Non-Invasive Assessment of the Autonomic Nervous System
Jamie M. O’ Driscoll1,2, Sharma R1*
1 Department of Cardiology, St George’s Healthcare NHS Trust, Tooting, London, UK.
2 Canterbury Christ Church University, School of Human and Life Sciences, London, UK.
*Corresponding Author
Dr Rajan Sharma,
Department of Cardiology,
St George’s Healthcare NHS Trust, Blackshaw Road,
Tooting, London, SW17 0QT, UK.
Tel: +44 (0)2087250286; Fax: +44 (0)2087254402
E-mail: rajan.sharma@stgeorges.nhs.uk
Received: May 27, 2015; Accepted: July 04, 2015; Published: July 06, 2015
Citation: Jamie M. O’ Driscoll, Sharma R (2015) Non-Invasive Assessment of the Autonomic Nervous System. Int J Clin Ther Diagn 3(3), 85-91. doi: dx.doi.org/10.19070/2332-2926-1500017
Copyright: Sharma R© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Autonomic dysfunction is associated with worse outcome in many disease states. Invasive assessment is time consuming and rarely used in the clinical setting. However, autonomic data can also be derived non-invasively from beat to beat analysis of heart rate and blood pressure. Computer based software (power spectral analysis) permits real time analysis of heart rate variability in the frequency domain. This article explores the principles and practice of non-invasive autonomic function assessment and the consequences of changes in autonomic tone seen in disease states associated with increased cardiovascular disease morbidity and mortality.
2.Introduction
3.Autonomic Assessment with Power Spectral Analysis
3.1.Deep Breathing
3.2.Valsalva Maneuver
3.3.Sustained Hand Grip
3.3.Active Orthostasis
4.Cardiovascular Autonomic Neuropathy
4.1.Hypertension
4.2.Ischaemic Heart Disease
4.3.Myocardial Infarction
4.4.Chronic Heart Failure
5.Diabetic Autonomic Neuropathy
6.Renal Autonomic Neuropathy
7.Limitations
8.Conclusion
9.References
Keywords
Autonomic Function; Cardiovascular Disease; Heart Rate Variability; Power Spectral Analysis.
Introduction
The autonomic nervous system (ANS) has a fundamental role in vmaintaining homeostasis of the human body through continually adjusting the functions of various organs in response to changing internal and external conditions. The relative reactions or changes induced by the ANS to maintain homeostasis is coupled with almost all physiological and therefore pathological conditions.
The ability to reliably quantify the dynamics of the ANS is crucial for examining ANS dysfunction associated diseases. The activity of the ANS can be determined by measuring cardiac noradrenaline spill overflow to plasma using isotope dilution or by measuring muscle sympathetic nerve activity by microneurography. However, these methods are invasive and precluded from use in outpatient settings. There are non-invasive methods used to measure autonomic activity that include time domain, frequency domain, and non-linear phenomena, which are comprehensively described elsewhere [1]. Non-invasive devices can continuously monitor and accurately measure autonomic function by using sophisticated algorithms, such as power spectral analysis (PSA), housed in computer software. PSA can be derived from both nonparametric (fast Fourier transform [FFT]) and parametric (autoregressive model) methods, which in the majority of instances provide comparable results. Baroreceptor reflex sensitivity (BRS) provides a measure of the reflex arc that adjusts heart rate (HR) in response to changes in blood pressure (BP). Techniques used to measure the integrity of BRS function include the phenylephrine bolus technique (invasive), cross spectral technique, and sequence technique method, which are described elsewhere [2]. The application of clinical methods designed to quantify ANS activity has led to an enormous understanding of human ANS physiology and pathophysiology in the study of disease, most notably of the cardiovascular system. This knowledge may be used for early clinical intervention.
Cardiovascular disease (CVD), diabetes and renal dysfunction are examples of disorders that have been known to alter ANS balance, resulting in sympathetic predominance, which has been associated with an unfavourable outcome and promote the occurrence of life-threatening arrhythmias. In addition a reduced BRS is a marker of depressed vagal reflexes and associated with an increased risk of mortality. Amplified parasympathetic modulation may exert a protective anti-arrhythmic effect.
Autonomic Assessment with Power Spectral Analysis
Several investigators have studied the mechanisms involved in the cardiovascular regulation by means of beat-to-beat variability analysis of both HR and BP [3]. Spectral analysis (frequency domain) of heart rate variability (HRV) and blood pressure variability (BPV) were used for the first time in 1968 and 1978 respectively [3] and have subsequently become commonly used non-invasive methods of quantifying the autonomic modulation of the cardiovascular system. The main advantage of PSA of signals is the possibility to study their frequency specific oscillations. Therefore, not only can the degree of variability from the measurements be obtained, but the oscillating frequency can also be obtained.
