Increased Maternal Serum Placental Growth Hormone Variant in Pregnancies Complicated with Otosclerosis
Liao S1,2, Li G3, Chen R3*
1 Rural Clinical School, University of New South Wales, Sydney, New South Wales, Australia.
2 The First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, China.
3 Department of ENT, The First Hospital of Wenzhou Medical University, Wenzhou, China.
*Corresponding Author
Dr Ruiying Chen MD, PhD,
Department of ENT, The First Hospital of Wenzhou Medical University,
Wenzhou, Zhejiang, 325035, China.
E-mail: chen.ruiying888@gmail.com
Received:June 27, 2018; Accepted: September 24, 2018; Published: September 29, 2018
Citation: Liao S, Li G, Chen R. Increased Maternal Serum Placental Growth Hormone Variant in Pregnancies Complicated with Otosclerosis. Int J Clin Trails Case Stud. 2018;3(1):16-19.
Copyright: Chen R© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: To investigate the possible role of maternal serum concentrations of placental growth hormone variant (GHV), insulin-like growth factor (IGF) 1 and 2, and IGF binding proteins (IGFBP) 1 and 3 in pregnancies complicated by otosclerosis.Method: Otosclerosis cases (n = 22) and age, ethnicity-matched controls (n = 22) were selected in a nested case-control study. Maternal serum hormone concentrations at 26 and 34 weeks of gestation were determined by enzyme-linked immunosorbent assay (ELISA).
Results: Maternal serum GH-V concentrations at 26 and 34 weeks of gestation were significantly increased in the otosclerosis group, when compared to the control group (2.53 ± 0.17 ng/ml vs. 1.78 ± 0.19 ng/ml, p = 0.036; 4.34 ± 0.31 ng/ml vs. 3.12 ± 0.18 ng/ml, p < 0.001, respectively). Maternal serum IGF-1 concentrations at 34 weeks in otosclerosis pregnancies were significantly higher than in the controls (589.1 ± 21.4 ng/ml vs. 499.7 ± 17.8 ng/ml, p < 0.001). The increase of IGF-1 was not observed at 26 weeks of gestation. There were no significant differences in serum IGF-2 or IGFBP-1 or IGFBP-3 concentrations between groups.
Conclusion: Concentrations of GH-V and IGF-1 in maternal serum were altered in pregnancy complicated with otosclerosis, suggesting that the GH-IGF axis may contribute to the development of this condition during pregnancy.
2.Abbreviations
3.Introduction
4.Materials and Methods
4.1 Participant
4.2 GH-V ELISA Procedure
4.3 Serum Analysis
4.4 Statistical Analysis
4.Results
5.Discussion
6.Conclusion
7.Acknowledgments
8.References
Keywords
Placental Growth Hormone; Pregnancy; Otosclerosis.
Abbreviations
GH-V: Growth Hormone Variant; PGH: Placental Growth Hormone; IGF: Insulin-like Growth Factor; IGFBP: Insulin-like Growth Factor Binding Proteins; ELISA: Enzyme-Linked Immunosorbent Assay; TMB: Tetramethylbenzidine; MMR: Measles, Mumps, and Rubella.
Introduction
Otosclerosis is a common form of progressive hearing loss in adults, which characterized by alternating phases of bone resorption and formation [1]. The activity of osteoblasts and osteoclasts plays an important role in the disease process [2]. Its aetiology remains poorly understood with a number of possible factors implicated in its development, including genetics, autoimmunity, viruses, inflammation, and hormones [3]. Hormone factors, especially estrogen, have long been considered to involve in the pathogenesis of otosclerosis due to the observations that increased occurrence or aggravation of the hearing loss in women during or shortly after pregnancy [4, 5]. However, a retrospective study by Lippy et al., on 128 women does not support this belief [6]. Moreover, despite the well-established participation of estrogen in osteoblastic function [7], hormonal influence of oral contraceptives does not predispose the female population to an increase in otosclerosis [8]. Therefore, based on the current evidence, the definitive conclusions, in terms of the association of otosclerosis and pregnancy, cannot be drawn.
