Evaluation of Symptoms and Characteristic Features of Lead Poisoning and their Assistance in Clinical Decision Making
D'souza HS1*, Menezes G2, Dsouza SA3, Venkatesh T4
1 Associate Professor, Department of Biotechnology, School of Life Sciences, Manipal University, Manipal, India.
2 Associate Professor, Faculty NRCLPI, Department of Biochemistry & Biophysics, St. John’s Medical College, Koramangala, Bangalore, India.
3 Professor and Head, Department of Occupational Therapy, School of Allied Health Sciences, Manipal University, Manipal, India.
4 Director - NRCLPI, St. John’s Medical College, Koramangala, Bangalore, India.
*Corresponding Author
Herman Sunil D’souza,
Associate Professor,
Department of Biotechnology,
School of Life Sciences,
Manipal University, Manipal, India.
Tel: 0091-820-2922058/0091-09448017901
Fax: 0091-820-2571919
E-mail: hsdsouza@gmail.com
Received: August 12, 2015; Accepted: September 09, 2015; Published: September 10, 2015
Citation: D'souza HS, Menezes G, Dsouza SA, Venkatesh T (2015) Evaluation of Symptoms and Characteristic Features of Lead Poisoningand their Assistance in Clinical Decision Making. Int J Clin Ther Diagn 3(5), 97-99. doi: dx.doi.org/10.19070/2332-2926-1500020.
Copyright: D'souza HS© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aim of the present study is to evaluate the symptoms and characteristics features in lead based industrial workers and accessing their reliability in clinical decision making and diagnosing lead toxicity. Study involves 15 industrial workers (exposed) and 15 non-exposed individuals, matched for age, sex and nationality selected from Bangalore, India. Association of various symptoms and characteristic features in exposed and non-exposed groups were evaluated and their association with high blood lead levels was studied. Exposed individuals had significantly higher blood lead levels (114.13 ± 39.95 μg/ dl) than non-exposed (5.47 ± 2.00 μg/dl). Corresponding with increase in lead levels, a decrease in hemoglobin and increase in zinc protoporphyrin levels were seen in all exposed individuals. Specific symptoms of lead poisoning such as wrist drop was seen in 33.3% and blue line on gums and basophilic stippling was seen in 26.7% of lead exposed industrial workers. Though the reported general symptoms of lead poisoning like weakness, abdominal colic, constipation, insomnia, dizziness, generalized body ache, loss of appetite, anxiety were strongly associated with high blood lead levels, similar symptoms were also seen in non-exposed individuals. Lead exposed industrial workers had higher prevalence of symptoms observed. Proper diagnosis of lead poisoning based only on symptoms may not be possible. Despite high blood lead levels, the specific symptoms of lead poisoning are not apparent, hence many cases of lead poisoning remain undiagnosed and untreated or might receive only symptomatic treatment. Estimating blood lead levels and correlating with specific symptoms may help diagnosing patients with lead poisoning and subsequent intervention.
2.Introduction
3.Materials and Methods
4.Results and Discussion
5.References
Keywords
Lead Poisoning; Blood Lead Level; Zinc Protoporphyrin; Anemia; Basophilic Stippling; Wrist Drop.
Introduction
Chronic exposure to lead has been a matter of public health of global proportion. Most significant way of exposure for occupationally exposed adults, is inhalation of dust and fumes contaminated with lead, particularly during battery manufacturing, mining, smelting, printing, pottery glazing and refining operations, reclamation operations, alloying, casting, abrasive blasting [1-3]. Lead poisoning cases are seen in all age groups causing serious health hazards, especially in lead-based industrial workers, where many of them are unaware of the risks of exposure to high levels of lead. Many organs or organ systems have been potential targets for lead in the body, including haematopoietic, neurological, skeletal, reproductive, gastrointestinal, immune and renal systems and might even cause chromosomal aberrations [4-6]. Many cases of lead poisoning do not show specific symptoms like blue lines on gum, basophilic stippling and wrist drop. The general symptoms shown are mimicking that of other disorders making the diagnosis very difficult, hence many of the cases remain undiagnosed and untreated or might receive only symptomatic treatment [7].
