Patterns of the Oro-facial Neural Manifestations in Patients with Multiple Sclerosis Admitted into Hospitals in Kerman (Iran)
Mahdian M1, Navabi N2*, Roozbakhshian MR3, Seddighi B4
1 General Dentist, Private Practice.
2 Assistant Professor, Oral and Dental Diseases Research Center, Kerman University of Medical Sciences, Kerman, Iran.
3 Specialist in Oral Medicine, Private Practice.
4 Associated Professor, Department of Neurology, Kerman University of Medical Sciences, Kerman, Iran.
*Corresponding Author
Nader Navabi DDS, MD,
Assistant professor,
Kerman school of dentistry,
Shafa Ave, Jomhoori-Islami BLVD, Kerman, Iran.
Tel: 7618759689
Fax: 0098 341 2118073
E-mail: n_navabi@kmu.ac.ir
Article Type: Research Article
Received: April 13, 2015; Accepted: May 23, 2015; Published: May 26, 2015
Citation: Mahsa Mahdian, Navabi N, Mohammad Reza Z, Sedighi B (2015) Patterns of the Oro-facial Neural Manifestations in Patients with Multiple Sclerosis Admitted into Hospitals in Kerman (Iran). Int J Dentistry Oral Sci. 2(5), 75-78. doi: dx.doi.org/10.19070/2377-8075-1500016
Copyright: Navabi N© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aims: Studies have shown an increase in the incidence of multiple sclerosis (MS) in recent years. This medical condition exhibits motor-sensory manifestations in the oral cavity and face. The aim of the present study was to evaluate the prevalence of these manifestations in patients with MS in Kerman Province, Iran, in 2013.
Methods: A total of 100 patients with MS, based on McDonald’s 2010 Diagnostic Criteria, were selected by simple sampling technique for the purpose of the present cross-sectional study. All the subjects received treatment in the Department of Neurology in Kerman Shafa Hospital.
Results: Eighty patients were female and the mean age of the subjects was 36.4 years; 33% and 43% of the subjects had dysphagia and a feeling of an unpleasant taste in the oral cavity or a history of facial pains, respectively.
Conclusion: Based on the results of the present study, it is recommended that dentists take account of the oral problems of patients with MS due to the sensory problems of these patients.
2.Introduction
3.Materials and Methods
3.1.Evaluation of a change in the sense of taste
3.2.Evaluation of dysphagia
3.3.Evaluation of trigeminal neuralgia
4.Results
5.Discussion
6.Conclusion
7.Acknowledgment
8.References
Keywords
Multiple Sclerosis; Oral; Facial.
Introduction
Multiple sclerosis (MS) is the most prevalent inflammatory disease, in which demyelination, i.e. destruction of the lipid or myelinsheath of nerves, takes place [1-3]. The condition appears as multiple plaques in the white matter of the brain and the spiral cord and is very progressive and debilitating [4-6]. There are conflicting reports about the gender of patients, with a higher rate of affliction in females compared to males [7]. The etiology of MS is unknown and different studies have highlighted the role of one environmental or acquired factor as the causative agent; however, it appears autoimmune factors are the most probable etiologic agents [8, 9]. Although MS is not a hereditary condition, a family history of MS can make an individual susceptible to it [9]. The clinical symptoms and signs of MS might consist of loss of muscular control and coordination from mild to severe forms [2]. In the most common course of the condition the patient first experiences a series of symptoms and signs that regress and disappear. These symptoms and signs disappear partially or completely and after a period of remission, progressive destruction of nerve sheaths begins [3, 8]. There is no definitive treatment for MS at present and the treatments available only result in decreasing the symptoms or signs. Some techniques used to treat MS include changing and modifying behavior patterns, medications, physical activity, rehabilitation, auxiliary devices and some other techniques [10-13]. In some patients with progressive symptoms and signs, chemotherapy and steroids might be effective [3].