Pregnancy involves endocrine and metabolic changes as a consequence of physiological alterations between mother and fetus, leading to the vast changes in maternal hormones during gestation. Placental growth hormone variant (GH-V) is a hormone specifically expressed in the syncytiotrophoblast layer of the human placenta [9]. GH-V gradually replaces GH-N as the main form of circulating GH at approximately 20 weeks gestation and is therefore thought to play a key role in maternal adaptation to pregnancy [10, 11]. GH-V differs from pituitary growth hormone (GH-N) by only 13 amino acids and shares similar physiological effects with GH-N, including the stimulation of insulin-like growth factor (IGF)-1 [12, 13]. Providing the evidence that GH regulates osteoblasts and osteoclasts activity and plays an important role in the maintenance of bone mass and the process of bone remodelling [14, 15], we hypothesised that GH-V was associated with the development of otosclerosis during pregnancy. The aim of this study was to determine whether maternal serum concentrations of GH-V, IGF-1 and 2, IGF binding proteins (IGFBP)-1 and 3 were altered in pregnancy complicated with otosclerosis.
This retrospective study was conducted in The First Hospital of Wenzhou Medical University according to the principles of the Declaration of Helsinki. Ethical approval was obtained from the institutional ethics committee of Wenzhou University on human research, and all women provided written informed consent. Between June 2013 and May 2017, 1286 nulliparous women from Wenzhou city (Zhejiang Province, China) with singleton pregnancies were recruited. Participants were given routine antenatal care. Detailed clinical and demographic data were collected. Maternal serum samples were collected at 26 and 34 weeks and stored at -80 °C. The specimens did not undergo any freeze/thaw cycles prior to analysis. 22 participants firstly diagnosed with otosclerosis during pregnancy were selected in our study. Diagnosis of otosclerosis was based on symptoms of progressive hearing loss, vertigo and tinnitus, audiometric examination with low-frequency conductive hearing loss, and the exclusion of other audiologic pathologies. Participants then underwent surgery after delivery, and the definite diagnosis was made by postoperative histopathologic analysis [16]. Exclusion criteria includes previous hearing impairment, gestational diabetes, preeclampsia, renal/liver failure, cardiovascular disorders, bleeding disorders, bone disorders, autoimmune disorders, congenital defects and abnormal fetal growth. In this nested case-control study, 22 otosclerosis cases were matched by ethnicity and age (± 3 years) to 22 controls.
The serum concentrations of GH-V were determined by an inhouse enzyme-linked immunosorbent assay (ELISA) [17]. In brief, microtiter plates were coated with the human GH-V monoclonal antibody 78.8E8 (Bio-Rad AbD Serotec) diluted in phosphate buffer (0.1M Sodium Carbonate, pH 9.5) at a concentration of 2 μg/ml by overnight incubation at 4°C and then blocked by Ultrablock (Bio-Rad AbD Serotec) at room temperature for 1 hour. Recombinant human 22-kDa GH-V protein (Protein Laboratories Rehovot) was reconstituted in 0.4 % NaHCO3 pH 9 as previously described [18]. GH-V standards were prepared with a range from 0.078 to 5 ng/ml. Standards and 1:2 diluted serum samples were incubated for 2 hours at room temperature, then washed for three times. All serum samples were measured in duplicate. The human GH-V monoclonal antibody 78.7C12 (Bio-Rad AbD Serotec) was biotinylated using a LYNX Rapid Biotin Antibody Conjugation Kit (Bio-Rad AbD Serotec). 8 μg/ ml biotinylated antibody 78.7C12 was added and incubated for 1 hour. After being washed three times, 200 ng/ml horseradish peroxidase conjugated streptavidin (Bio-Rad AbD Serotec) was added and incubated for 30 minutes. The microtiter plates were washed four times. 3, 3′, 5, 5′-Tetramethylbenzidine (TMB) Substrate Reagent Set (BD Biosciences) and stop solution (2N H2SO4) were used for end-point detection. Absorbance was read at 450 nm and 590 nm within 30 minutes of stopping reaction. Serum samples were spiked with recombinant GH-V and the average recovery rate was 106%. Coefficients of variation of intra-assay and inter-assay were 4.8% and 6.8%, respectively.