PSA involves degeneration of the haemodynamic parameters into a sum of waves (sinusoidal) of different amplitude and frequencies, thus the results can be displayed with the magnitude of variability as a function of frequency (power spectrum) [4]. Therefore, the power spectrum reflects the amplitude of the haemodynamic fluctuations at different oscillation frequencies and provides the ability to divide the sympathetic and parasympathetic stimulations on the heart into distinct frequencies [4], which is a technique that may provide clarification of the pathogenesis of disease and the role of the ANS [1].
PSA of cardiovascular signals has grown considerably since the recognition that haemodynamic variability has become a substantial diagnostic tool for the detection of dysautonomia and therefore its application is of significant clinical importance. PSA techniques used to determine HRV and BPV usually focus on variability components with frequencies ranging between 0.025 and 0.50 Hz, specifically 0.04 – 0.15 Hz for low frequency (sympathetic cardiovascular modulation) and 0.15 – 0.4 Hz for high frequency (parasympathetic cardiovascular modulation), which is based on the evidence that within these frequency ranges, HR and BP are modulated by neural autonomic influences [5].
Autonomic Function Testing Procedures
Ewing and colleagues introduced physiological stress manoeuvres for studying autonomic function (Ewing battery) [6]. These tests assess the integrity of parasympathetic and sympathetic nerve activity and have been widely accepted as a means to classify autonomic neuropathy in terms of its severity.
With an intact parasympathetic nerve supply, HR varies during inspiration and expiration. The variation in HR can be studied during quiet deep breathing, with six breaths.min-1 the most rereproducible method. In the semi-recumbent position, the patient breathes deeply at six breaths.min-1 (five seconds for inspiration and five seconds for expiration) and a continuous electrocardiogram records HR variation during the manoeuvre. The RR-intervals (RRI) during inspiration and expiration are calculated and the result is expressed as the mean difference between maximum and minimum heart rates for the manoeuvre. Normal values are ≥ 15 beats.min-1, borderline values are 11-14 beats.min-1 and abnormal values are ≤ 10 beats.min-1. Patients with diabetes with autonomic neuropathy may have a reduction in, and sometimes complete absence of HR variation [6].
To perform the Valsalva, the patient blows with an open glottis into a disposable syringe connected to a mercury column of a sphygmomanometer and maintains a forced expiratory pressure of 40 mmHg for 15-seconds. During the strain period of the Valsalva manoeuvre there are 4-distinct phases of HR and BP changes (Figure 1). At phase 1, there is a brief increase in BP and a reflex fall in HR due to compression of the aorta. At phase 2, there is an early fall in BP with a subsequent recovery later in this phase. The BP changes are accompanied by an increase in HR. At phase 3, BP falls for 1-2 seconds and HR increases with cessation of expiration, and at phase 4, BP increases (overshoot) above baseline values because of delayed vasoconstriction and restored cardiac output. The BP overshoot causes a decrease in HR due to baroreflex control mechanisms.
The Valsalva ratio is calculated by the ratio of the longest RRI post-manoeuvre, reflecting the bradycardic response to the BP overshoot, to the shortest RRI during the manoeuvre, reflecting the tachycardia during strain. Abnormal values are a ratio below 1.1.
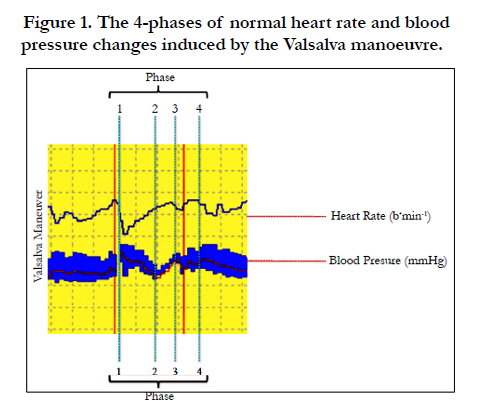
Figure 1. The 4-phases of normal heart rate and blood pressure changes induced by the Valsalva manoeuvre.
The sustained handgrip test provides valuable evidence for the function of the efferent sympathetic nervous system. The maximum voluntary contraction is determined using a handgrip dynamometer and the handgrip is maintained at 30% of that maximum for 5-minutes. During sustained muscle contraction there is an increase in BP, primarily through an increased HR and cardiac output with little change in peripheral vascular resistance. The normal response is a ≥ 16 mmHg increase in diastolic BP, whereas a response ≤ 10 mmHg is considered abnormal. In weak and elderly patients the sustained handgrip test can be replaced by the cold pressor test.