Three principal Oro-facial Neural Manifestations of MS include the followings:
- Trigeminal neuralgia due to the demyelination of the trigeminal nerve, which is usually manifested after the diagnosis of MS. The patients complain of acute and lancinating facial pain. These pain episodes are repeated during the day and if the patient is young and the pain appears bilaterally, it is in favor of a diagnosis of MS [13-16]. MS is diagnosed with the help of trigeminal neuralgia in 2-4% of the patients. Routine daily activities, including speaking and eating, might result in pain, severely affecting the patient’s quality of life [13, 14]. In addition, if neuralgia is not diagnosed correctly by the dentist, attempts might be made at unnecessary tooth extraction [16].
- Sensory neuropathy: Neuropathy might affect the second and third branches of the trigeminal nerve; it has a progressive, bilateral and irreversible nature. The condition has a rapid onset and is sometimes associated with pain. The neuropathy of the mental branch leads to the anesthesia of the lower lip and chin area, with or without pain. Several studies have shown that the neuropathic pain in patients with MS is manifested in 26-58% of cases, indicating that pain is common in such patients [17].
- Paralysis of the motornerves:Paralysis of the facial nerve is in fact the loss of all the voluntary movements of facial muscles on one side and usually occurs in the final stages of the disease [12, 14]. Almost 24% of MS patients suffer from the paralysis of the facial nerve. Generally, patients with functional disturbances in the neurologic pathways controlling deglutition are the first candidates for dysphagia which is seen in more than one-third of patients with MS. Functional disturbances in the muscles of the oral cavity, pharynx and esophagus result in complications such as the problem of food remaining in the oral cavity, inability to swallow properly, packing of food into the pharynx, food remaining in the pharynx and aspiration of food into the larynx [15-18].
Materials and Methods
In the present cross-sectional study, simple random sampling technique was used to select 100 patients with MS, who had referred to the Department of Neurology of Shafa Hospital, Kerman, Iran, and the private office of a neurologist in Kerman and had undergone consecutive examinations in 2013. All the subjects had files in the Iranian Association of MS patients. All the diagnoses by the neurologist were based on the Revised McDonald’s Criteria (2010) for MS and use of the MRI technique. In addition, the demographic variables of the subjects were evaluated, which included age, gender, education, living district/area and the duration of affliction with MS. The questionnaires were filled out and clinical examinations were carried out by a third-year postgraduate student of oral medicine. Examinations were carried out on a dental unit and use of disposable dental mirrors, latex gloves, dental explorers and periodontal probes. In case of hospitalized subjects, examinations were carried out with the use of an electric hand torch [15, 16, 19, 20].
Any disturbance in the sense of taste or feeling of any abnormal taste in the oral cavity is referred to as parageusia or dysgeusia, which was evaluated in the present study based on the following criteria. A change in the sense of taste was identified when the patient gave a positive response to at least to 3 of the 5 following questions:
- Do you have any unpleasant taste in your mouth?
- Do you have any problems with one or several tastes?
- Have there been any changes in your diet?
- Have the disturbances resulted in any changes in your daily activities?
- Can you feel the following tastes: the bitterness of coffee, the sweetness of an ice cream, the saltiness of French fries and the sourness of lemons?
To evaluate dysphagia, the history of the problem, coughing during deglutition, history of skipping a meal or resorting to soft feeds were questioned [18].
To evaluate affliction with trigeminal neuralgia, the subjects were questioned about a history of facial pains, the time and location of these pains and the factors initiating such pains [8].
Data were recorded in questionnaires and analyzed with SPSS 18. Descriptive statics, including central parameters, distribution parameters and frequencies and percentages were used for descriptive purposes. The patients received explanations about the reasons for examinations and questionings and informed consent was obtained. All the examinations were carried out and data recorded anonymously. The necessary counseling for treatment modalities and options in the faculty were provided for all the subjects.
Results
Of 100 subjects, 80 and 20 subjects were female and male, respectively, with a mean age of 36.4 and standard deviation of 7.49 (an age range of 21-57). The mean age of affliction with the disease was 28.8 years with a standard deviation of 6.61 years (with a range of 17-45 years). The majority of the subjects were married (82%). Of 20 male subjects, 17 were self-employed and employees. Of 80 female subjects, 68 were housewives (67.5%). The mean time since the last labor in female patients was 10.87% years, with the shortest and longest time since labor being 2 and 21 years, respectively. Of 61 married subjects in the present study, 21% had a history of two deliveries, which was the highest frequency, followed by 17% of women having 3 deliveries. None of the female subjects were in the lactating period.
