Knowledge of Risks Associated with Dental Implants Failure
Al-Dwairi ZN1*, Abu-Al Haija MA2
1 Professor of Prosthodontics, Department of Prosthodontics, Jordan University of Science and Technology, Jordan.
2 Private practice, Amman-Jordan.
*Corresponding Author
Ziad N. Al-Dwairi BDS, PhD, FIADFE,
Professor of Prosthodontics,
Department of Prosthodontics, Jordan
University of Science and Technology,
Po Box 3030, Irbid 22110
Jordan.
Fax: 0096227201080
E-mail: ziadd@just.edu.jo
Article Type: Research Article
Received: February 20, 2015; Accepted: April 17, 2015; Published: April 20, 2015
Citation: Al-Dwairi ZN, Abu-Al Haija MA (2015) Knowledge of Risks Associated with Dental Implants Failure. Int J Dentistry Oral Sci. 2(4) 59-64. doi: dx.doi.org/10.19070/2377-8075-1500013
Copyright: Al-Dwairi ZN© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: This paper presents the results of a survey of dentists practicing implant dentistry regarding their knowledge of risk factors that they considered to be important for predicting dental implant failure.
Materials and Methods: A pilot-tested questionnaire was distributed to 100 dentists known to practice implant dentistry. The questionnaire enquired about speciality, qualifications, dental implant experience in addition to knowledge of factors that could lead to dental implants failure.
Results: Seventy seven participating dentists were working in private sector and 58 were general dental practitioners. Forty eight dentists were reported to place more than 50 implants (per year), and 50% had an experience of less than 5 years. The most widely used implant system in Jordan was the Oraltronics (Pit-Easy®) with 54% having used it. Fifty percent of dentists believed that the posterior maxilla was the most risky intra-oral site for implant failure. Over 50% of the sample believed that cylindrical and machined surface implants were the most risky types of implants associated with failures. Seventy four dentists believed that posterior extension cantilever design was the prosthetic design most associated with dental implant failure. Experience, age and specialty significantly influenced the knowledge of factors that could lead to implant failure (p<0.05). Conclusions: The results obtained underscore the importance of obtaining comprehensive implantology education in Jordan.
2.Introduction
3.Materials and Methods
4.Statistical Analysis
5.Results
6.Discussion
7.Conclusion
8.Acknowledgment
9.References
Keywords
Implant; Risk; Failure; Jordan; Experience.
Introduction
Implant-based dental treatment to restore oral health and function is a widely used treatment option in contemporary dental practice. Since their introduction in 1950, many systems and designs were used, and different success rates have been reported [1]. Basic guidelines of successful implant treatment include: good patient selection criteria, good implant system surface selection, implant system design and configuration, neat surgical procedures, nondisturbed healing phase and excellent prosthetic reconstructions [2-6]. Applying these guidelines should allow good osseo integration, stability and survival of the implants and increase the success rate of this treatment modality [7, 8].
Osseo integration was a hallmark of success of implant dentistry. It was believed that an implant was successfully integrated when there was direct contact between bone and the titanium implant, at the light microscopic level, with no fibrous connective tissue interface. Recently, criteria for implant success have changed. Other factors have been introduced including: stability of the implant; adequate radiographic bone levels, lack of symptoms or evidence of infection, minimal probing depths around the implant and the ability of the patient to keep the area clean [9].
Restorative dentists have a variety of treatment plans to replace teeth. Implants can optimally restore aesthetics and function. Although the overall success rate is very high, dental implants may occasionally fail [10].
The causes and mechanisms of implant failure are unclear. However, different studies have found a variety of statistically significant factors associated with implant failure, these are: age and sex [10], smoking [11], systemic diseases [12, 13], maxillary implant location, quantity and quality of bone [14] and implant surface treatments and characteristics [14, 15]. Immunological [16] and genetic factors [17] have also been reported to be associated with early implant failure.
An unmotivated patient would not be a good candidate for dental implants. Similarly periodontal health may influence implant success. Periodontitis was associated with an increased failure rate of dental implants after approximately 2.5 years with an increased level of bone resorption [18].
Cigarette smoking was associated with an increased rate of implant failures. It not only decreases the vascularity of local tissues but also plays a role in interrupting healing, chemotaxis and the overall systemic immunity. Overall failure rates have been reported as 11% for smokers compared to 5% for non-smokers [11].
