Hypercalcemia And Metastic Parathyroid Carcinoma: Diagnostic Challenge
Mariano FV1*, Gondak RO2, Corrêa MB3, de Almeida OP4, Kowalski LP5
1* DDS, PhD of Department of Pathology, Faculty of Medicine, University of Campinas (UNICAMP), Brazil.
2 DDS, PhD of Department of Pathology, University of Santa Catarina (UFSC)
3 MD of Department of Head and Neck Surgery, Oncology Center, Piracicaba, Brazil
4 DDS, PhD of Department of Oral Diagnosis, Piracicaba Dental School, University of Campinas (UNICAMP), Brazil
5 MD of Department of Head and Neck Surgery, AC Camargo Cancer Center, São Paulo, Brazil
*Corresponding Author
Fernanda Viviane Mariano
DDS, PhD of Department of Pathology,
Faculty of Medicine, University of Campinas (UNICAMP),
Brazil.
E-mail: fmariano@fcm.unicamp.br
Received: November 12, 2013; Accepted: December 12, 2013; Published: December 19, 2013.
Citation: Mariano FV, et al. (2013) Hypercalcemia and Metastic Parathyroid Carcinoma: Diagnostic Challenge. Int J Clin Ther Diagn. 1(4), 23-26. doi: dx.doi.org/10.19070/2332-2926-130005
Copyright: Fernanda Viviane Mariano. © 2013 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Parathyroid carcinoma is an extremely rare neoplasm which typically is associated with hardened nodules in the parathyroid region, hypercalcemia and renal failure. A 69 year-old woman presented with knee pain at an emergency unity. On clinical examination the patient also presented a 2.0cm fibroelastic and mobile node in the left neck, level II. Serum total calcium and parathyroid hormone were increased, and the node was also detected by CT and 99mTc-sestamib scintigraphy. The patient had been surgically previously treated of parathyroid carcinoma misdiagnosed as a thyroid adenoma (eleven years ago), and a hyperplasia of parathyroid chief cells (nine years ago), that after revision was diagnosed as cervical metastasis of parathyroid carcinoma. She was surgically treated by neck dissection, confirming the second regional metastasis of parathyroid carcinoma. The diagnosis of parathyroid carcinoma is a challenge, and although rare, it should be considered in the presence of hypercalcemia and palpable neck nodule.
iv.Introduction
v.Description of The Case
vi.Discussion
vii.References
Keywords
Parathyroid Carcinoma; Hypercalcemia; Hyperparathyroidism; Lymph Node Metastasis; Nodule.
Introduction
Parathyroid carcinoma is an extremely rare neoplasm derived from parathyroid parenchymal cells, representingfewer than 4% of cases of parathyroid disease [1,2]. Primary hyperparathyroidism is mainly associated with adenomas (90%) and hyperplasias (7%) of the parathyroid, and less than 1% with carcinomas [3].
The main targets of PTH are the kidney and skeleton.Primary hyperparathyroidism is the most common cause of hypercalcemia, that when severe causes various symptoms, including fatigue, weakness, weight loss, anorexia, nausea, vomiting, renal insufficiency, nephrolithiasis, nephrocalcinosis, polyuria, and polydipsia, bone pain and pathologic fractures [4-6]. A palpable and hardened neck mass is a common finding in patients with parathyroid carcinoma, and it is reported in over 75% of cases1 [7,8].
Histologically it is very difficult to distinguish parathyroid carcinoma and adenoma, and parameters to be considered include fixation to the thyroid, metastasis, and vascular, perineural, capsular and adjacent tissues invasion. In parathyroid carcinomas hypercalcemia can reach very high levels3.
This report describes a patient who was initially surgically treated of a possible nodular hyperplasia of the parathyroid. Later she presented high hypercalcemia associated with lymph node metastasis of carcinoma of the parathyroid. The clinical diagnostic reasoning was fundamental to clarify this case.
Description of The Case
A 69 year-old Caucasian woman was referred in 2010 to the Emergency Service of the Fornecedores de Cana Hospital, Piracicaba, Brazil, complaining of pain in her knee. She had been previously submitted to left partial thyroidectomy in 1999 with histological diagnosis of thyroid adenoma. In 2008 the patient was submitted to cervical node biopsy with the diagnosis of hyperplasia of parathyroid chief cells.
