Human Periodontal Ligament Cells Response to Commercially Available Calcium Hydroxide Pastes
Fahd Alsalleeh1,2, Lane. Stephenson1, Nickolas. Lyons1, Ashley. Young1, Stetson. Williams1.
1 Department of Surgical Specialties, College of Dentistry, University of Nebraska Medical Center, USA.
2 King Saud University, College of Dentistry, Restorative Dental Sciences, Saudi Arabia.
*Corresponding Author
Fahd Alsalleeh, BDS, MS, Ph.D,
University of Nebraska Medical Center,
College of Dentistry, Surgical Specialties,
Post graduate Endodontics, USA.
Tell : +1 402 472 6280; Fax: +1 402 4726681;
E-mail: fahd.alsalleeh@unmc.edu
Article Type: Research Article
Received: September 02, 2014; Accepted: October 01, 2014; Published: October 02, 2014
Citation:Fahd Alsalleeh, Lane. Stephenson, Nickolas. Lyons, Ashley. Young, Stetson. Williams. (2014) Human Periodontal Ligament Cells Response to Commercially Available Calcium Hydroxide Pastes. Int J Dentistry Oral Sci. 2(1), 6-9.doi:dx.doi.org/10.19070/2377-8075-140002
Copyright: Fahd Alsalleeh © 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Several studies have shown that calcium hydroxidebased medicaments have a cytotoxic effect on human cells. The purpose of this study was to evaluate the cytoxicity of several calcium hydroxideproducts on periodontal ligament (PDL) cells. Calcium hydroxide powder (Avantor Performance Materials Inc.), Calasept® (Nordiska Dental AB), Metapaste® (Meta Biomed Co., Ltd.), Vitapex® (Neo Dental International Inc.), Ultracal® (Ultradent Products, Inc.), and Pulpdent® (Pulpdent Corporation) products were tested. PDL cells were exposed to various concentrations of calcium hydroxidefrom each product (1.0, 0.5, 0.25, and 0.125 mg/mL). Cell viability was measured after 24 h and 48 h by Cell Proliferation Assay. All materials tested had a more toxic effect on PDL cells after 48 h.At 24 and 48 h, Metapaste® was the most toxic regardless of concentrations used. Products with a1.0 and 0.5 mg/mL concentration hadstatistically significant more cytotoxic effectswhen compared to the negative control. Pure calcium hydroxide and Calacept® induced 35% cell death at a 1 mg/mL concentration and 15-20% cell death at 0.5, 0.25, and 0.125 mg/mL after 24 h. Pulpdent® and Ultracal® induced 30-35% cell death at a 1 mg/mL concentration and its effect diminished at 0.25 and 0.125 mg/mL at 24 h. The Vitapex® preparation induced 20% PDL cell death at 24 h regardless of the concentration and was the least toxic significantly at 1 mg/mL compared to other brands, except Pulpdent®, at the same concentration at 24 h.All calcium hydroxideproducts showed evidence of cytoxicity on PDL cells, with Metapaste being the most cytotoxic. The cytotoxicity was related to concentration and exposure time. Pulpdent® and Ultracal® had excellent biocompatibility at lower concentrations.
2.Introduction
3.Methods
3.1 Calcium hydroxide brands used
3.2 Sample preparation, pH readings and cell proliferation assay
3.3 Data analysis
4.Results
4.1 MSDS data and pH measurement
4.2 PDL cells Proliferation
5.Discussion
6.Acknowledgments
7.References
Keywords
Cytotoxicity; Calcium hydroxide; Human cells; Fibroblasts.
Introduction
Calcium hydroxide is the de facto standard intracanal medicament for root canal disinfection and the promotion of chronic apical periodontitis healing [1-3]. At first, clinicians were mixing calcium hydroxide with water to produce an aqueous paste. Then, several studies tested different vehicles and formulations to improve handling properties, antibacterial actions, physical behavior, and radiopacity. Currently, there are several commercial preparations available [4]. The biological consequences of different mixing vehicles are not fully understood.