During the change from supine to standing there is a characteristic immediate increase in HR, which is maximal at approximately the 15th beat post-standing. A relative bradycardia then occurs, which is maximal at approximately the 30th beat post-standing. This response is mediated by the vagus nerve. The test is performed with the patient lying quietly on a couch with continuous monitoring and then asked to stand up unaided. The shortest RRI at approximately the 15th beat and the longest RRI at approximately the 30th beat post-standing are recorded and the characteristic HR response is expressed by the 30:15 ratio. Normal value is a ratio > 1.04, borderline ratio 1.01-1.03 and abnormal if the ratio is < 1.00. For sympathetic function, the result of the test is considered normal when the systolic BP decreases < 10 mmHg, borderline 11-29 mmHg and abnormal if systolic BP falls by 30 mmHg within 3-minutes post-standing.
The AFT results can be categorized into four groups: normal; early parasympathetic damage, where one of the three parasympathetic AFT are abnormal; definite parasympathetic damage, where two or more of the parasympathetic AFT are abnormal; and combined parasympathetic and sympathetic damage, where in addition to abnormal parasympathetic function one or both sympathetic tests are abnormal. Figure 2 illustrates the normal autonomic response to the Ewing battery of tests and Figure 3 illustrates the power spectral analysis of a patient with normal autonomic function compared with a patient with autonomic failure.
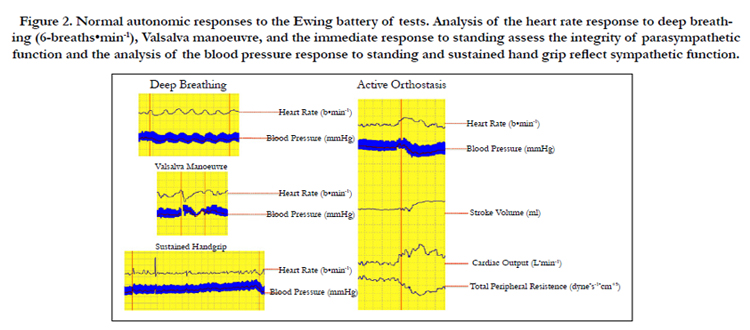
Figure 2. Normal autonomic responses to the Ewing battery of tests. Analysis of the heart rate response to deep breathing (6-breaths•min-1), Valsalva manoeuvre, and the immediate response to standing assess the integrity of parasympathetic function and the analysis of the blood pressure response to standing and sustained hand grip reflect sympathetic function.
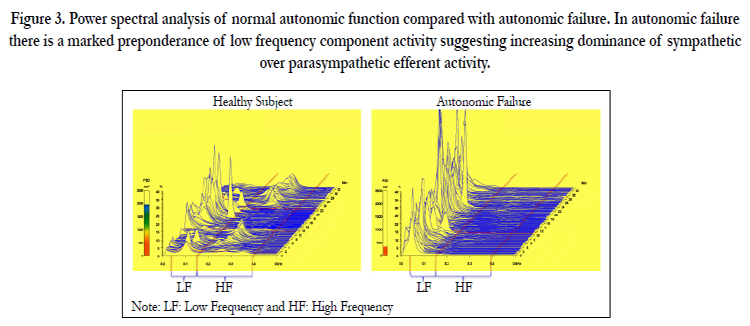
Figure 3. Power spectral analysis of normal autonomic function compared with autonomic failure. In autonomic failure there is a marked preponderance of low frequency component activity suggesting increasing dominance of sympathetic over parasympathetic efferent activity.
Cardiovascular Autonomic Neuropathy
Autonomic dysfunction is evident in CVD conditions, advancing unfavourable prognosis in a number of patient groups such as in patients with hypertension, ischaemic heart disease, previous myocardial infarction (MI) and heart failure, which is related to premature mortality.
The ANS plays an important role in both BP regulation and in the development of hypertension. Hypertension is a debilitating condition that increases the risk of cardiovascular morbidity and mortality and affects a large number of the world’s population. ANS dysfunction has been demonstrated previously in patients with systemic hypertension, where an increased sympathetic drive combined with decreased levels of parasympathetic modulation is witnessed [7]. Sympathetic hyper-activity has also been demonstrated in early hypertension [7], which suggests that neurohormonal dysregulation may be important in its aetiology, progression and consequent end-organ damage.
Research has demonstrated that a reduced HRV is present in patients with systemic hypertension. In normotensive patients a lower HRV was associated with greater risk of developing hypertension, which is consistent with the findings that dysautonomia is present in the early stage of hypertension [7]. Furthermore, hypertension has been noted to impair the cardiac baroreflex and cause vascular alterations. A reduced BRS is a marker of depressed vagal reflexes and associated with an increased risk of mortality.