A total of 95% of the subjects had a history of dental visits, with 25% referring for tooth restoration and 1% for surgical procedures, comprising the most and the least frequencies for dental visits, respectively. The most frequent treatments were tooth restorations, root canal therapies and tooth extractions (21%) and the least frequent treatment was scaling and root planing (2%). The mean time of the last dental visit was 22.66 months. The shortest and longest times since the last dentalvisit were 1 month and 13 years, respectively. A total of 22% of the subjects had other medical conditions, too, apart from MS, including hypothy roidism and hypertension as the most frequent entities. In relation to the use of specific medications the following medications were used by the subjects: Cinovex (32%), Interferon (10%), Zinferon (9%), Rebifor (8%), GA (Topamer) (6%) and Recigen (5%).
Table-1 presents the frequencies and frequency percentages of patients with dysphagia and taste disorders, based on clinical examinations.Table 2 presents the frequencies of facial pains as reported by the subjects.
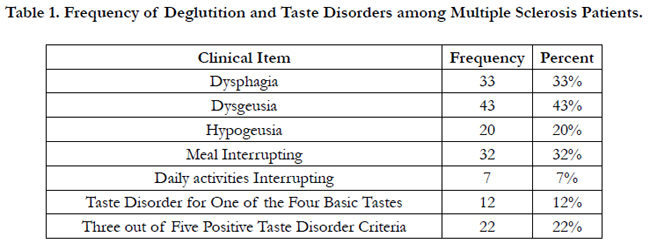

Table 1. Frequency of Deglutition and Taste Disorders among Multiple Sclerosis Patients.
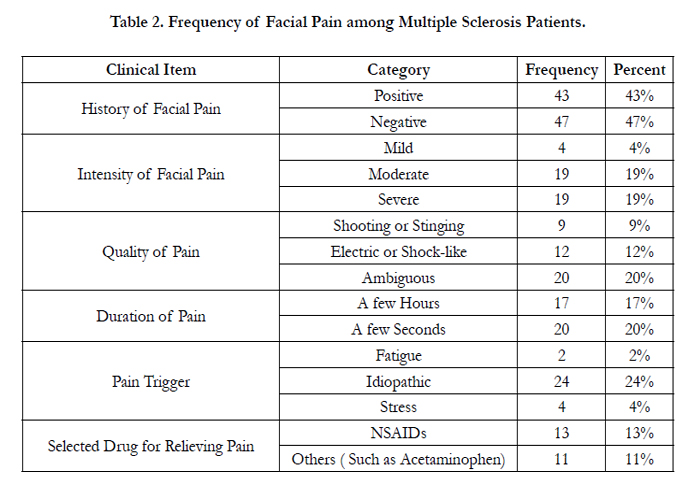
Table 2. Frequency of Facial Pain among Multiple Sclerosis Patients.
Discussion
The present study was carried outto determine the frequency of oral and facial neurologic manifestations in patients with Multiple sclerosis (MS) in Kerman Province in 2013. MS is very debilitating chronic disease, with social and economic complications. The disease causes serious problems for patients, resulting in the loss of personal independence and resulting in limitations in the social activities of the patient.
The present study showed a prevalence rate of 80% in females of 100 patients under study with a female-to-male ratio of 4:1. Different ratios have been reported in previous studies but in general the disease has been reported to be more common in females compared to males. In a study by Canellas, the disease was twice more common in females compared to males, with an affliction age range of 20-40 [7]. In the study by Nedjon and Montazeri the female-to-male ratio was reported to be 10:3 [8], with 3:1 in a study by Inalou et al in southern Iran [22]. In a study by Fatemi andShoaibi in Khorasan Province in Iran the prevalence of MS in females was three times that in males [23]. In a study in Turkey, the symptoms and signs had appeared under 16 years of age in 41.3% of the patients.