It has been reported that types I, II, and III bone offer good strength and primary stability, in contrast to type IV bone which has a thin cortex, low trabecular density, and poor medullary strength. Only 3% of fixtures placed in types I, II, and III bone were lost compared to a 35% failure rate of implants placed in type IV bone [19]. However, bone quality may be less of a concern when cylindrical type implant fixtures are utilized which demonstrated a success rate of 97.5% over 5 years [20].
Systemic health of the patient is also important when considering placement of implants. The repercussions of diabetes on the healing of soft tissue will depend on the degree of glycaemic control and the existence of chronic vascular complications [21]. A review by Mellado-Valero et al [22] found more failures in diabetic patients compared to the general population, the majority during the first year of functional loading. In irradiated bone, the reduced vascularity and also accompanying chemotherapy can affect bone healing of implant sites leading to failure [23].
Poor surgical technique is another possible cause of implant failure, which may result for example from inadequate irrigation of the surgical site or from using low torque and excessive drill speed during placement. Failure can result from excessive temperature elevation in bone during placement, leading to necrosis of the supporting bone around the implant [24].
It has been found that dense, hypovascular, traumatized and previouslycomminuted bone was highly susceptible to heat generationduring drilling and tapping procedures. This may influence implant osseointegration [25].
In Jordan, different implant systems exist and dentists practice implant dentistry as part of their qualifications or based on continuous dental education workshops. No studies have assessed the provision of dental implants or dental implants experience in Jordan. This study aimed to document the state of knowledge of the Jordanian dental implant community about risk factors that they considered to be important for predicting implant failure in an attempt to elicit the extent of the awareness of risks that could potentially impact upon implant failures.
Materials and Methods
This study included 100 randomly chosen Jordanian dentists practising implant dentistry in Jordan each of whom had placed more than one implant. Name lists were obtained from the Jordanian Dental Association records and Jordan Society of Implant Dentistry. Data collection adopted a personal contact structured interview to fill a pilot-tested questionnaire (Appendix 1). Pilot testing was carried out on 20 dentists who were later excluded from the study.
The questionnaire was set after a thorough review of literature taking into account the possible risk factors for implant failure which were grouped into:
- Patient- related factors: age, gender, medical history, intra oral sites, oral hygiene and smoking.
- Implant- related factors: the design of implant surfaces (machined surfaces, sand blasted, sand blasted and acid etched, titanium plasma spray, HA coated, resorbable bioactive materials coat, dual acid etched) and fixture shape.
- Surgical factors: traumatic procedures and immediate implantation.
- Prosthetic factors: type of supported prosthesis (fixed partial denture, fixed detachable prosthesis, removable detachable prosthesis, resilient overdenture and cantilever designs of fixed prosthesis), and the loading protocol of the prosthesis (immediate, early, and delayed).
Statistical Analysis
Data analysis was carried out using the statistical package for social sciences software (SPSS), version 11.0. Variables were described using frequency tables. Associations among variables such as level of dental implant experience, specialty status and types of risk factors were assessed using the Chi-squared statistics with a threshold of significance set at a P-value of 0.05.
Results
All one hundred dentists were included in this study. Table 1 shows the distribution of the sample population by gender according to age, experience and specialty. Ages of participants ranged from 25 to 60 years and 75% were between the ages of 31 - 50 years. Fifty dentists had practical experience as implant practitioners for less than 5 years. Practitioners with more experience were in the age group of 41 to 50 years of age (P < 0.01).
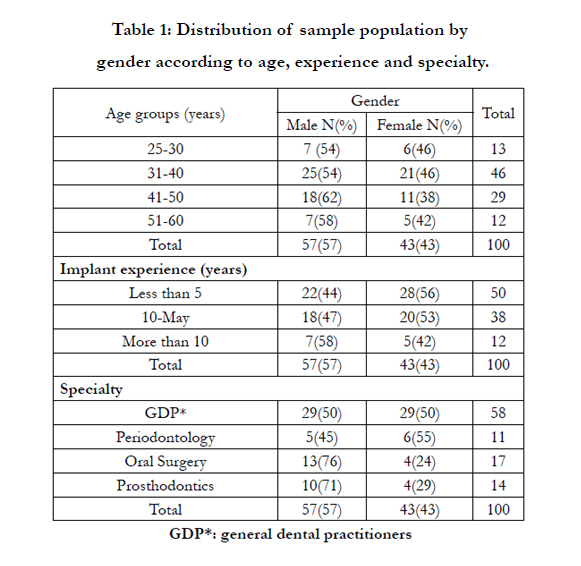

Table 1: Distribution of sample population by gender according to age, experience and specialty.