Coronary artery disease (CAD) is a leading cause of global mortality and research has demonstrated that a reduced HRV is associated with the development of CAD [8] and predicts morbidity and mortality [9, 10]. Indeed, a recent angiographic study demonstrated an inverse relationship with HRV and the severity of CAD [11]. Furthermore, sympathetic drive and parasympathetic withdrawal reflected by changes in HRV has been demonstrated in ambulatory human subjects with ischaemic episodes [12]. Recently, Sharma and colleagues [13] demonstrated different HRV responses in the presence and absence of transient myocardial ischaemia in patients undergoing pharmacological (dobutamine) stress echocardiography with matched haemodynamic and myocardial workloads. In non-ischaemic patients, dobutamine stress was associated with a residual predominance of parasympathetic over sympathetic activity. In contrast, under ischaemic conditions, there was a reverse of this autonomic balance with greater residual sympathetic over parasympathetic activity, and this response was greater as the burden of ischaemia increased. The impact of this response on outcome is unknown and is the subject of ongoing research.
Autonomic dysfunction reflected by excessive cardiac sympathetic and/or inadequate cardiac parasympathetic modulation is a strong and independent predictor of mortality in patients following a MI. In HRV analysis, the sympathetic activation is reflected by an increase in the low frequency oscillations with an associated increased HR. An elevated HR during hospitalisation and discharge in patients with acute MI has been associated with an increase in both short and long-term mortality. However, the use of anti-ischaemic therapy (beta-blocker) to decrease HR was shown to reduce infarct size (by 25-30%), mortality and non-fatal re-infarctions [14].
The dysfunction of cardiac muscle nervous innervation due to tissue infarction, resulting in sympathetic predominance may arise due to the interruption of the fibres that pass across the affected tissue [15], which results in derangement in cardiac neural activity [1]. Necrosis of infarct cardiac tissue and the ensuing non-contracting segments may change the geometry of cardiac muscle contraction, which in turn may initiate an abnormal firing of sympathetic fibres due to mechanical deformation of the sensory endings [16]. The markedly increased sympathetic activation may debilitate the activity of parasympathetic innervation (vagal fibres) directed to the sinus node [1]. However, an alternative explanation is that the responsiveness of sinus node cells to neural modulations is reduced following a MI [1].
PSA of HRV in patients surviving a MI demonstrated a reduction in total and individual power of spectral components. When the power of sympathetic and parasympathetic frequencies were calculated in normalised units an increased low frequency component and diminished high frequency component was observed during resting conditions and over 24-hour electrocardiography recordings [17]. These results indicate sympathetic predominance. In addition, research reported a significant association between reduced HRV and increased rates of mortality, where patients with a low HRV had a 3.4-fold increase risk of death compared to patients with higher HRV [18]. Interestingly, female patients have worse prognosis post MI and research has indentified that women develop twice the sympathetic activation compared to men following an acute MI. This may be one of the mechanisms responsible for the known gender related differences in cardiovascular complications post MI [19].
BRS is a marker of the capability of the ANS to reflexively increase parasympathetic activity and simultaneously reduce sympathetic drive in response to a sudden increase in BP. When reduced, the BRS is significantly associated with an increased risk of death following a MI and when measured together, a reduced HRV and BRS further increases the risk of mortality in patients following a MI [20].
In a study of 808 post MI patients, HRV was an independent and better predictor of mortality than mean HR [18]. Although HRV is reduced following a MI, over a period of between 6 and 12-months HRV has been shown to improve in this population, but still remains lower than in healthy individuals [15]. These results suggest that markers of an imbalanced ANS may be useful for risk evaluation of post-MI patients [18], since the pathophysiological debilitation as a direct consequence of cardiac tissue infarction powerfully influences the activity of the ANS and therefore those patients who are at an increased risk of life threatening arrhythmias [21].
The pathophysiological link between a reduced HRV and increased mortality is unclear. In the Defibrillator in Acute Myocardial Infraction Trial (DINAMIT), patients who had a recent MI, reduced left ventricular ejection fraction and impaired autonomic function (as indicated by decreased HRV and high resting HR) did not have a survival benefit with prophylactic implantable cardioverter defibrillator intervention [22]. In addition, the Azimilide Post Infract Survival Evaluation study detailed that impaired HRV is associated with increased mortality but not specifically mortality from arrhythmic cause [23].