During clinical and laboratory examinations, it was found that the patient presented high levels of hypercalcemia and a 2.0 cm fibroelastic, mobile nodule in the left cervical region. In addition, the patient also showed evident hoarseness. Based on these informations, laboratorial investigations were carried out, showing high levels of PTH and hypercalcemia (Table 1). A 99mTc-sestamib scintigraphy showed intense uptake in the cervical node, and CT scan confirmed that the palpable node highlighted by the scintigraphy was a cervical level II lymph node (Figs. 1 and 2).
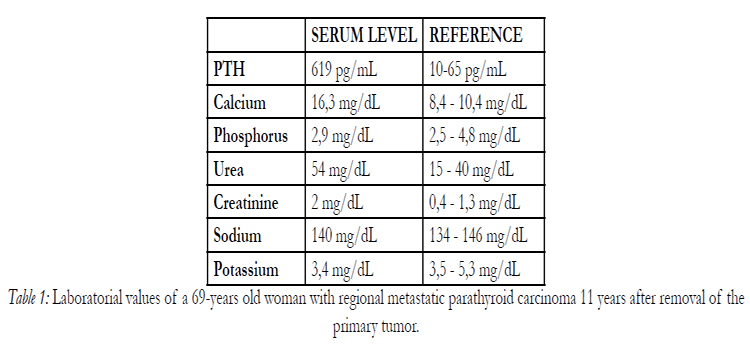

Table 1: Laboratorial values of a 69-years old woman with regional metastatic parathyroid carcinoma 11 years after removal of the primary tumor.
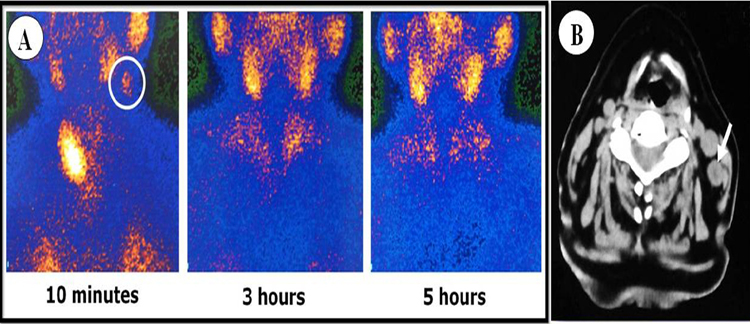
Figure 1: A- Parathyroid scintigraphy with 99mTc-sestamib. The circle at 10 minutes shows the uptake on the left cervical lymph node detected clinically. There are signs of left partial thyroidectomy at 10 minutes. At 3 and 5 hours it is seen only uptakes corresponding to normal structures.
B- Computed tomography of the neck. The image show in an axial section, without contrast, the cervical lymph node in level II confirmed histologically as metastasis of parathyroid carcinoma (arrow).
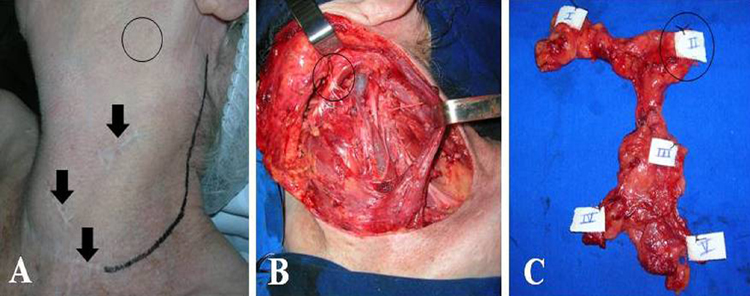
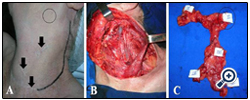
Figure 2: Radical left neck dissection of the second metastasis of the parathyroid carcinoma in lymph node.
A- Definition of surgical incision in black line. The arrows show the resulting scars due prior surgeries. The location of the palpable lymph node is indicated by circle.
B- Radical dissection of the neck showing the involved lymph node (circle).
C- Surgical specimen showing involved lymph node at level II.
Considering the present clinical data, a review of the original surgical specimen diagnosed as parathyroid hyperplasia in 2008 prompted the diagnosis of metastatic parathyroid carcinoma in cervical lymph node. It was then considered that the initial surgery of a left partial thryroidectomy realized in 1999 with the diagnosis of thyroid adenoma, was probably due a parathyroid carcinoma misdiagnosed as a thyroid adenoma. On this way, the patient had in 1999 a parathyroid carcinoma, in 2008 the first cervical lymphnode metastasis and in 2010, when we saw the patient,the second cervical metastasis.