Regarding speciality, 58% percent of the sample was general dental practitioners (GDP’s), 11% Periodontists, 17% Oral Surgeons and 14% were Prosthodontists. Seventy-seven percent of dentists were private practitioners, 8% were working in the Ministry of Health and 15% in Universities. All the practitioners in Universities and the Ministry of Health were specialists, whilst only around 25% (19/77) of the private practitioners were specialists. Forty eight dentists had placed more than 50 fixtures, most of whom were private practitioners (p<0.05), Table 2.
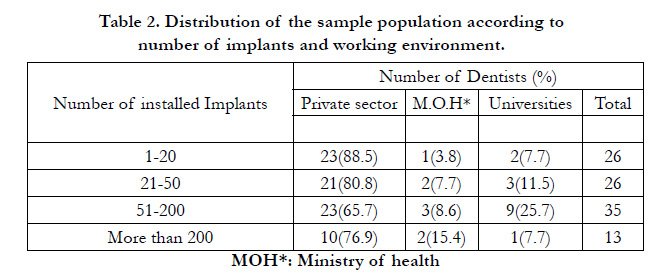
Table 2. Distribution of the sample population according to number of implants and working environment
Figure 1 shows the list of the different implant systems used in Jordan. Among different implant systems available, the Oraltronics (Pit-Easy®) system from Germany was found to be used by 54% of dentists.
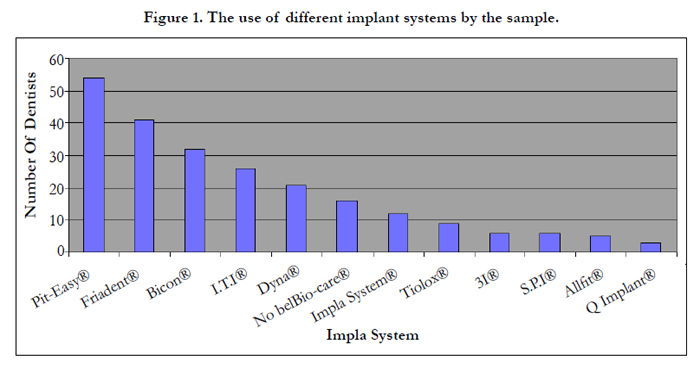
Figure 1. The use of different implant systems by the sample
Thirty two dentists suggested that a patient age of 61 years and above was the most susceptible age for implant failure, whilst 24 dentists lacked knowledge on the contribution of age. Sixty one dentists considered gender as an irrelevant factor in implant failure.
As for intra-oral location, significantly more practitioners considered the posterior maxilla as the most susceptible location for failure in comparison to other intraoral sites. (P < 0.05). Uncontrolled diabetes mellitus, osteoporosis and radiotherapy were considered by 63%, 36%, and 20% respectively as being the most common medical conditions involved in dental implant failure. Over 95% considered poor oral hygiene as a potential risk factor for implant failure. Smoking had unanimous agreement (100%) to be a major risk factor.
Cylindrical fixtures were considered by 56% as the design most likely to be associated with failure, whilst 60% of dentists considered machined surface implants to have been the most common reason for failure.
Among the surgical procedures, traumatic surgery was significantly reported by 65% as a major risk factor for implant failure, while immediate implantation was considered by 37 dentists as a potential risk factor. Immediate loading was considered by 46% of practitioners as an important factor leading to failure, whilst 25% believed that early loading was a risk factor. As for the type of prosthesis, posterior extension cantilever designs were considered as a risk factor for implant failure by 74% of participants. Table 3 summarizes the risk factors as most likely to lead to dental implant failure that were considered by a significant number of practitioners according to their age, experience and speciality.