Chronic heart failure (CHF) is a common condition, which is difficult to manage in clinical practice with mortality rates exceeding 10% in patients with mild to moderate CHF, despite therapies that improve prognosis. Mortality rates of more than 40% are found in New York Heart Association (NYHA) functional classification IV patients [24].
Major abnormalities of autonomic cardiovascular control mechanisms are associated with CHF, with signs of sympathetic overactivation and parasympathetic withdrawal. This change in autonomic activity may play an important role in both predicting survival of CHF patients and the pathophysiology of cardiac death [24].
The dysautonomia associated with CHF, which is often interpreted as essential in order to maintain haemodynamic output contributes to disease progression and is associated with poor prognosis. However, assessment and quantification of autonomic dysfunction through analysis of HRV may provide additional important prognostic value for patients with CHF, since it has been shown to predict clinical outcome in such patient groups [24]. PSA of HRV may provide clinicians with valuable information regarding deterioration of disease and the intervention required to preserve and/or slow disease progression in order to maintain functional capacity. Such interventions include pharmacological and exercise training, which have both been shown to modulate the autonomic nervous system, by reducing sympathetic drive and increasing parasympathetic output [25].
Epidemiological research has demonstrated that resting HR is an independent predictor of cardiovascular and all cause mortality in men and women with and without diagnosed CVD [26]. Pathophysiological studies indicate that a high resting HR has a direct detrimental effect on progression of coronary atherosclerosis, myocardial ischaemia, ventricular arrhythmia and left ventricular function. Cardiac resynchronization therapy (CRT) with biventricular pacemakers has recently been shown to improve survival in a selected group of patients with NYHA functional class III or IV heart failure and cardiac dyssynchrony [27]. CRT has been demonstrated to increase HRV [28]. A study involving 113 patients with NYHA functional class III or IV heart failure found that those with improved time domain measures of HRV within 4 weeks of initiation of cardiac resynchronisation therapy had a better outcome compared to those with a less pronounced response [29].
Diabetic Autonomic Neuropathy
Diabetic autonomic neuropathy (DAN) is a common complication, which is positively related to an unfavourable outcome and carries an increased risk of morbidity and mortality. DAN increases with age (diabetes duration) and affects a considerable number of diabetic patients with large numbers presenting with symptoms. Furthermore, DAN is rarely recognised and poorly understood, which in part may be attributed to asymptomatic autonomic neuropathy and without examination may go undetected. These unsuspecting clinical features significantly impacts upon survival and quality of life in patients with diabetes as well as contributes to an increased cost of caring for the large numbers of adult diabetic patients in the UK.
DAN is a heterogeneous disorder, which affects different parts of the nervous system and therefore organ systems, such as the cardiovascular system, gastrointestinal tract and others and presents with diverse clinical symptoms. Cardiovascular autonomic neuropathy (CAN) is the most researched and clinically important form of DAN, which is frequently overlooked and has prevalence rates of between 7.7-90% in diabetic patients [30]. However, the heterogeneous methodology makes it difficult to compare CAN epidemiology across different research studies. CAN is a frequent degenerative complication in diabetes and confers to an increased cardiovascular risk. Indeed, diabetic patients with impaired autonomic function had approximately doubled the risk of mortality when compared to non-diabetic patients [31].
CAN results from damage to the autonomic nerve fibres that innervate the myocardium and vasculature, which causes abnormalities in HR control and central and peripheral blood vessel dynamics. The metabolic disorders of diabetes lead to diffuse and widespread damage of peripheral nerves and small vessels [30]. Damage to small myelinated and unmyelinated nerve fibres is manifested by impairment of vagally controlled HRV with diminished peripheral sympathetic tone that leads to increased blood flow together with reduced thermal and pain sensation, which gives rise to DAN. Small nerve fibre damage can occur selectively or together with impairment of other sensory modalities due to the loss of large nerve fibres. Indeed, the ubiquitous distribution of the ANS and the fact that the vagus nerve is the longest of the ANS (accounting for approximately 75% of all parasympathetic activity), typically renders almost all organs susceptible to dysautonomia and results in DAN to be a potential system wide disorder [30].
Parasympathetic nervous dysfunction causes an above normal resting HR, which is possibly attributed to vagal impairment that results in unopposed sympathetic nervous outflow, with resting HR reaching up to 130 b∙min-1. Parasympathetic nervous dysfunction occurs earlier than sympathetic nervous dysfunction in CAN, but advancement of disease with combined sympathetic and parasympathetic nervous impairment causes a slower HR. Advanced dysautonomia causes an apparent fixed HR, which means the determination of HR alone is not a reliable indication of CAN, whereas a reduction in HRV is the earliest indicator.
