Q Fever
Rehman HU1*, Kimberly Hagel2
1* Clinical Associate Professor, Department of Medicine, Regina Qu’Appelle Health Region, Regina General Hospital, Canada
2 Associate Professor, University of Saskatchewan, Saskatoon, Canada
*Corresponding Author
HU Rehman
Clinical Associate Professor, Department of Medicine,
Regina Qu’Appelle Health Region, Regina General Hospital,
Canada
E-mail: habib31@sasktel.net
Received: June 15, 2013; Accepted: June 27, 2013; Published: June 29, 2013
Citation: Rehman HU, Hagel K (2014) Q Fever Int J Clin Ther Diagn. 1(1), 1-4. doi: dx.doi.org/10.19070/2332-2926-130001
Copyright: Rehman HU© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
2.Q: What is your initial differential diagnosis?
3.Q: Zoonotic disease was raised as a possibility. Which zoonotic infection is most likely?
4.Q: What is the next step in management?
5.Outcome
6.Discussion
7.Clinical features
8.Treatment
9.Conclusion
10.References
Introduction
A 75-year-old retired farmer living in rural Saskatchewan, presented with fever, night sweats, and fatigue for three weeks and a two-day history of bilateral calf pain and lower extremity weakness in August. He reported occasional shortness of breath, but denied cough, altered bowel habit, chills, rash, arthralgia, or headache. He had no recent travel history or sick contacts, though he did have contact with animals including several miniature horses and a pet rabbit on his farm, and frequent attendance at horse shows. In the weeks prior to his presentation he had been working on the farm cleaning out an old barn. There was a positive remote history of multiple tick bites.
Past medical history included hypertension, benign prostatic hypertrophy, rheumatoid arthritis, chronic obstructive pulmonary disease, atrial fibrillation, diverticulosis, and granulomatosis with polyangiitis, which had been symptomatic in the past with scleritis and upper airway inflammation but had been quiescent recently. Patient was taking methotrexate 10mg/week. At his home hospital the patient’s white blood cell count was 17.9×109/L (4.1-10.0) and temperature was 37.2°C, reaching a high of over 38°C. Urine and blood cultures were negative. He was treated empirically with gentamicin 540mg IV q24h and ceftriaxone 2gm q12h.
Despite this antibiotic regimen, the patient’s condition did not improve and his temperature continued to spike. After three days in hospital, the patient developed pitting edema to the distal legs bilaterally and weakness to the distal arms and neck. The patient was transferred to our center for further assessment. On evaluation at our hospital, he appeared non-toxic. Vital signs were within normal limits. There was a grade two systolic murmur at the right upper sternal border and marked pitting edema to the legs bilaterally. No lymphadenopathy or rash was present; respiratory and abdominal examinations were unremarkable. Neurologic examinations revealed generalized weakness and diffuse hyporeflexia. Laboratory results are outlined in Table 1.
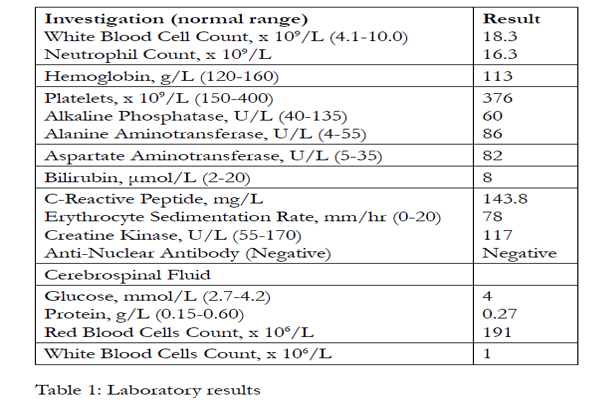

Table 1: Laboratory results.
No significant intrathoracic abnormalities were found on chest X-Ray. Computerized tomographic (CT) scan of the chest and abdomen did not reveal any lymphadenopathy or collection of pus. Few indeterminate pulmonary nodules were seen. Nuclear medicine white blood cell whole body-scan showed no abnormal uptake and no evidence of occult infection. Nerve conduction studies were normal. MRI of the cervical spine showed degenerative disc changes and bilateral moderate to severe neural foraminal stenosis at C5-6 and C6-7. There was no evidence of discitis or osteomyelitis. Antinuclear antibody test was negative and rheumatoid factor was elevated at 1160 IU/mL. Anti-myeloperoxidase ((MPO) antibody was positive at 47U/ml (0-6). Anti-neutrophil cytoplasmic antibody (ANCA) serology had been negative 3 years ago. He was seen by the rheumatology consult service who, did not think that granulomatosis with polyangiitis was active. Methotrexate was discontinued.