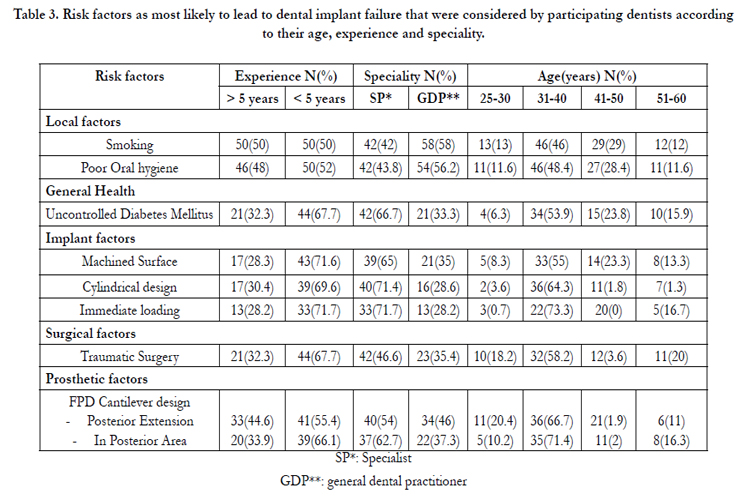
Table 3. Risk factors as most likely to lead to dental implant failure that were considered by participating dentists according to their age, experience and speciality.
Discussion
Current dental implant technologies and materials continue to develop at a strong pace. Implantology is often the procedure of choice when patients are faced with the decision to replace single or multiple teeth.
The selected sample was of implant practitioners in private and public (Universities and Ministry of Health) sectors. The number of private practitioners was significantly higher than those who practiced in a public work environment. This may be due to the fact that there are only two dental schools in Jordan with limited number of specialists with implant experience. Similarly in the Ministry of Health, specialists are limited to those who obtained their postgraduate training in implant dentistry from the aforementioned dental schools. Most of the questions in this survey required detailed knowledge of dentists to decide what factors contribute more to failure of dental implants. Many of these dentists lacked implantology expertise. This is reflected by that fact that 50% of the sample had experience of less than 5 years in the field of implant dentistry and only 48 % of the sample had placed more than 50 fixtures.
In most studies [12, 14, 15] age and sex were not related to early implant failure. Noguerol et al [26] had more failures in patients aged 41-60 years than in patients aged over 60 implying that older age was not contraindicative to implant treatment.
On the other hand, Sverzut et al [11] observed that the possibility for early failure of implants was increased by a factor of 1.075 for each additional year in patient age. In addition, advanced age increased the risk of implant failure; patients older than 60 years were twice as likely to have adverse outcomes. One explanation for this phenomenon may be the loss of bone mineral associated with increasing age [27]. Regarding gender, Sverzut et al[11] found that men had a 1.255 times greater risk of early implant failure than women. In the present survey older age was considered as a contributing risk factor for implant failure while gender was reported to be irrelevant.
The results showed a great spread of new implant systems over other systems in Jordan. The most frequently used system was the OralTronics® company “Pit-Easy®” where records of simplicity, diversity of diameters, lengths, designs and surfaces of the fixtures were remarked as features in this system that might contributed to its wide use. The ITI® System was used less (26%) and was reputed to be of high cost, a factor that lessened its use,despite its well known good reputation worldwide.
As for implant location, three times more failures have been observed in the maxilla than the mandible [28]. In a study by van Steenberghe et al [14] approximately half the early failures occurred in the posterior maxilla. When comparing success rates, the posterior maxillary region had a success rate of 91.4% compared to the anterior maxillary region with 97%, 96.3% in the posterior mandible and 97.9% in the anterior mandible. Alsaadi et al [12] found significantly more failures in the posterior region of both jaws compared to the anterior mandibular region. However, in a prospective study by Alsaadi et al [13] the implant site was not a significant factor in implant failure. In agreement with a previous study [10], 50% of dentists agreed that the posterior maxilla was the most susceptible location for failure, while the anterior mandible was the least (7%). This was attributed to the superiority of bone quality in the anterior mandible compared to the bone in the posterior maxilla. The latter was considered the least favourable for primary stability of dental implants. The results suggested this agreement with the literature data, but it should be remembered that, although some intra-oral sites comprise risks to dental implants, this doesn't exclude them as favourable implant sites when a proper treatment protocol is carried out.