Research has demonstrated that diabetic patients diagnosed with dysautonomia via analysis of HRV, have increased mortality rates of 20-27% [32] compared to 4-5% in diabetic patients with no dysautonomia with the rates of sudden death higher in the former group [32]. Indeed, HRV analysis demonstrated a reduction of both parasympathetic and sympathetic activity in diabetic patients [33]. Furthermore, research demonstrated that diabetic patients showed distinct changes in HRV and BPV with reduced BRS, which decreased from minimal to severe according to disease status. The sensitive methods used to collect and analyse the data highlighted patients with no previous evidence of dysautonomia according to conventional testing and demonstrated altered HRV and BPV, which may represent the early stages of CAN [34]. Previous studies have demonstrated that sympathetic dominance is associated with a higher cardiovascular mortality in diabetic patients, which may be related to cases of sudden death [18], despite the absence of documented pre-existing heart disease [35].
Renal Autonomic Neuropathy
Renal autonomic neuropathy (RAN) is a complication that is related to a poor outcome. Patients presenting with chronic kidney disease (CKD) or end stage renal disease (ESRD) are characterised with extreme cardiovascular morbidity and mortality. Indeed, for patients aged between 15-30 years of age on haemodialysis, the incidence of cardiovascular death is 150 times greater than the general population [36].
Research has demonstrated that moderate-to-severe RAN is a prominent characteristic of renal dysfunction and can be present in up to 63% of patients with kidney disease. The autonomic dysfunction involves both the sympathetic and parasympathetic nervous system and research has reported a parallel reduction in BRS, which is important in the overall integrity of autonomic control [36]. However, symptoms of RAN are often vague and non-specific.
Patients with mild to moderate renal dysfunction or ESRD, display increased levels of sympathetic activity compared with healthy subjects, with further evidence describing that the diseased kidneys themselves may be a trigger of sympathetic hyperactivity. Signals arising from the kidney appear to mediate sympathetic over-activity that may be the result of circulating uraemia-related toxins, which are present in renal dysfunction and more pronounced in patients with ESRD regardless of effective dialysis treatment. The circulating toxins may produce sustained activation of sympathetic nervous activity through stimulation of renal afferent signals, which has been shown to be irreversible through long-term dialysis [37]. Furthermore, reports have detailed that lesions may occur in both the afferent and efferent limbs of the ANS in conditions of chronic uraemia [37], which may also contribute to renal dysautonomia.
A raised level of sympathetic nervous activity is now recognised as an important mechanism that contributes to an increased morbidity and mortality as well as the incidence of sudden cardiac death in RAN patients. Indeed, research has stated that high levels of circulating catecholamine’s adjunct with sympathetic nervous hyperactivity renders patients with renal dysfunction vulnerable to a series of severe cardiovascular complications, ranging from left ventricular hypertrophy, arterial remodelling, atherosclerosis and arrhythmias [38]. These adjoining diseases due to sympathetic over-activity culminates with a 92% excess risk of cardiovascular complications even in the absence of pre-diagnosed CVD [38].
The presence and severity of RAN does not appear to be associated with either the duration of renal dysfunction or dialysis treatment [37]. Therefore, the ability to use sensitive, non-invasive and reproducible equipment that has the ability to rapidly evaluate autonomic nervous control in patients with renal dysfunction is advantageous for early intervention and prevention of premature morbidity and mortality. Indeed research observed that in patients with end-stage renal disease (ESRD) successful renal transplantation corrected autonomic function [39].
Limitations
At present, non-invasive HRV analysis requires stationary, ectopic free, recording periods. Therefore, populations that may benefit from HRV assessment who have electrocardiographic disturbances, such as frequent ectopic beats or atrial fibrillation are excluded.
There is debate concerning the use of HRV frequency domains to represent sympathetic (low frequency) and parasympathetic (high frequency) cardiovascular modulation. Adhering to the traditional paradigm used to explain low frequency oscillations of HRV, it would be logical to assume that in disease states that are characterised by increased sympathetic drive, patients would exhibit marked increases in the low frequency component of cardiovascular variability. However, in patients with severe CHF, low frequency oscillations are reduced and in many patients absent. Indeed the greater the reduction in low frequency power the higher the level of sympathetic activation (measured invasively) and the greater the risk of mortality [40]. In addition, recent research has demonstrated that low frequency oscillations reflect BRS function and not cardiac sympathetic innervation [41]. Although further work is necessary in order to clarify and define the physiological importance of the low frequency distribution of HRV, overall power spectral density of HRV has continually provided clinically significant information, such as the association of increased mortality with reduced HRV in a number of disease states, including post MI, CHF, hypertension, diabetes, and renal disease compared to normal patients.
