): 22–28.
- Ericsson Y (1959) Clinical investigation of the salivary buffering effect. Acta Odontol Scan. 17(2): 131–165.
- Ericsson Y (1962) Recent Advances in Dental Caries Research: Biochemistry. Salivary Food Factors in Dental Caries Development. Int Dent J 12:476–495.
- Hegde AM, Rai K, Padmanabhan V (2009) Total antioxidant capacity of saliva and its relation with early childhood caries and rampant caries. J Clin Pediatr Dent. 33(3): 231–234.
- Roa NS, Chaves M, Gomez M, Jaramillo A (2008) Association of salivary proteins with dental caries in a Colombian population. Acta Odontol Latinoma, 21(1): 69-75.
- Dodwad R, Betigeri A, Preeti B (2011) Estimation of total antioxidant capacity levels in saliva of caries-free and caries-active children. Contemp Clin Dent. 2(1): 17–20.
- Ribeiro T, Dria K, de Carvalho C, Monterio AJ, Fonteles MC, et al.,(2013) Salivary peptide profile and its association with early childhood caries. Int J Pediatr Dent. 23(3): 225-234.
- Toomarian L , Sattari M, Hashemi N, Tadayon N, Akbarzadeh BA, (2011) Comparison of neutrophil apoptosis, α-defensins and calprotectin in children with and without severe early childhood caries. Iran J Immunol. 8(1): 11-19.
- Kohler B, Bjarnason S (1992) Mutans streptococci, lactobacilli and caries prevalence in 15 to 16-year olds in Goteborg. Part II. Swed Dent J. 16(6): 253–259.
- Becker M, Paster B, Leys EJ, Kenyon SG, Galvin JL, et al., (2002) Molecular analysis of bacterial species associated with childhood caries. J Clin Microbiol. 40(3): 1001–1009.
- Marsh P (2003) Are dental diseases examples of ecological catastrophes? Microbiology. 149(2): 279–294.
- Corby P, Lyons-Weiler J, Bretz WA, Hart TC, Aas JA, et al., (2005) Microbial risk indicators of early childhood caries. J Clin Microbiol. 43(11): 5753–5759.
- Aas J, Griffen AL, Sara RD, Alice ML, Floyd E, et al.,(2008) Bacteria of dental caries in primary and permanent teeth in children and young adults. J Clin Microbiol. 46(4): 1407–1417.
- Parisotto T, Steiner-Oliveira C, Silva CM, Rodriques LK, Nobre-dos-Santos M, et al., (2010) Early childhood caries and mutans streptococci: a systematic review. Oral Health Prev Dent. 8(1): 59–70.