In a study by van Steenberghe et al [14] chemotherapy and radiotherapy of oral tissues were significantly related to implant failure; and patients with claustrophobia had more failures as surgery was carried out under insufficiently sterile conditions. Uncontrolled diabetes may also adversely affect bone healing and immunological response. Osteoporosis may lower both quality and quantity of alveolar bone, although alveolar bone is the last bone to be affected. Radiotherapy may lower bone vascularisation that would affect healing in recipient sites rendering these sites susceptible to osteo-radionecrosis [19-23]. Smoking is a common contributor to decreased tissue oxygenation [11]. Carbon monoxide, oxidant radicals, nitrosamines, and nicotine are released during smoking. Nicotine causes a systemic increase in epinephrine, norepinephrine and carboxyhemoglobin, and also decreases blood flow, collagen deposition, prostacyclin formation. Nicotine also increases platelet aggregation, causes polymorphonuclear neutrophil dysfunction, and increases fibrinogen and blood viscosity, all of which negatively affect wound healing. It has been concluded that long-term smoking results in poor bone quality and a poorer prognosis for implants [11].
Several studies [13, 15, 26] found significantly more failures in heavy smokers (> 20 cigarettes / day) than in non-smokers and early failure of implants was related to smoking and increased with cigarette consumption [13]. Van Steenberghe et al [14] found that approximately one in every three implant failures occurred in smokers, and one in five patients with early failures smoked more than 10 cigarettes per day, whilst only 12.3% of patients without failures were smokers. Konstrom et al [16] found an association with smoking although it was not the most important factor. In contrast, Sverzut et al [11] did not observe any statistically significant association between smoking and early implant failures, concluding that smoking alone cannot be considered a risk factor for early failure of implants. In the present study, smoking had unanimous agreement to consider it the major risk factor. This concurs with many previous studies [1, 18].
There are a number of surface treatments commercially available on dental implants. Most of these surfaces have proven clinical efficacy (>95% over 5 years). However, the development of these surfaces has been empirical, requiring numerous in vitro and in vivo tests. Most of these tests were not standardized, using different surfaces, cell populations or animal models. The exact role of surface chemistry and topography on the early events of the osseointegration of dental implants remain poorly understood [29]. Machined surfaces and hydroxyapatite (HA) coated implants were considered by most participating dentists as the worst surface treatments and the most susceptible for failure. The lowest percentage (6%) was for titanium plasma sprayed surfaces. The literature revealed an approximation to these results [2, 3], with some researchers defending the HA coated surfaces as well as the machined surfaces. Several studies [2-5] revealed the impossibility of direct osseo-genesis on smooth implant surfaces, as well as microcracks and disruption of the HA coating on HA coated implants.
Hollow-cylinders, solid cylinders, hollow screws or solid screws are commonly employed shapes which are designed to maximise the potential area for osseointegration and provide good initial stability. Even minor alterations in the size and pitch of threads can enhance the latter property. Screw shaped implants also offer good load distribution characteristics in function [29].
Cylindrical and stepped fixture designs were reported to be associated with the highest percentage of failure. The least percentage was for the root shape design 10.1%. This is not in agreement with other results [6, 7]. This can be due to lack of scientific knowledge about both designs as well as a lack of practical experience of many available designs. Most of these implant placement dentists in Jordan were accustomed to one or two “at most” designs, as shown by the results of the most used systems of dental implants in Jordan.
In some circumstances it has been shown that immediate loading is compatible with subsequent successful osseointegration, providing the bone quality is good and the functional forces can be adequately controlled. The latter may involve placing an adequate number of implants and connecting them together as soon as possible with a rigid framework. However, these latter protocols should be considered experimental at the present time, and there is much data to support the more cautious approach advocated by Branemark in ensuring a high level of predictable implant success [13]. Traumatic surgery, immediate loading (within 10 days of insertion), immediate implantation, early loading (within one month of insertion) were considered by most dentists as being risks for implant failure. These results were in agreement with a previous report [24].