At present there is no clear consensus for normal power spectral density of HRV values for male and females as well as different ethic groups. Clarifying this may provide clinicians with information on disease progression and therefore a therapeutic target to improve HRV via interventions such as pharmacological optimisation and exercise training.
Conclusion
Traditional autonomic function testing still remains the foundation in the clinical evaluation of patients with suspected dysautonomia. However, autonomic data can also be derived non-invasively from beat to beat analysis of HR and BP. Computer based software (power spectral analysis) permits real time analysis of HRV in the frequency domain. Detection of autonomic dysfunction by this technique allows identification of high-risk patients who may benefit from earlier intervention. It may be suggested that patients who exhibit autonomic dysfunction are candidates for closer surveillance, which may include early coronary revascularisation and/or more aggressive pharmacological and/or device therapy to protect against premature mortality.
References
- Malik M, Bigger TJ, Camm JA, Kleiger RE, Malliani A et al. (1996) Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 93(5):1043-65.
- Frenneaux M (2004) Autonomic changes in patients with heart failure and in post-myocardial infarction patients. Heart 90(11):1248-55.
- Di Rienzo M, Castiglioni P, Ramirez AJ, Mancia G, Pedotti A (1992) Sequential Spectral Analysis of Blood Pressure and Heart Rate in Humans and Animals. In: Di Rienzo M, Mancia G, Parati G, Pedotti A, Zanchetti A. ed. Blood Pressure and Heart Rate Variability: IOS Press, 1992:24-38.
- Akselrod S, Gordon D, Ubel FA, Shannon DC, Berger AC, et al. (1981) Power spectrum analysis of heart rate fluctuation: a quantitative probe of beat-to-beat cardiovascular control. Science 213(4504):220-2.
- Parati G, Saul JP, Di Rienzo M, Mancia G (1995) Spectral analysis of blood pressure and heart rate variability in evaluating cardiovascular regulation. A critical appraisal. Hypertension 25(6):1276-86.
- Ewing DJ, Clarke BF (1982) Diagnosis and management of diabetic autonomic neuropathy. Br Med J 285(6346):916-8.
- Julius S (1991) Autonomic nervous system dysregulation in human hypertension. Am J Cardiol 67(10):3B-7B.
- Liao D, Cai J, Rosamond WD (1997) Cardiac autonomic function and incident coronary heart disease: a population-based case-cohort study. The ARIC Study. Atherosclerosis Risk in Communities Study. Am J Epidemiol 145(8):696-706.
- Hayano J, Sakakibara Y, Yamada M (1990) Decreased magnitude of heart rate spectral components in coronary artery disease. Its relation to angiographic severity. Circulation 81(4):1217-24.
- van Boven AJ, Jukema JW, Haaksma J, Zwinderman AH, Crijns HJ, et al. (1998) Depressed heart rate variability is associated with events in patients with stable coronary artery disease and preserved left ventricular function. REGRESS Study Group. Am Heart J 135(4):571-6.
- Kotecha D, New G, Flather MD, Eccleston D, Pepper J, et al. (2011) Fiveminute heart rate variability can predict obstructive angiographic coronary disease. Heart 98(5):395-401.
- Bernardi L, Lumina C, Ferrari MR (1988) Relationship between fluctuations in heart rate and asymptomatic nocturnal ischaemia. Int J Cardiol 20(1):39-51.
- Sharma R, O'Driscoll JM, Saha A, Sritharan M, Sutton R, et al. (2015) Differing autonomic responses to dobutamine stress in the presence and absence of myocardial ischaemia. J Physiol 593(9):2171-84.
- Kjekshus JK (1986) Importance of heart rate in determining beta-blocker efficacy in acute and long-term acute myocardial infarction intervention trials. Am J Cardiol 57(12):43F-49F.
- De La Cruz Torres B, Lopez Lopez C, Naranjo Orellana J (2008) Analysis Of Heart Rate Variability at Rest And During Aerobic Exercise. A Study In Healthy People And Cardiac Patients. Br J Sports Med 42(9):715-20.
- Malliani A (1982) Cardiovascular sympathetic afferent fibers. Reviews of Physiology, Biochemistry and Pharmacology 94:11-74.
- Lombardi F, Sandrone G, Mortara A (1992) Circadian variation of spectral indices of heart rate variability after myocardial infarction. Am Heart J 123(6):1521-9.
- Kleiger RE, Miller JP, Bigger JT, Moss AJ (1987) Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am J Cardiol 59(4):256-62.