A study by Lasemi et al showed that the most prevalent manifestations in these patients were visual symptoms and signs, with trigeminal neuralgia being the least common manifestation [6]. In other words, of every 5 patients with MS, 4 had visual problems and those who had oral manifestations were afflicted with the disease for more than 7 years in 40.9% of the cases and only 14.7% of patients with more than 7 years of affliction did not have orodental manifestations. In addition, dysphagia, speech problems, trigeminal nerve neuralgia, facial paralysis and visual problems had appeared in 90%, 88%, 70%, 62% and 39% of the patients after the initial diagnosis of the condition. Facial paralysis and trigeminal nerve neuralgia were found in almost 25% of MS patients before the diagnosis was established. In another study by Pourjavad et al in Isfahan in 2009, the prevalence of dysphagia was 3.7% in MS patients [19]. Osterberg et al., (2005) reported a prevalence rate of 4.9% for trigeminal neuralgia in MS patients in Sweden [24].
In relation to the use of specific medications in the present study, the subjects took the following medication: Cinovex (32%), Interferon (10%), Zinferon (9%), Rebifor (8%), GA (Topamer) (6%) and Recigen (5%). A study in Turkey showed that 68 patients (51.1%) took immunosuppressive agents, including Azathioprine, Glatiramer acetate and Interferon-β [25]. In the present study, 44% of the subjects had dysphagia; in previous studies, dysphagia was observed in more than a third of the patients with MS. Calgano et al reported dysphagia in 34.3% of patients with MS [15]. In a study by Lasemi et al, dysphagia was reported in 21% of patients with MS [19]. In addition, 33% of patients suffered from xerostomia, consistent with the results of previous studies [13].
In the present study a large number of MS patients were unable to cooperate during examinations due to severe inability to more. Since neuropathy and pain of the facial area are a major component of the problems these patients have and oral medicine departments at present can evaluate these aspects of the problems in such patients, further studies are suggested in this respect. It appears it is necessary o establish a special ward for the examination and treatment of systemic patients, including MS patients, so that it would be possible to carry out epidemiological studies and train students and assistants interested in this dental field. It appears it is rational to prepare a comprehensive program for the examination and treatment of the patients at a time when the symptoms and signs have not become severe, so that lower costs would be inflicted on the health system in the long term and the quality of life of these patients would improve.
Conclusion
Not only will the quality of life of such patients improve by evaluation of the oro-facial problems of such patients and by finding ways to prevent and treat such problems in early stages, but also the treatment costs of such patients will significantly decrease. Furthermore, MS patients in advanced stages of the disease require some modifications in their dental treatment planning because they have problem in relation to observing oral hygiene due to the involvement of motor nerves. Dentists should be familiar with the clinical manifestations of MS in the oral and maxillofacial region and the problems related to the general health of such patients.
Acknowledgment
This study was financially supported by Oral and Dental Diseases Research center, Kerman University of Medical Sciences (Research No: 92/510) and This paper has been written from professional thesis number 77 of Kerman dental school.
References
- Chemaly D, Lefrancois A, Perussê R (2000) Oral and maxillofacial manifestations of multiple sclerosis. J. Can. Dent. Assoc 66(11): 600-605.
- Danesh-Sani SA, Rahimdoost A, Soltani M, Ghiyasi M, Haghdoost N, et al. (2013) Clinical assessment of orofacial manifestations in 500 patients with multiple sclerosis. J Oral Maxillofac Surg 71(2): 290-294.
- Devor M, Govrin-Lippmann R, Rappaport Z.H (2002) Mechanism of trigeminal neuralgia: An ultrastructural analysis of trigeminal root specimens obtained during microvascular decompression surgery. J. Neurosurg 96(3):532-543.
- Bruck W, Stadelmann C (2003) Inflammation and degeneration in multiple sclerosis. Neurol. Sci 24: S265-267.