The patient did not show evidences of distant metastasis or bone lesions, and she was then treated by radical left neck dissection (Fig. 3). One out of 38 nodes removed was involved by the carcinoma. Levels of calcium and PTH rapidly came close to normal, and symptoms improved.
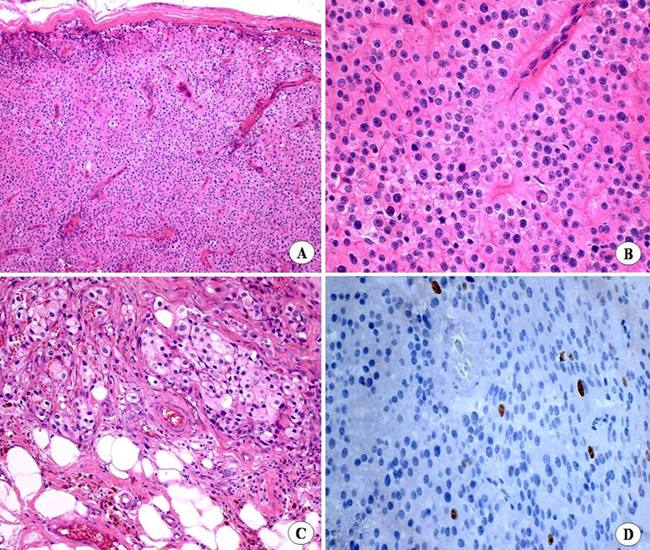
Figure 3: First metastasis of the parathyroid carcinoma in lymph node.
A- The nodule showed solid sheets of parathyroid malignant cells, with diffuse vascularization and broad fibrous septa surrounded by a thick capsule The cells were polyhedral, with well defined limits, and eosinophilic cytoplasm.
B- The nuclei were uniform, hyperchromatic and sometimes pleomorphic. Macronucleoli, and increased nuclear-cytoplasmic ratio and cytoplasmic inclusion also were observed.
C- The neoplasic cells invaded the adjacent adipose tissue and broad broad fibrous septa formed nests of vacuolated and granular pleomorphic cells.
D- Some cells were positive for Ki-67.
Eight months after surgery the patient showed slight increase in the PTH level, and a metastatic parathyroid tissue surrounded by fibrous connective tissue in the left side of the neck was surgically removed, followed by radiotherapy. The patient is under follow up for 10 months, without evidences of disease and with normal levels of calcium and PTH.
Histologically the review of the original surgical specimen from 2008 (first metastatic parathyroid carcinoma in cervical lymph node showed an encapsulated nodule, with areas of infiltration into the adjacent tissues. Most of the tumor was formed by solid sheets of polyhedral cells with well defined limits and eosinophilic cytoplasm, central nuclei and prominent nucleoli. The peripheral cells showed scant cytoplasm, with more hyperchromatic nuclei in relation to the central cells. An increased nuclear-cytoplasmic ratio and cytoplasmic inclusions also were found. Only a few cells showed positivity for Ki-67, indicating a low proliferative rate (Dako, clone MIB-1, dilution 1:100) (Figure. 4).
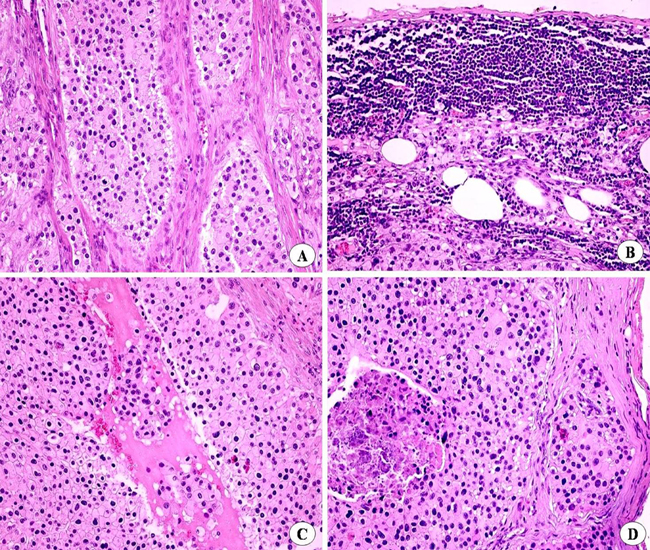
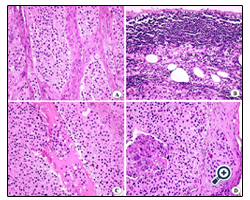
Figure 4: Second metastasis of the parathyroid carcinoma in lymph node.