The basic mechanism action of calcium hydroxide is based on the dissociation of Ca2+ and OH- ions. The outcome of such dissociation results in an elevated pH. Calcium hydroxide has been shown to have antimicrobial activity when used clinically or with in vitro models.Intracanal calcium hydroxide rendered infected root canals free of cultivable bacteria after seven days [2,5]. It has been shown that 92.5% of canals become bacteria free using the same protocol [6]. However, others have shown that calcium hydroxide application between appointments did not have any effect on disinfecting canals or treatment outcome[7,8]. Furthermore, a more recent systematic review of eight clinical trials indicated that calcium hydroxide was ineffective in eliminating bacteria from infected root canals[9]. The differences in these studies may be attributed to the different calcium preparations used. It was suggested that certain vehicles may decrease the antimicrobial effectiveness of calcium hydroxide[10]. Nevertheless, studies are lacking to compare antimicrobial activities of different calcium hydroxide preparations.
It is well known that calcium hydroxide is cytotoxic. Several in vitro/ex vivo and animal studies were conducted to test individual products. Intracanal medicaments are usually confined within the root canal system. Yet, through extrusion, calcium hydroxide may invade the periapical tissues. Some authors have advocated such practices to improve the outcome of teeth with periapical lesions and thus change the environment of chronically inflamed tissue and epithelial cystic linings[11]. But, case reports have alluded to bone necrosis and neurotoxicity as a result of this approach[12]. The lack of periapical healing and more complications have been reported after the extrusion of calcium hydroxide[13]. Others have shown that sealer containing calcium hydroxide had a toxic effect on rat sciatic nerve, yet it appeared this effect diminished after 60 minutes[14,15]. Direct contact of calcium hydroxide with nerve tissue for 30 minutes caused irreversible damage [15]. Periodontal ligament cells (PDL cells) play a crucial role in the regeneration and repair process of chronic apical periodontitis[16]. Due to the fact that any intracanal medicaments used will come in close contact or accidentally injected outside the root canal system, it should not prevent nor interfere the healing process or be toxic to PDL cells[17]. Therefore, the present study was designed to evaluate the cytoxicity of several calcium hydroxide products on primary PDL cells.
Six brands of commercially available dental calcium hydroxide medicaments were purchased. Calcium hydroxide powder (Avantor Performance Materials Inc.), Calasept® (Nordiska Dental AB), Metapaste® (Meta Biomed Co., Ltd.), Vitapex® (Neo Dental International Inc.), Ultracal® (Ultradent Products, Inc.), and Pulpdent® (Pulpdent Corporation) products were selected. All material safety data sheet (MSDS) were obtained from the manufacturer’s websites.
All calcium hydroxide products were mixed with culture media (Dulbecco's modified Eagle's medium culture medium (Life Technologies, NY) supplemented with antibiotics and 10% fetal bovine serum (FBS). Each product was serially diluted at ratios of 1.0, 0.5, 0.25, and 0.125 mg/mL. The pH of each preparation was measured using Accumet basic pH meter (Waltham, MA).
PDL cells were obtained from ScienCell (Carlsbad, CA) and grown in complete Dulbecco's modified Eagle's culture medium (Life Technologies, NY) supplemented with antibiotics and 10% FBS at 37°C in a humidified 5% CO2 atmosphere incubator. Cells between the 4th and 6th passages were used. A total of 15 x 103 PDL cells were plated in culture medium onto 96-well plates and grown overnight to allow adherence to the surface.
For the experimental groups, different calcium hydroxide brands of various concentrations were added to each well. PDL cells treated with 6% sodium hypochlorite served as the positive control. PDL cells kept in fresh medium served as the negative control. After 24 and 48 h, PDL cells proliferation was evaluated by CellTiter96 AQueous Non-Radioactive Cell Proliferation Assay (Madison, WI), composed of [3-(4,5-dimethylthiazol-2-yl)-5-(3- carboxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium, inner salt; MTS], according to the manufacturer’s instructions. The optical density (OD) values for each well were measured spectrophotometrically at 490 nm.
Six brands of commercially available dental calcium hydroxide medicaments were purchased. Calcium hydroxide powder (Avantor Performance Materials Inc.), Calasept® (Nordiska Dental AB), Metapaste® (Meta Biomed Co., Ltd.), Vitapex® (Neo Dental International Inc.), Ultracal® (Ultradent Products, Inc.), and Pulpdent® (Pulpdent Corporation) products were selected. All material safety data sheet (MSDS) were obtained from the manufacturer’s websites.