Q: What is your initial differential diagnosis?
a: Lymphoma
b: Subacute infective endocarditis
c: Tuberculosis
d: Zoonotic infection
Prolonged fever, night sweats, generalized weakness and fatigue are common symptoms of lymphoma, particularly in this age group and was one of the differential diagnosis in our patient. However, absence of lymphadenopathy, splenomegaly on clinical and radiological examination did not show mediastinal or retroperitoneal lymphadenopathy. Bone marrow aspirate revealed a normoblastic erythroid series and myeloid hyperplasia. Megakaryocyte, plasma cell, and lymphocytic populations were normal. Marrow biopsy showed normocellular normoblastic bone marrow. Myeloid series and megakaryocytes appeared normal, and there was no evidence of granuloma or lymphoma. Reticulin stain showed minimal reticulin fibrosis. These findings make lymphoma very unlikely.
Culture negative infective endocarditis was also on the list of differential diagnoses at this stage. Transesophageal echocardiography (TEE) showed bilateral atrial enlargement and aortic sclerosis but failed to reveal any vegetations. Negative blood cultures and absence of vegetation on TEE makes endocarditis less likely.
Although clinical picture of prolonged fevers and night sweats would suggest tuberculosis, absence of cough and negative findings on radiology and bone marrow biopsy make pulmonary or disseminated tuberculosis unlikely. Disseminated tuberculosis however, is often difficult to diagnose, and neither the PPD test nor stains for acid-fast bacilli are sensitive enough to rule out disseminated tuberculosis. Patient had no known exposure to tuberculosis and was not taking tumor necrosis factor-alpha (TNF-a) antagonist drugs, which would have predisposed him to tuberculosis.
Gentamicin and ceftriaxone were administered in the peripheral hospital presumably as empiric therapy for an occult infection. Lack of response to broad- spectrum antibiotic treatment and negative blood cultures should make one aware of the possibility of either a non-infectious cause of fever or an infectious agent that is difficult to culture in the laboratory.
Q: Zoonotic disease was raised as a possibility. Which zoonotic infection is most likely?
a-Histoplasmosis
b-Tularemia
c-Brucellosis
d-Q fever
The differential diagnosis at this stage was narrowed to: disseminated histoplasmosis, brucellosis, tularemia and Q fever. Histoplasma capsulatum is a thermally dimorphic fungus found in soil, where the organism exists in mycelial phase. Cattle-farming is a risk factor for histoplasmosis. Infection is acquired by inhaling the spores, which are deposited in the lungs. Histoplasmosis is usually asymptomatic and self-limiting in the normal host. However, progressive disease, either restricted to lungs or disseminated, develops in a small number of patients, particularly in patients with immunodeficiency [1]. Fever and weight loss are common symptoms. Pulmonary infiltrates are found in about half the patients. Bone marrow involvement can cause cytopenias. Being on immunosuppressant treatment, our patient was susceptible to disseminated histoplasmosis and could have been exposed to histoplasmosis on his farm. However, bone marrow cultures were negative for H. capsulatum andmycobacterial tuberculum. Bone marrow cultures are positive for H. capsulatum in over 90% of patients. Urinary polysaccharide antigen test, which is highly sensitive and specific for H. capsulatum was negative, thus excluding the diagnosis.
With patient’s history of exposure to farm animals and tick bites and sub acute illness with fever, headache, generalized arthralgias, weakness and liver function abnormalities, infection with Francisella tularensis must be considered. F.tularensis can persist for months in mud, water and mammal or bird carcasses and can be spread to humans by ingestion, inhalation, tick and deerfly bites, contact with infected tissues, or an animal bite. Depending on the route of infection, a number of syndromes including ulceroglandular, oculoglandular, oropharyngeal, and pneumonic tularemia are recognized [2]. In the ulceroglandular variety, the cutaneous lesion begins as a papule, which ulcerates with raised edges and forms an eschar and is usually associated with regional lymphadenopathy. Involved lymph nodes may suppurate and drain but there is no associated lymphangitis. Fever, chills, malaise, myalgia, arthralgia, sore throat and fatigue are common symptoms. Oculoglandular tularemia is characterized by painful, purulent unilateral conjunctivitis with cervical and periauricular lymphadenopathy. Ingestion of infected food or water may cause oropharyngeal or gastrointestinal tularemia. Oropharyngeal tularemia is characterized by acute exudative pharyngitis, tonsillitis or stomatitis with cervical lymphadenopathy. Tonsils enlarge and may be covered by a yellow or white pseudomembrane. Abdominal pain, nausea, vomiting diarrhea, gastrointestinal bleeding and mesenteric lymphadenopathy characterize gastrointestinal tularemia.