Serum concentrations of total IGF-1, total IGF-2, IGFBP-1 and IGFBP-3 were assayed with human-specific ELISAs as per the manufacturer’s instructions (Mediagnost).
Data are expressed as means ± S.E.M unless stated otherwise. Group means were compared using a Student’s t test. Categorical variables were compared using chi-square or Fisher’s exact test. All analyses were conducted using IBM SPSS Statistics 23. A p-value of < 0.05 was accepted as statistically significant.
Results
The demographic and clinical details are shown in Table 1. There were no significant differences in family history of hearing loss, the measles, mumps and rubella (MMR) vaccination status, smoking and drinking habit, and previous oral contraceptives use between the otosclerosis group and the control group (Table 1). The average gestational age when diagnosed with otosclerosis is 25.9 ± 2.9 weeks (range from 21 to 32 weeks).
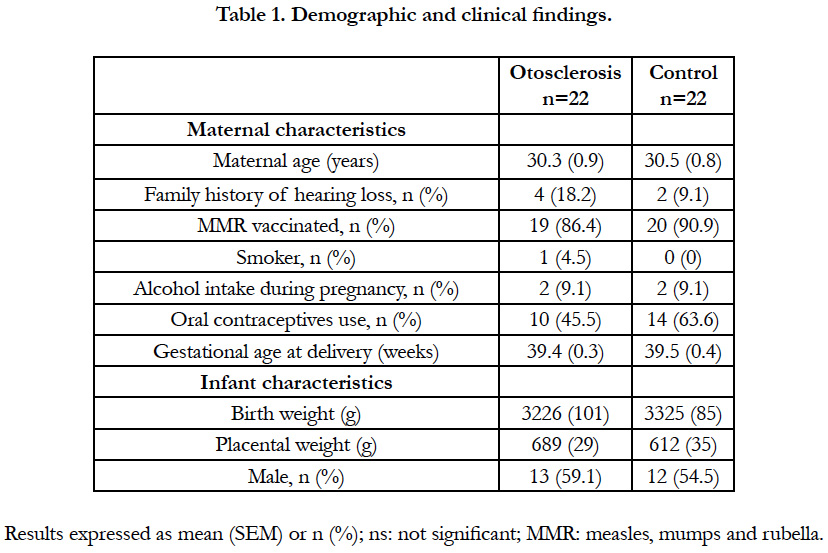

Table 1. Demographic and clinical findings.
Maternal serum concentrations of GH-V, IGF-1, IGF-2 and IGFBP-3 in both the otosclerosis group and the control group increased as pregnancy progressed (Figure 1). Interestingly, maternal serum GH-V concentrations at 26 and 34 weeks of gestation were significantly increased in the otosclerosis group, when compared to the control group (2.53 ± 0.17 ng/ml vs. 1.78 ± 0.19 ng/ml, p = 0.036; 4.34 ± 0.31 ng/ml vs. 3.12 ± 0.18 ng/ ml, p < 0.001, respectively) (Figure 1A). Maternal serum IGF- 1 concentrations at 34 weeks in otosclerosis pregnancies were significantly higher than in the controls (589.1 ± 21.4 ng/ml vs. 499.7 ± 17.8 ng/ml, p < 0.001) (Figure 1B). The increase of IGF-1 was not observed at 26 weeks of gestation. There were no significant differences in serum IGF-2 or IGFBP-1 or IGFBP-3 concentrations between groups (Figure 1C, D and E).