Relevant clinical data on the material safety data sheet of each product was summarized in table 1. The highest concentration calcium hydroxide was reported in the pure USP brand, followed by Pulpdent® which reported 42%. Other brands ranged from 30-35%. Calacept®, Ultracal®, and Pulpdent® are aqueous preparations. The use of propyleneglycol makes Metapaste® a viscous preparation and reports an unspecified calcium hydroxide percentage. Vitapex® contains 40% idoform and silicone oil as a carrier.
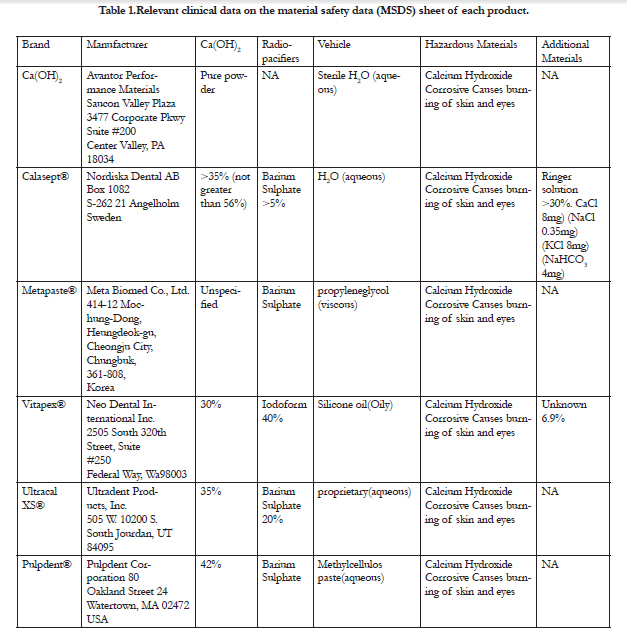

Table 1.Relevant clinical data on the material safety data (MSDS) sheet of each product.
The pH readings of all materials tested with different concentrations were shown in table 2. Pure calcium hydroxide had the highest pH reading. Metapaste® and Vitapex® were the lowest. The pH readings were lower as the concentration of materials tested decreased.
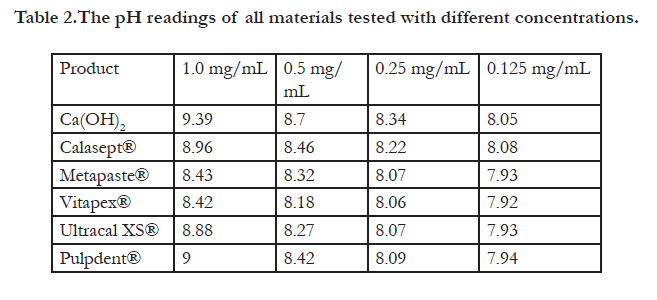
Table 2.The pH readings of all materials tested with different concentrations.
All materials tested had a more toxic effect on PDL cells after 48h (Fig. 1a). At 24 and 48 h, Metapaste® was the most toxic regardless of the concentration used. Interestingly enough, the Metapaste ® at 0.125 mg/mL was significantly more toxic than other brands at 1 mg/mL at the 24 and 48 h intervals (Fig. 1b& c). Pure calcium hydroxide mixed with water and Calacept® induced 35% cell death at a 1 mg/mL concentration and 15-20% cell death at 0.5, 0.25, and 0.125 mg/mL after 24 h (Fig. 1b). Pulpdent® and Ultracal® appeared to have similar outcomes on PDL cell death. Both induced 30-35% cell death at a 1 mg/mL concentration and its effect diminished at 0.25 and 0.125 mg/mL at 24 h (Fig. 1b). The Vitapex® preparation induced 20% PDL cell death at 24 h regardless of the concentration. Furthermore, Vitapex® was the least toxic significantly at 1 mg/mL compared to other brands, except Pulpdent®, at the same concentration at 24 h (Fig. 1b). At 48 h, all brands, except Metapaste®, had very similar toxic effect (Fig. 1c). Sodium hypochlorite at 6% induced 100% cell death at 24 and 48 h (data no shown).