- D. Fragoso, H.H. Alves, L.C. Alves, N.C. Alves, C.M. Andrade, et al. (2010) Dental care in multiple sclerosis: an overlooked and under-assessed condition. Journal of Disability and Oral Health; 112 53-56
- Lasemi E, Sahraian M, Kalantar Motamedi M, Valayi N, Moradi N, et al. (2011) prevalence of oral and maxillofacial manifestations in patients with multiple sclerosis.. J Res Dent Sci 8(1) :20-26.
- Frohman EM (2003) Multiple sclerosis; Med. Clin. North Am 87: 867-897.7
- Fukazawa T, Monwaka F, Humada K, Hamad T, Tashiro K (1997) Facial palsy in multiple sclerosis.J neural 244(10): 631-633.
- Goodin DS, Frohman EM, Garmany GP Jr, Halper J, Likosky WH, et al. (2002) Disease modifying therapies in multiple sclerosis: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and the MS Council for Clinical Practice Guidelines. Neurology 58(2): 169-178.
- McDonald WI, Compston A, Edan G , Goodkin D, Hartung HP, et al. (2001) Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the diagnosis of multiple sclerosis. Ann. Neurol 50(1): 121–127.
- McCormack PL, Scott LJ (2004) Interferon-beta-lb: a review of its use in relapsing-remitting and secondary progressive multiple sclerosis. CNS Drugs 18(8): 521-546.
- Kovac Z, Uhac I, Buković D, Cabov T, Kovacević D, et al. (2005) Oral health status and temporomandibular disorders in multiple sclerosis patients. CollAntropol De 29(2): 441-444.
- Matsuka Y, Fort ET, Merrill RL (2000) Trigeminal neuralgia due to an acoustic neuroma in the cerebellopontine angle. J. Orofac. Pain 14(2): 147-151.
- Gulay A, Rock H, Li W (2009) Multiple sclerosis and acute disseminated encephalomyelitis diagnosed in children after long-term follow-up: comparison of presenting features. Dev Med Child Neurol 51(6): 480–486.
- Derya K, Egemen I, Serkan O (2012) Inflammatory Demyelinating Central Nervous System Diseases in Childhood: Clinical and Paraclinical Profiles in 133 Patients. Hindawi Publishing Corporation Autoimmune Diseases 63(9): 102-108.
- Mury CG, Merson J, Daly Ti (1980) Radiation necrosis of the mandible: A 10 years study. Int J radiat Oncd Biol Phy 6: 593-6.
- O’Connor P (2002) Canadian Multiple Sclerosis Working Group. Key issues in the diagnosis and treatment of multiple sclerosis: An overview. Neurology 59(6): 1-33.
- Pauova DE, Dejaeyerb E, Dheoghe Bc, Cartond H (2002) Dysphagia in multiple sclerosis. clin neurosurg 104: 345-351.
- Russel SL, Reisin S (1998) Investigation of xerostomia in patients with Rheumatoid Arthritis. JADA 129: 733-739.
- Kovac Z, Uhac I, Buković D, Cabov T, Kovacević D, et al. (2005) Oral Health Status and Temporomandibular Disorders in Multiple Sclerosis Patients. Coll. Antropol 29(2): 441–444.
- Yamashita H, Nakaquwa K, Togo M (2006) Taste dysfunction in Patient receiving radio therapy. Head Neck 28(6): 508-516.
- Inaloo S, Yavari MJ, Saboori S (2008) Multiple Sclerosis in Children: A review of clinical and practical features in 26 cases. IJCM 2(4): 41-46.
- Jarin V, Anannit V, Lochana T, Prapasri S, Chaiyos Kh, et al. (2010) Acute disseminated encephalomyelitis: A 10-year cohort study in Thai children. Eur. J. Paediatr. Neurol 14(6): 513–518.
- Osterberg A, Boivie J, Thuomas KA (2005) Central pain in multiple sclerosis-prevalence & clinical characteristics. Eur J Pain 9(5): 531-542.
- Hiroyuki T, Ryutaro K, Yoshito I, Masafumi S, Yui Y, et al. (2010) Clinical study of childhood acute disseminated encephalomyelitis, multiple sclerosis, and acute transverse myelitis in Fukuoka Prefecture, Japan. Brain Dev 32(7):454–462.