- Hogarth AJ, Graham LN, Mary DA, Greenwood JP (2009) Gender differences in sympathetic neural activation following uncomplicated acute myocardial infarction. Eur Heart J 30(14):1764-70.
- La Rovere MT, Bigger JT, Marcus FI, Mortara A, Schwartz PJ (1998) Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) Investigators. Lancet 351(9101):478-84.
- Farrell TG, Bashir Y, Cripps T (1991) Risk stratification for arrhythmic events in postinfarction patients based on heart rate variability, ambulatory electrocardiographic variables and the signal-averaged electrocardiogram. J Am Coll Cardiol 18(3):687-97.
- Hohnloser SH, Kuck KH, Dorian P (2004) Prophylactic use of an implantable cardioverter-defibrillator after acute myocardial infarction. N Engl J Med 351(24):2481-8.
- Camm AJ, Pratt CM, Schwartz PJ (2004) Mortality in patients after a recent myocardial infarction: a randomized, placebo-controlled trial of azimilide using heart rate variability for risk stratification. Circulation 109(8):990-6.
- Nolan J, Batin PD, Andrews R (1998) Prospective study of heart rate variability and mortality in chronic heart failure: results of the United Kingdom heart failure evaluation and assessment of risk trial (UK-heart). Circulation 98(15):1510-6.
- Malfatto G, Branzi G, Riva B, Sala L, Leonetti G, et al. (2002) Recovery of cardiac autonomic responsiveness with low-intensity physical training in patients with chronic heart failure. Eur J Heart Fail 4(2):159-66.
- Gillum RF, Makuc DM, Feldman JJ (1991) Pulse rate, coronary heart disease, and death: the NHANES I Epidemiologic Follow-up Study. Am Heart J 121(1 Pt 1):172-7.
- Cleland JG, Daubert JC, Erdmann E (2005) The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med 352(15):1539-49.
- Adamson PB, Kleckner KJ, VanHout WL, Srinivasan S, Abraham WT (2003) Cardiac resynchronization therapy improves heart rate variability in patients with symptomatic heart failure. Circulation 108(3):266-9.
- Fantoni C, Raffa S, Regoli F (2005) Cardiac resynchronization therapy improves heart rate profile and heart rate variability of patients with moderate to severe heart failure. J Am Coll Cardiol 46(10):1875-82.
- Vinik AI, Maser RE, Mitchell BD, Freeman R (2003) Diabetic autonomic neuropathy. Diabetes Care 26(5):1553-79.
- Gerritsen J, Dekker JM, TenVoorde BJ (2001) Impaired autonomic function is associated with increased mortality, especially in subjects with diabetes, hypertension, or a history of cardiovascular disease: the Hoorn Study. Diabetes Care 24(10):1793-8.
- Ziegler D (1994) Diabetic cardiovascular autonomic neuropathy: prognosis, diagnosis and treatment. Diabetes Metab Rev 10(4):339-83.
- Bellavere F, Balzani I, De Masi G (1992) Power spectral analysis of heart-rate variations improves assessment of diabetic cardiac autonomic neuropathy. Diabetes 41(5):633-40.
- Ziegler D, Laude D, Akila F, Elghozi JL (2001) Time- and frequency-domain estimation of early diabetic cardiovascular autonomic neuropathy. Clin Auton Res 11(6):369-76.
- Tsuji H, Venditti FJ, Jr., Manders ES (1994) Reduced heart rate variability and mortality risk in an elderly cohort. The Framingham Heart Study. Circulation 90(2):878-83.
- Robinson TG, Carr SJ (2002) Cardiovascular autonomic dysfunction in uremia. Kidney Int 62(6):1921-32.
- Vita G, Bellinghieri G, Trusso A (1999) Uremic autonomic neuropathy studied by spectral analysis of heart rate. Kidney Int 56(1):232-7.
- Zoccali C, Mallamaci F, Parlongo S (2002) Plasma norepinephrine predicts survival and incident cardiovascular events in patients with end-stage renal disease. Circulation 105(11):1354-9.
- Rubinger D, Sapoznikov D, Pollak A, Popovtzer MM, Luria MH (1999) Heart rate variability during chronic hemodialysis and after renal transplantation: studies in patients without and with systemic amyloidosis. J Am Soc Nephrol 10(9):1972-81.
- van de Borne P, Montano N, Pagani M, Oren R, Somers VK (1997) Absence of low-frequency variability of sympathetic nerve activity in severe heart failure. Circulation 95(6):1449-54.
- Moak JP, Goldstein DS, Eldadah BA (2009) Supine low-frequency power of heart rate variability reflects baroreflex function, not cardiac sympathetic innervation. Cleve Clin J Med 76:S51-S59.