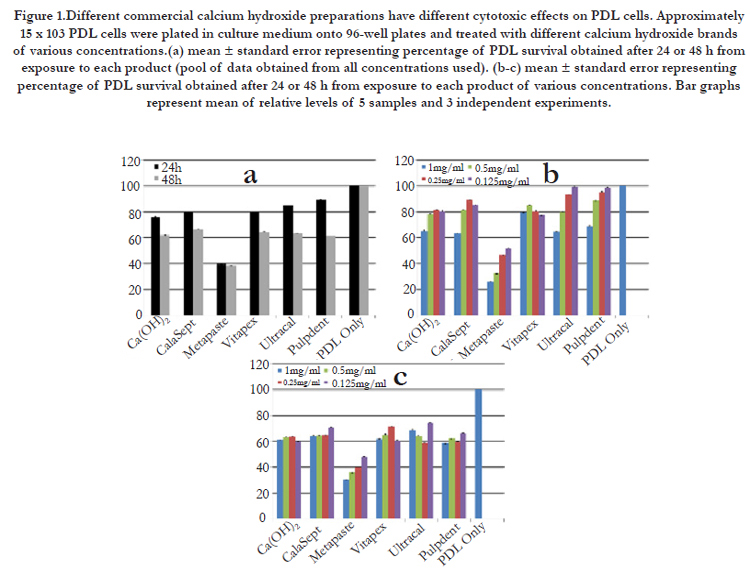
Figure 1.Different commercial calcium hydroxide preparations have different cytotoxic effects on PDL cells. Approximately 15 x 103 PDL cells were plated in culture medium onto 96-well plates and treated with different calcium hydroxide brands of various concentrations.(a) mean ± standard error representing percentage of PDL survival obtained after 24 or 48 h from exposure to each product (pool of data obtained from all concentrations used). (b-c) mean ± standard error representing percentage of PDL survival obtained after 24 or 48 h from exposure to each product of various concentrations. Bar graphs represent mean of relative levels of 5 samples and 3 independent experiments.
Discussions
The antimicrobial effect of calcium hydroxide has been studied extensively with different outcomes. Early studies reported high success with the use of calcium hydroxide[2]. However, a more recent systematic review of eight clinical trials indicated that calcium hydroxide is ineffective in eliminating bacteria from infected root canals[18]. The early studies used pure calcium hydroxide mixed in-office. Currently, commercial preparations are convenient to use. The antimicrobial effect of calcium hydroxide may be compromised when using different delivery vehicles[10]. The present study, for the first time, compares the cytoxicity of several commercial preparations on PDL cells. PDL cells are crucial during the early infection as well as the resolution stage of infection at the root surfaces[16]. Therefore, it would be prudent to use a product that is least toxic to the PDL cells. Moreover, it would be interesting to evaluate the anti-microbial effect of the least toxic commercial calcium hydroxide product in the future.
As endodontists, the intention is to keep any intracanal medicaments within the root canal system. Yet, calcium hydroxide may extrude beyond the apical foramen. Some authors have advocated such practices to improve the outcome of teeth with periapical lesions to change the environment of chronically inflamed tissue and epithelial cystic linings [11]. Furthermore, emerging evidence indicates that calcium hydroxide has an application in endodontic regeneration[19-21]. Calcium hydroxide significantly increased the proliferation of stem cells of apical papilla[22]. The present study demonstratedthat different preparations have different effects on PDL cell survival, regardless of concentration. Metapaste® was the most toxic and had lower pH readings compared to others. It is considered a viscous preparation, in which propyleneglycol is used as the vehicle and barium sulphate for radiopacity. The results presented suggest that the toxic effect was not only due to calcium hydroxide, but from other component(s), especially those in Metapaste®.
It appears that Ultracal® and Pulpdent® have the least toxic effect at 0.25 and 0.125 mg/mL. Both brands are considered aqueous preparations that facilitate the dissociation reaction required for calcium hydroxide to be effective [23]. It should be noted that the pH of these concentrations is close to 8. With emerging evidence of extra radicular microorganisms and biofilms, it would be advantageous to use a preparation with the least toxic effect on the host.
In conclusion, different commercial calcium hydroxide preparations have different cytotoxic effects on PDL cells, with Pulpdent ® and Ultracal® exhibiting excellent biocompatibility at lower concentrations.
Acknowledgments
The study was supported by American Association Foundation and departmental funds. The authors deny any conflicts of interest.
References
- Bystrom A, Claesson R , Sundqvist G (1985) The antibacterial effect of camphorated paramonochlorophenol, camphorated phenol and calcium hydroxide in the treatment of infected root canals. Endod Dent Traumatol 1:170-175.