Materials and Methods
Study included 15 lead based industrial workers and equal number of age and sex matched controls. All subjects included in the study were working for 7 to 8 hours a day for more than 5 years. Standard questionnaires were used to interview each individual. Information related to their working environment, personal protective equipment, personal hygiene and habits and working hours/day was collected. Written informed consent was obtained from all the individuals participated in the study before collecting blood sample and for the publication of the data generated. Association of various symptoms and characteristic features in exposed and non-exposed groups was evaluated and their association with high blood lead levels was studied. ESA model 3010B lead analyzer was used to estimate blood lead levels (PbB), which uses the principle of differential pulse anodic stripping voltammetry (DPASV). AVIV model 206 Hematofluorometer was used to estimate Zinc protoporphyrin (ZPP), which works on the principle of front surface fluorometry. Hemoglobin (Hb) was estimated by colorimetry using Drabkin's reagent. Statistical analysis was carried out using unpaired Student’s t-test and Mann-Whitney U test. Significance in the effects was considered as follows: p ≤ 0.001- very highly significant; p ≤ 0.01- highly significant; p ≤ 0.05 significant; p > 0.05- 0.1 - possibly significant; p > 0.1- NS (not significant). Odds ratio with 95% confidence interval (CI) was used to show the prevalence frequency.
Results and Discussion
Study was conducted in 15 lead based industrial workers and equal number of controls. The controls did not have any known source of lead exposure. Both groups had a mean work experience of more than 5 years. Despite a difference in mean work experience of 9.86 years in exposed and 6.86 years in non-exposed, the nonparametric Man-Whitney U test showed no statistical significance (p = 0.267) between the two groups.
Table 1 shows measurements of indicators of lead poisoning PbB, ZPP, Hb and Blood pressure (BP) in both groups. The exposed group showed a significant elevation (p < 0.001) in PbB and ZPP levels. Chronic lead toxicity in the exposed group was indicated by increase in mean PbB and ZPP levels more than 100 μg/dl, the elevations being 20 and 3.8 fold respectively. A significant decrease (p < 0.001) in Hb levels was seen in exposed group. The decrease amounted to 28%. Further, exposed group showed a significant variation (p < 0.001) in systolic and diastolic BP, the decrease being 11.6% and 17.7% respectively.
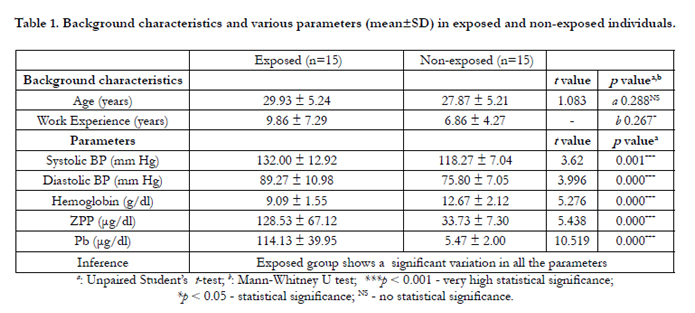

Table 1.Background characteristics and various parameters (mean±SD) in exposed and non-exposed individuals.
Table 2 indicates association of various symptoms and characteristic features in exposed and non-exposed groups. Amongst the general symptoms in the exposed group, constipation dominated (86.7%), followed by dizziness, generalized body ache, abdominal colic (66.7%), weakness and insomnia (60%).
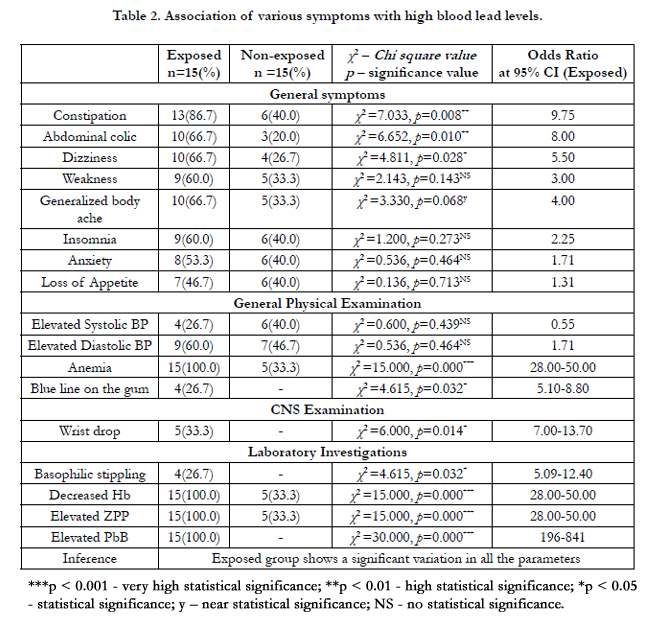
Table 2. Association of various symptoms with high blood lead levels.