Some implant reconstructions are designed with cantilever extensions to provide function and appearance in areas where provision of additional implants is difficult. This may be caused by practical or financial considerations. Cantilever extensions have the potential to create high loads, particularly on the implant adjacent to the cantilever. The extent of the leverage of any cantilever should be considered in relation to the anteroposterior distance between implants supporting the reconstruction. The cantilever extension should not exceed this length and the cross sectional design should be adequate to prevent flexing29. The results of the present investigation reported that the cantilever design was the most susceptible design for failure, whether it was anterior or posterior. These results were in agreement with general bio-mechanical rules suggested by a previous study [30]. The most hazardous extensions for cantilever design problems were posterior extensions. This was explained by both biomechanical rules that advise against posterior extension of the cantilever fixed bridge for more than one tooth width, and by local favourable factors in the anterior area of the jaw, where better quality and/or quantity of bone is present than in posterior area.34 It is note-worthy that angulations and anatomical structures are more challenging in the posterior area of the jaw especially in the maxilla [30].
Cantilever designs in general should be avoided, although results showed that anterior extensions and cantilever bridges in the anterior area have a better prognosis.
Conclusion
In conclusion, it appears that there is a need to increase the knowledge and awareness of dental practitioners who are practicing dental implantology in Jordan regarding the potential risk factors that could potentially impact upon implant failures through continuous dental educational programs and workshops. Regular assessment of the theoretical and practical knowledge of GDPs who practice implant dentistry is mandatory in order to improve their implant experience.
Acknowledgment
This study was funded by Department of Scientific Research at Jordan University of Science and Technology.
References
- Evian CI, Emling R, Posenberg ES, Waasdorp JA, Halpern W, et al. (2004) Retrospective analysis of implant survival and the influence of periodontal disease and immediate placement on long-term results. Int J of Oral and Maxillofac Implants 19(3): 393-398.
- Cassinelli G, Morra M, Bruzzone G, Carpi A, Di Santi G, et al. (2003) Surface chemistry effects of topographic modifications of titanium dental implants surfaces: In vitro experiments. Int J of Oral and Maxillofac Implants 18(1): 46-52.
- Morra M, Cassinelli C, Bruzzone G Carpi A, Di Santi G, et al. (2003) Surface chemistry effects of topographic modifications of titanium dental implants surfaces: Surface analysis. Int J of Oral and Maxillofac Implants 18(1): 40-45.
- Trisi P, Keith DJ, Rocco S (2005) Human histologic and histomorphometric analyses of hydroxyapatite-coated implants after 10 years of function: a case report. Int J Oral Maxillofac Implants 20(1): 124-130.
- Kunzler TP, Drobek T, Schuler M, Spencer ND (2007) Systematic study of osteoblast and fibroblast response to roughness by means of surface-morphology gradients. Biomaterials 28(13): 2175-2182.
- Calandriello R, Tomatis M, Rangert B (2003) Immediate functional loading of Brånemark System implants with enhanced initial stability: a prospective 1- to 2-year clinical and radiographic study. Clin Implant Dent Relat Res 5(1): 10-20.
- Testori T, Meltzer A, Del Fabbro M, Zuffetti F, Troiano M, et al. (2004) Immediate occlusal loading of Osseotite implants in the lower edentulous jaw. A multicenter prospective study.. Clin Oral Implants Res 15(3): 278-284.
- Testori T, Del Fabbro M, Szmukler-Moncler S, Francetti L, Weinstein RL. (2003) Immediate occlusal loading of Osseotite implants in the completely edentulous mandible. Int J of Oral and Maxillofac Implants 18(4): 544-551.
- Ashley ET, Covington LL, Bishop BG, Breault LG (2003) Ailing and failing endosseous dental implants: a literature review. J Contemp Dent Pract 15: 35-50.
- Eliasson A, Narby B, Ekstrand K, Hirsch J, Johansson A, et al. (2010) A 5-year prospective clinical study of submerged and nonsubmerged Paragon system implants in the edentulous mandible. Int J Prosthodont 23(1): 231-238.
- Sverzut AT, Stabile GA, de Moraes M, Mazzonetto R, Moreira RW (2008) The influence of tobacco on early dental implant failure. J Oral Maxillofac Surg 66(5): 1004-1009.