Typhoidal tularemia has symptoms of fever, chills, dry cough, myalgia, arthralgia and sore throat without any focal signs. Inhalation of the aerosolized organisms causes pneumonic tularemia. Symptoms include fever, non-productive cough, pleuritic chest pain and dyspnea. Chest X-ray will show pulmonary infiltrates which may be bilateral and associated with hilar adenopathy. In our patient lack of ocular involvement and painful regional lymphadenopathy makes the oculoglandular and ulceroglandular varieties of tularemia unlikely. Lack of abdominal symptoms, cough, and pulmonary infiltrates on radiological examination make typhoidal and pneumonic varieties unlikely. Tularemia serology was negative.
Brucellosis can be acquired by drinking unpasteurized dairy products on a farm. Humans acquire brucellosis from exposure to infected animals or contaminated animal products and would be a consideration in the differential diagnosis of our patients because of history of exposure to farm animals. Although, Canada was declared free of brucellosis in 1985, several isolated cases of bovine brucellosis in livestock were subsequently identified, with the last known case occurring in a cattle herd in Saskatchewan in 1989 [3]. The incubation period for brucella infection is highly variable, ranging from a few days to many months. Brucellosis, therefore, should be considered a possibility when detailed travel history is not available. Moreover, brucellosis may be acquired from ingestion of imported dairy products such as cheese.
Patients with acute brucellosis present with nonspecific symptoms, including fever, sweats, malaise, and anorexia. Chronic brucellosis may cause ulcerations of the gastrointestinal tract, splenic abscess or splenomegaly, and osteoarticular complications, including osteomyelitis, arthritis, tenosynovitis, bursitis, and spondylitis. Sacroiliitis is the most frequently reported articular complication of brucellosis . Blood cultures are often negative in brucellosis often yield no organisms, and the diagnosis rests principally on serologic test results. Our patient had no recent travel history to brucella endemic areas. Lack of articular symptoms and negative serological tests for brucellosis makes it an unlikely diagnosis in our patient.
Q fever was thought likely at this stage since lymphoma; infective endocarditis, brucellosis, tularemia, histoplasmosis and tuberculosis were excluded. Q-fever can cause prolonged fever, abnormal liver enzymes and is associated with exposure to farm animals. Coxiella burnetti serology was positive as outlined in Table 2,confirming a diagnosis of acute Q fever, likely causing granulomatous hepatitis. Q fever can present as an acute or chronic infection.
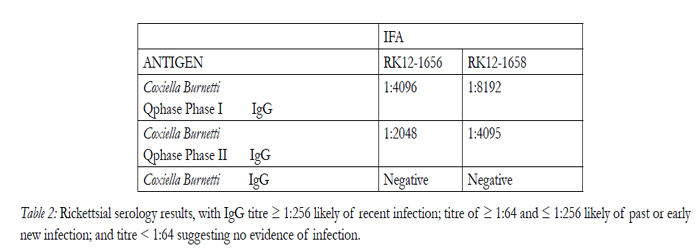
Table 2: Rickettsial serology results, with IgG titre ≥ 1:256 likely of recent infection; titre of ≥ 1:64 and ≤ 1:256 likely of past or early new infection; and titre < 1:64 suggesting no evidence of infection.
Q: What is the next step in management?
a- Liver Biopsy
b- Inform Public Health
c- Change treatment to doxycycline and chloroquine
Q-fever causes granulomatous infection of the liver and abnormal liver enzymes are a common finding in Q fever. A diagnosis of granulomatous hepatitis due to acute Q- fever is highly likely in view of abnormal liver enzymes and positive serology for C burnetti, a liver biopsy may show characteristic fibrin-ring granulomas. However, liver biopsy is an invasive procedure with risk of complications and will not change management decisions, is not indicated.
Q fever is a reportable disease in Ontario under the Health Protection and Promotion Act and must be reported immediately to the local medical officer of health by telephone. The disease should be reported even if it is only suspected and has not yet been confirmed [5]. It is not notifiable in Saskatchewan.