The odds ratios for constipation and abdominal colic were 9.75 and 8.0 with 95% CI respectively, indicating frequency of occurrence of constipation in lead exposed individuals is 9.75 and abdominal pain is 8.0 times higher compared to non-exposed. Odds ratios for various other symptoms are showed in Table 2. General physical and CNS examination showed anemia in all exposed workers (p < 0.001), with odds ratio indicating that anemia is 28- 50 times more likely to occur in lead exposed workers with PbB levels of 100μg/dl and more. Anemia was seen in only 33.3% of the non-exposed individuals. Though elevated systolic and diastolic BP was shown by both groups, exposed group presented with higher diastolic BP (60%). The increased BP among the lead exposed workers in this study also agrees with the observations of other reported studies [8]. Blue line on the gum (p < 0.05) was seen in 4 (26.7%) and wrist drop (p < 0.05) in 5 (33.3%) of the lead exposed workers.
Amongst the laboratory parameters, elevated PbB (p < 0.001), ZPP (p < 0.001) and Hb (p < 0.01) was seen in all exposed workers (100%) while only 26.7% showed basophilic stippling (p < 0.05). 33.3% non-exposed individuals, were having anemia with Hb levels of 9.09 ± 1.55 g/dl, which was further confirmed by elevated ZPP levels. Increase in ZPP levels in 5 of the non-exposed individual is because of anemia, since iron deficiency anemia will lead to increased production of ZPP [9]. ZPP which is used as a tool for predicting lead exposure has its limitations because of its elevation in individuals with anemia as observed in the present study.
PbB levels of exposed workers, working in different sections of the battery factories and small scale industries were observed to be very high and alarming (Table 1). General symptoms of lead poisoning evaluated in this study are seen both in lead exposed and non-exposed group, indicating proper diagnosis of lead poisoning based on these symptoms may be challenging. Despite of elevated blood lead levels, specific symptoms of lead poisoning like wrist drop was seen in 33.3% and the blue line on the gum and basophilic stippling was seen in only 26.7% of lead exposed workers. Thus based on absence of these findings one cannot rule out lead poisoning (Table 2). Lead poisoning cases have no specific symptoms, leading to delay in diagnosis or might go undiagnosed or misdiagnosed receiving only symptomatic treatment leading to death in few cases [7, 10]. It would be appropriate to consider the potentially hazardous sources of lead exposure while medically evaluating lead poisoning cases. Since in most of the cases, the symptoms of lead poisoning mimic that of other disorders, the best screening and diagnostic tool for clinical decision making appears to be estimating blood lead levels.
References
- Menezes G, D’souza HS, Venkatesh T (2003) Chronic lead poisoning in an adult battery worker. Occup Med (Lond) 53(7): 476-478.
- Gottesfeld P, Pokhrel AK (2011) Review: Lead exposure in battery manufacturing and recycling in developing countries and among children in nearby communities. J Occup Environ Hyg 8(9): 520-532.
- Kasuba V, Rozga JR, Milic M, Zeljezic D, Kopjar N, et al. (2012) Evaluation of genotoxic effects of lead in pottery-glaze workers using micronucleus assay, alkaline comet assay and DNA diffusion assay. Int Arch Occup Environ Health 85(7): 807-818.
- Herman SD, Geraldine M, Venkatesh T (2002) Fetal lead exposure: encephalopathy in a child. Indian J Clin Biochem 17(1): 9-11.
- Madhavi D, Devi KR, Sowjanya BL (2008) Increased frequency of chromosomal aberrations in industrial painters exposed to lead-based paints. J Environ Pathol Toxicol Oncol 27(1): 53-59.
- Jusko TA, Henderson CR Jr, Lanphear BP, Cory-Slechta DA, Parsons PJ, et al. (2008) Blood lead concentrations < 10 μg/dL and child intelligence at 6 Years of age. Environ Health Perspect 116(2): 243-248.
- Dedeken P, Louw V, Vandooren AK, Verstegen G, Goossens W, et al. (2006) Plumbism or lead intoxication mimicking an abdominal tumor. J Gen Intern Med 21(6): C1-3.
- Vupputuri S, He J, Muntner P, Bazzano LA, Whelton PK, et al. (2003) Blood lead level is associated with elevated blood pressure in blacks. Hypertension 41(3): 463-468.
- Baart AM, de Kort WL, Moons KG, Atsma F, Vergouwe Y (2013) Zinc protoporphyrin levels have added value in the prediction of low hemoglobin deferral in whole blood donors. Transfusion 53(8): 1661-1669.
- Berkowitz S, Tarrago R (2006) Acute brain herniation from lead toxicity. Pediatrics 118(6): 2548-2551.