A- The metastatic lymph node showed similar morphological and architectural features as shown on the first metastasis. Sheets of polyhedral eosinophilic cells separated by thick septae. Some cells showed nuclear pseudo-inclusions.
B- Residual lymphoid tissue was observed close of the lymph node capsule.
C- Areas of cystic degeneration.
D- Capsule invasion and comedonecrosis were also found.
The second metastatic lymph node detected in 2010, was invaded by the malignant parathyroid cells, showing similar morphological and architectural features as above described. Residual lymphoid tissue was found close to the lymph nodal capsule, which showed areas of invasion by the tumor cells. It was also observed areas of cystic degeneration and necrosis
Discussion
Hypercalcemia occurs in approximately 10-30% of all cancer patients, and it is the most common life-threatening metabolic disorder associated with malignancies. Chemical mediators as RANKL, TGF-β, PTHrP, IL-1,IL-6, IL-7 and TNF-α can be activated by factors released by tumor cells and cause hypercalcemia [9].
Hypercalcemia in patients with cancer can be either PTH-independent or dependent. PTH-independent includes humoral hypercalcemia of malignancy (HHM), local osteolytic hypercalcemia, hypercalcemia due to increased production of 1,25 dihydroxyvitamin D3, hypercalcemia related to drugs, and immobilization-associated hypercalcemia. PTH-dependent is associated with parathyroid carcinoma or ectopic production of PTH by malignancies [9].
The normal level of PTH (10-65pg/mL) is inversely proportional to the level of calcium in the blood, which is tightly regulated between 8.8 and 10.2 mg/dL. Our patient showed a serum level of PTH and calcium of 619pg/mL and 16.3 mg/dL respectively. High levels of hypercalcemia can be fatal, and determination of its causes is fundamental for the correct treatment. Rarely parathyroid carcinomas do not secrete PTH and consequently the patient does not show the signs and symptoms of hypercalcemia. On these situations the diagnosis of the tumor usually is late, and frequently the patients die due the large size of the tumor mass [10]. More frequently elevated levels of PTH can also be seen in non-neoplastic lesions of the parathyroid as hyperplasia, parathyroiditis and cysts, as well as in adenomas.
Hypercalcemia and its symptoms can be found in 86% of patients with parathyroid carcinoma, particularly bone and joint pain and renal stone [7,11,12].Our patient looked for treatment because of pain on her knees, but she also showed a neck nodule, that is found in more than 75% of the patients with parathyroid carcinoma [1,7,8,13]. Our patient also showed evident hoarseness and slight loss of voice, and it is well known that recurrent palsy of the laryngeal nerve in a patient with primary hyperparathyroidism is indicative of parathyroid carcinoma [3,13].
It should be considered that patients with primary hyperparathyroidism can present bone brown tumors, histologically similar to giant cell lesions of the jaws. Also patients with hereditary hyperparathyroidism with jaw-tumor syndrome (HPT-JT) present a fibrousosseous lesion indistinguishable of central ossifying fibroma, and up to 15% of these patients have parathyroid carcinoma [6,14,15]. Our patient was submitted to radiographic bone screening including the jaws, and no bone lesion was found.
The histological distinction between parathyroid adenoma and carcinoma is difficult. It is suggested that trabecular pattern, mitosis, Ki-67 index, nuclear hyperchromatism, thick fibrous bands, capsule and tissue invasiveness favors malignancies, but it should be also considered that some adenomas can show atypical morphology [6]. More reliable characteristics include metastasis, comedonecrosis and severe hypercalcemia. It is not uncommon that a parathyroid carcinoma is misdiagnosed as a benign lesion, as it happened initially on the present case.