Treatment for acute Q fever is doxycycline 100mg twice daily for 2 weeks. Patient’s serology and course of illness at this stage suggests acute Q fever. Addition of hydroxychloroquine therefore is not indicated. Treatment for chronic Q-fever is combination of doxycycline and chloroquine for at least 1.5 to 3 years. Hydroxychloroquine is added to increase lysosomal pH to enhance activity of Doxycycline in the intracellular compartment where Coxiella resides. Hydroxychloroquine therefore, should be added to the treatment regimen if future course of the disease suggests chronicity.
Outcome
Patient was initially treated with doxycycline 100mg twice daily for acute Q fever. Patient complained of recurrent fevers when reviewed 4 weeks later. He also felt generalized weakness and fatigue. Liver enzymes showed a worsening trend. Chronic Q fever was thought likely at this stage. Doxycycline was restarted and chloroquine was added to his treatment. Patient was doing well 4 months after initial presentation. He had no fevers, muscle pains and fatigue had improved significantly and liver enzymes came down to within normal range.
Discussion
Q-fever is a zoonosis caused by Coxiella burnetii, an obligate intracellular pleomorphic gram-negative coccobacillus. The reservoir includes a wide variety of animals including cows, goats, sheep, dogs, cats, wild rodents and small mammals, big game wild life, reptiles, amphibians, birds, fish and ticks [6]. C burnetii is shed in milk, faeces, urine, and especially in birth byproducts. Humans are infected by inhalation of infectious aerosol particles from parturient fluids of infected livestock. One does not need direct exposure to the animals since Coxiella burnetii can be carried in dust and wind over large distances. Sporadic cases of human transmission have occurred by consuming unpasteurised milk, contact with contaminated clothing, blood transfusion, sexual intercourse, and tick bites. Transplacental transmission may cause congenital infection.
Q-fever has been reported from most countries except New Zealand [7]. Incidence varies in different geographic areas, being 500 cases per million people in France, 38 cases per million persons in Australia and 0.28 cases per million persons in USA [8]. The number of cases of Q fever has declined considerably from the 1980s and early 1990s. Q fever was common in Nova Scotia (50-60 cases per year in a population of 950, 000) . Since 2004, only 4-5 cases have been reported each year [10].
Clinical features
Asymptomatic infections are common. After an incubation period of 9-28 days, the acute illness presents with an influenza-like illness with headache, fever, myalgia and atypical pneumonia. However, late presentations can occur. Chest radiographs findings are nonspecific and pneumonia is mild with non-productive cough with minimal auscultatory findings. Maculopapular or purpuric rash occurs in 10% and myocarditis and meningoencephalitis in 1% of cases.
Endocarditis accounts for 60 to 70% of chronic Qfever. Diagnosis is difficult since cultures are usually negative and vegetations absent or small. Most patients with endocarditis have underlying valvulopathies or immunosuppression. Modified Duke criteria for endocarditis takes this into account and serologic evidence of active infection with Coxiella burnetii has been included as a major criterion [11]. After an incubation period of 1 to 20 years it usually presents with fever, malaise, weight loss, chills, anorexia and night sweats. Other manifestations of chronic Q-fever include osteomyelitis, granulomatous hepatitis, infected aortic aneurysms and chronic pulmonary infections. Q fever infection in pregnancy may induce abortion or premature delivery and cause intrauterine growth retardation, intrauterine foetal death, and oligoamnios [12].
Leucocyte count is generally normal but may be elevated. Thrombocytopenia is found in 25% of patients. Transaminases are moderately elevated in 85% of patients. Hyperglobulinemia and elevated erythrocyte sedimentation rate are common findings. Rheumatoid factor and autoantibodies including antimitochondrial antibodies, anti-smooth muscle antibodies and antibodies to phospholipids are commonly found in chronic Q fever [13]. Fibrin ring or “doughnut” granulomas may be found in liver or bone marrow biopsy specimen.
Treatment
Our patient was discharged on doxycycline 100 mg twice daily and hydoxychloroquine 200mg three times daily with follow-up arranges as out patient. The treatment of choice for acute Q-fever is oral doxycycline 100mg every 12 hours for 12 to 14 days. Cotrimoxazole is recommended for pregnant women and young children. Pregnant patient treated with cotrimoxazole may require treatment with doxycycline and hydroxychloroquine for chronic Q-fever post-partum. Two different treatment protocols have been evaluated: doxycycline in combination with quinolones for at least 4 years and doxycycline in combination with hydroxychloroquine for 1.5 to 3 years. The second therapy leads to fewer relapses, but requires routine eye exams to detect accumulation of chloroquine. The efficacy of doxycycline/ hydroxychloroquine combination treatment has been confirmed in a study comparing with the standard treatment of doxycycline (100mg) twice daily and ofloxacin (200mg) 3 times daily16. This treatment should be continued for 18 months to 3 years. However, the optimum duration of treatment is unknown.