- Sjogren U,Figdor D, Persson S, Sundqvist G(1997) Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J, 30: 297-306.
- Trope M , Delano E.O, Orstavik D (1999) Endodontic treatment of teeth with apical periodontitis: single vs. multivisit treatment. J Endod 25: 345-350.
- Fava L.R, Saunders W.P(1999) Calcium hydroxide pastes: classification and clinical indications. Int Endod J 32: 257-282.
- Sjogren U , Figdor D , Spangberg L,Sundqvist G(1991) The antimicrobial effect of calcium hydroxide as a short-term intracanal dressing. Int Endod J 24: 119-125.
- Shuping G.B, Orstavik D , Sigurdsson A, Trope M (2000) Reduction of intracanal bacteria using nickel-titanium rotary instrumentation and various medications. J Endod 26:751-755.
- Waltimo T , Trope M , Haapasalo M,Orstavik D (2005) Clinical efficacy of treatment procedures in endodontic infection control and one year followup of periapical healing. J Endod 31: 863-866.
- Peters L.B, Wesselink P.R (2002) Periapical healing of endodontically treated teeth in one and two visits obturated in the presence or absence of detectable microorganisms. Int Endod J 35: 660-667.
- Sathorn C, Parashos P, Messer H.H (2005) Effectiveness of single- versus multiple-visit endodontic treatment of teeth with apical periodontitis: a systematic review and meta-analysis. Int Endod J 38: 347-355.
- Safavi K, and Nakayama T.A (2000) Influence of mixing vehicle on dissociation of calcium hydroxide in solution. J Endod 26: 649-651.
- Tronstad L, Andreasen J.O, Hasselgren G, Kristerson L, Riis I (1981) pH changes in dental tissues after root canal filling with calcium hydroxide. J Endod 7: 17-21.
- Himel V.T, Brady J, Jr. and Weir, J., Jr. (1985) Evaluation of repair of mechanical perforations of the pulp chamber floor using biodegradable tricalcium phosphate or calcium hydroxide. J Endod 11: 161-165.
- Ioannidis K , Lambrianidis T , Beltes P, Besi E, Malliari M (2011) Endodontic management and cone-beam computed tomography evaluation of seven maxillary and mandibular molars with single roots and single canals in a patient. J Endod 37:103-109.
- Serper A, Ucer O, Onur R, Etikan I (1998) Comparative neurotoxic effects of root canal filling materials on rat sciatic nerve. J Endod 24:592-594.
- Boiesen J, Brodin P (1991) Neurotoxic effect of two root canal sealers with calcium hydroxide on rat phrenic nerve in vitro. Endod Dent Traumatol 7:242-245.
- Jonsson D, Nebel D, Bratthall G, NilssonB.O (2011) The human periodontal ligament cell: a fibroblast-like cell acting as an immune cell. J Periodontal Res 46:153-157.
- Huang F.M, Tai K.W, Chou M.Y,Chang Y.C (2002) Cytotoxicity of resin-,zinc oxide-eugenol-, and calcium hydroxide-based root canal sealers on human periodontal ligament cells and permanent V79 cells. Int Endod J 35:153-158.
- Sathorn C, ParashosP, MesserH (2007) Antibacterial efficacy of calcium hydroxide intracanal dressing: a systematic review and meta-analysis. Int Endod J 40:2-10.
- Chueh L.H, Ho Y.C, KuoT.C, LaiW.H, Chen Y.H et al. (2009) Regenerative endodontic treatment for necrotic immature permanent teeth. J Endod 35: 160-164.
- Bose R, Nummikoski P, Hargreaves K (2009) A retrospective evaluation of radiographic outcomes in immature teeth with necrotic root canal systems treated with regenerative endodontic procedures. J Endod 35: 1343-1349.
- Cehreli Z.C, Isbitiren B, Sara S ,Erbas G (2011) Regenerative endodontic treatment (revascularization) of immature necrotic molars medicated with calcium hydroxide: a case series. J Endod 37:1327-1330.
- Ruparel N.B, Teixeira F.B, Ferraz C.C, Diogenes A (2012) Direct effect of intracanal medicaments on survival of stem cells of the apical papilla. J Endod 38: 1372-1375.
- Mohammadi Z, DummerP.M (2011) Properties and applications of calcium hydroxide in endodontics and dental traumatology. Int Endod J 44: 697-730.