Clinical and pathological staging is not yet well established for parathyroid carcinoma. Metastasis may occur in the later course of the disease, mainly in the lungs (40%), liver (10%) and also in regional lymph nodes (30%), as on the present case [7]. The clinical relevance of cervical node involvement is not well established [3]. Our patient showed two ipsilateral lymph node metastasis and one local recurrence, but a close follow up indicates that she is free of the disease and without clinical and laboratory alterations.
The main modality of treatment of parathyroid carcinoma is radical surgery, with removal of the lesion together with the ipsilateral thyroid, thyroid isthmus and lymph nodes. Surgery is also the treatment of choice for local recurrences and regional metastases [7]. Prior surgery, severe hypercalcemia should be controlled by drugs. Although the tumor is resistant to radiotherapy, it is indicated in cases of microscopic residual disease, and it was used on our patient, since she had two regional nodal metastases and one local recurrence involving fibrous tissue. The patient must have a long follow up, since metastases have been described later in the course of the disease, as happened on the case here described.
In short, the patient was treated 11 years before of an adenoma of the thyroid that probably was a non diagnosed parathyroid carcinoma. After 9 years a node on the neck was removed with the diagnosis of hyperplasia of the parathyroid, which on revision was in fact the first metastatic node of parathyroid carcinoma. After another 2 years she presented knee pain and high levels of hypercalcemia and a neck node that it was confirmed as the second metastatic parathyroid carcinoma. Finally after 8 months the patient presented a local recurrence, also surgically removed followed by adjuvant radiotherapy. Conclusively, clinical and histological diagnosis of parathyroid carcinomas can be a challenge, and severe hypercalcemia and its symptoms, associated with primary hyperparathyroidism and neck nodule are the main indicatives of this disease.
References
- Bondeson L, Grimelius L, DeLellis RA, Lloyd R, Akerstrom G.Parathyroid carcinoma. In: DeLellis RA, Lloyd RV, Heitz PU, Eng C. World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of endocrine organs. Lyon; 2004. pp. 124-127
- Carlson Diane. Parathyroid pathology. Hyperparathyroidism and parathyroid tumors. Arch Pathol Lab Med. 2010; 134:1639-1644.
- Owen, RP, Silver CE, Pellitteri, et al. Parathyroid carcinoma: A review.Head & Neck. Head Neck. 2011; 33:429-36.
- Shaha AR, Shah JP. Parathyroid carcinoma: a diagnostic and therapeutic challenge. Cancer.1999; 86:378-380.
- Shane E. Clinical review 122: parathyroid carcinoma. J Clin Endocrinol Metab. 2001;86:485-493.
- Givi B, Shah JP. Parathyroid carcinoma. Clinical Oncology.2010;22:498-507.
- Witteveen JE, Haak HR, Kievit J, Morreau H, Romijn JA, Hamdy NAT. Challenges and pitfalls in the management of parathyroid carcinoma:17-year follow-up of a case and review of the literature.Horm Canc. 2010; 1:205-214.
- Schantz A, Castleman B. Parathyroid carcinoma. A study of 70 cases.Cancer. 1973; 31:600-605.
- Santarpia L, Koch CA, Sarllis NJ. Hypercalcemia in câncer patients: pathobiology and management. Horm Metab Res. 2010; 42:153- 164.
- Wilkins BJ, Lewis JS. Non-functional parathyroid carcinoma: a review of the literature and report of a case requiring extensive surgery. Head Neck Pathol. 2009; 3:140-149.
- Valdivielso P, López-Sanchez J, Garrido A, Sánchez-Carrillo JJ. Metastatic calcificationa and severe hypercalcemia in a patient with parathyroid carcinoma. J Endocrinol Invest. 2006; 29:641-4.
- Kung B, Winokur R, Cognetti D, O’Hara B, Rosen D. Parathyroid carcinoma: a rare cause of primary hyperparathyroidism. Ear Nose Throat J. 2009; 88:E10-3.
- Busaidy NL, Jimenez C, Habra MA, et al. Parathyroid carcinoma: a 22-year experience. Head Neck. 2004; 26:716-726.
- Carpten JD, Robbins CM, Villablanca A, et al., HRPT2, encoding parafiromin, is mutated in hyperparathyroidism-jaw tumor syndrome.Nat Genet. 2002; 32:676-680.
- Chen JD, Morrison C, Zhang C, et al. Hyperparathyroidism-jaw tumour syndrome. J Intern Med. 2003; 253:634-642.