- Alsaadi G, Quirynen M, Komárek A, van Steenberghe D (2007) Impact of local and systemic factors on the incidence of oral implant failures, up to abutment connection. J Clin Periodontol 34(7): 610-617.
- Alsaadi G, Quirynen M, Michiles K, Teughels W, Komárek A, et al. (2008) Impact of local and systemic factors on the incidence of failures up to abutment connection with modified surface oral implants. J Clin Periodontol 35(1): 51-57.
- van Steenberghe D, Jacobs R, Desnyder M, Maffei G, Quirynen M (2002) The relative impact of local and endogenous patient-related factors on implant failure up to the abutment stage. Clin Oral Implants Res 13(6): 617-622.
- Bornstein MM1, Halbritter S, Harnisch H, Weber HP, Buser D (2008) A retrospective analysis of patients referred for implant placement to a specialty clinic: indications, surgical procedures, and early failures. Int J Oral Maxillofac Implants 23(6): 1109-1116.
- Kronström M, Svensson B, Erickson E, Houston L, Braham P, et al (2000). Humoral immunity host factors in subjects with failing or successful titanium dental implants. J Clin Periodontol 27(12): 875-882.
- Leite MF, Santos MC, de Souza AP, Line SR (2008) Osseointegrated implant failure associated with MMP-1 promotor polymorphisms (-1607 and -519).Int J Oral Maxillofac Implants 23: 653-658.
- Herrmann I, Lekholm V, Holm S, Kultje C (2005) Evaluation of impatient and implant characteristics as potential prognostic variables for oral implant failures. Int J of Oral and Maxillofac Implants 20: 220–230.
- Ridell A, Gröndahl K, Sennerby L (2009) Placement of Brånemark implants in the maxillary tuber region: anatomical considerations, surgical technique and long-term results. Clin Oral Implants Res 20(1): 94-98.
- Barone A, Orlando B, Cingano L, Marconcini S, Derchi G, et al. (2012) A randomized clinical trial to evaluate and compare implants placed in augmented versus non-augmented extraction sockets: 3-year results. J Periodontol 83(7): 836-846.
- Farzad P, Andersson L, Nyberg J (2002) Dental implant treatment in diabetic patients. Implant Dent 11(3): 262-267.
- Mellado-Valero A, Ferrer García JC, Herrera Ballester A, Labaig Rueda C (2007) Effects of diabetes on the osseointegration of dental implants. Med Oral Patol Oral Cir Bucal 12(1): E38-43.
- Granström G (2005) Osseointegration in irradiated cancer patients: an analysis with respect to implant failures. J of Oral and Maxillofac Surg 63(5):579-585.
- Mishra SK, Chowdhary R (2014) Heat generated by dental implant drills during osteotomy-a review: heat generated by dental implant drills. J Indian Prosthodont Soc 14(2): 131-143.
- Nkenke E, Lehner B, Fenner M, Roman FS, Thams U, et al. (2005) Immediate versus delayed loading of dental implants in the maxillae of mini pigs: follow-up of dental implant stability and dental implant failures. Int J of Oral and Maxillofac Implants 20(1): 39-47.
- Noguerol B, Muñoz R, Mesa F, de Dios Luna J, O'Valle F (2006) Early implant failure. Prognostic capacity of Periotest: retrospective study of a large sample. Clin Oral Implants Res 17(4): 459-464.
- Güler AU, Sumer M, Sumer P, Biçer I (2005) The evaluation of vertical heights of maxillary and mandibular bones and the location of anatomic landmarks in panoramic radiographs of edentulous patients for implant dentistry. J Oral Rehabil 32(10): 741-746.
- Wennström JL, Ekestubbe A, Gröndahl K, Karlsson S, Lindhe J (2004) Oral rehabilitation with implant-supported fixed partial dentures in periodontitis- susceptible subjects. A 5-year prospective study. J Clin Periodontol 31(9):713-724.
- Le Guéhennec L, Soueidan A, Layrolle P, Amouriq Y (2007) Surface treatments of titanium dental implants for rapid osseointegration Dent Mater 23(7): 844-854.
- Conrad HJ, Schulte JK, Vallee MC (2008) Fractures related to occlusal overload with single posterior implants: a clinical report. J Prosthet Dent 99(4): 251-256.