The ratio of serum doxycycline concentration to MIC should be monitored during the course of therapy in patients with Q-fever endocarditis and should be maintained ≥1 since patients with a ratio between 0.5 and 1 show a low decline of antibody levels compared to those with a ratio of ≥117. In practice, however, obtaining MIC values and doxycycline levels are difficult and not available in most laboratories.
IgM and IgG antibody titres to phase-I should be monitored every 3 months during therapy until they are less than 1:200. IgM antibodies disappear first, followed by IgA antibodies. IgG titres may remain posiHU Rehman, International Journal of Clinical Therapeutics and Diagnosis 2013, 1:102 6 tive for years. Relapse rate is high even with combination therapy and antibody titres should be monitored once the treatment is discontinued. A 4-fold rise indicates relapse. Follow up for life may be needed.
Farmers, ranchers and farm workers in contact with cattle, sheep and goats; meat packers, rendering plant workers, hide and wool handlers; hunters and trappers; laboratory animal researchers and support staff; and workers who care for pets and livestock, veterinary personnel, pet-shop workers and zoo attendants are occupations at risk of Q fever and should take precautions when handling animals or animal products. The risk can be reduced in high- risk workers by vaccination of workers, personal precautions, and workplace hygiene. The use of this vaccine should be limited to those at high risk of exposure whose blood tests for resistance to Q fever are negative. Before vaccination, workers must also have a skin test to determine if they are allergic to the vaccine [15].
Conclusion
Q-fever should be sought as a diagnostic possibility when a patient presents with fever of unknown origin, has a relevant history of exposure to animals and when the blood cultures and other radiological conditions do not find an alternative cause of patient’s symptoms.
References
- Christopher-Stine L., Robinson D.R., Wu C.C., Mark E.J. Case 37-2012 — A 21-Year- Old Man with Fevers, Arthralgias, and Pulmonary Infiltrates. N Engl J Med 2012; 367:2134-2146.
- Rehman HU. Separating the chaff from the grain. Eur Rev Med Pharmacol Sci 2011; 16(4): 554-8.
- http://www.inspection.gc.ca/animals/terrestrial-Animals/diseases/ reportable/brucellosis/fact-sheet/ Accessed April 14, 2013
- Noble JT, Mark EJ. Case 10-2013 — A 30-Year-Old Man with Fever,Myalgias, Arthritis, and Rash. N Eng J Med 2002;347:200-6.
- http://www.health.gov.on.ca/english/providers/pub/disease/qfever.html. Accessed April 13, 2013.
- Parker NR, Barralet JH, Bell AM. Q fever. Lancet 2006;367:679-88.
- Hilbink F, Penrose M, Kocacova E, Kazar J. Q fever is absent from New Zealand.Int J Epidemiol 1993;22:945-9.
- McQuiston JH, Holman RC, McCall CL, Childs JE, et al. National surveillance and epidemiology of human Q fever in the UnitedStates, 1978-2004. Am J Trop Med Gyg 2006;75:36-40.
- Marrie TJ, Durant H, Williams JC, Mintz E, Waag DM Exposure to parturient cats: a risk factor for acquisition of Q fever in Maritime Canada. J Infect Dis 1988;158:101- 8.
- Marrie TJ. Campbell N. McNeil SA. Webster D. Hatchette TF. Q fever update, Maritime Canada.Emerging Infectious Diseases 2008;14:67-9.
- Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infec Dis 2000;30:633-8.
- Raoult D, Fenollar F, Stein A. Q fever during pregnancy: Diagnosis, treatment and follow-up. Arch Intern Med 2002;162:701-4.
- Maurin M, Raoult D. Q fever. Clin Microbiol Rev 1999;12:518-53.
- Fournier PE, Marrie TJ, Raoult D. Diagnosis of Q fever. J Clin Microbiol 1998;36:1823-34.
- http://www.ccohs.ca/oshanswers/diseases/qfever.html. Accessed April 13, 2013.