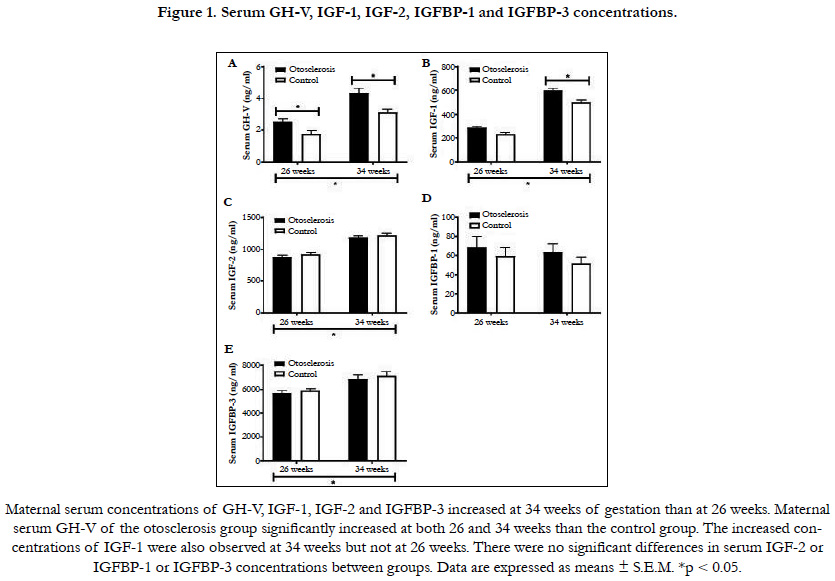

Figure 1. Serum GH-V, IGF-1, IGF-2, IGFBP-1 and IGFBP-3 concentrations.
Discussion
The present study, for the first time, investigated the changes of GH-V, IGFs and IGFBPs in pregnancy complicated with otosclerosis. Otosclerosis is a localized bone remodelling process that occurs in the vicinity of the otic capsule, in which the normal structure of the bone has been replaced by the otosclerotic bone [1]. Histology reveals that otosclerosis as a perturbation of the local control of osteoclasts and osteoblasts, resulting to the failure of regulation of bone remodelling. A number of known factors and most likely a cascade of tightly controlled promoters and inhibitors mediate this process, including growth factors, cytokines, Eicosanoids, enzymes and free radicals [1]. Therefore, GH, as one of the regulators of bone remodelling, is likely to be associated with the development or the process of otosclerosis. In the present study, we found that increased serum GH-V concentrations in pregnancy complicated with otosclerosis, providing further evidence for this hypothesis. GH has been long accepted to be the key hormone in normal postnatal longitudinal bone growth. However, it is now well established that GH also exerts important effects in adults and play a role in bone remodelling, supported by studies in both animals and humans [19]. For example, GH directly stimulates osteoblasts in a number of osteoblastic cells of various origin, including human, chicken, rat and mouse [20-23]. Further study also indicates that GH stimulates osteoblast activity through both its direct and indirect actions on osteoblast differentiation and though its activation of mature osteoblasts via osteoblasts [14]. Moreover, the regulation of bone remodelling also achieves by the GH-induced local production of IGF-1 and by a GH-induced increase in circulating levels of IGF-1, apart from the direct effect of GH [24, 25]. Consistent with this, we found that increased maternal serum IGF-1 at 34 weeks in otosclerosis pregnancies. However, how much of the GH effect is mediated by IGFs and how much is IGF-independent are still unclear.
Conclusions
The findings of our study indicate that the maternal serum concentrations of GH-V and IGF-1 are likely to be associated with the occurrence of otosclerosis during pregnancy. The limitations of this study are that only two sampling time-points (26 and 34 weeks) were applied and the sample sizes were relatively small. Large-scale prospective studies to investigate the change of GH-V and IGF-1 during pregnancy complicated by otosclerosis would provide valuable insights and support our findings.
Acknowledgments
The authors gratefully acknowledge the financial support from the Wenzhou Sciences Foundation (W20153389452). Shutan Liao is funded under an NHMRC Development Grant.
References
- Chole RA, McKenna M. Pathophysiology of otosclerosis. Otology & neurotology. Otol Neurotol. 2001 Mar;22(2):249-57. PubMed PMID: 11300278.
- Parahy C, Linthicum FH Jr. Otosclerosis and otospongiosis: clinical and histological comparisons. Laryngoscope. 1984 Apr;94(4):508-12. PubMed PMID: 6200744.
- Rudic M, Keogh I, Wagner R, Wilkinson E, Kiros N, Ferrary E, et al. The pathophysiology of otosclerosis: Review of current research. Hear Res. 2015 Dec;330(Pt A):51-6. doi: 10.1016/j.heares.2015.07.014. PubMed PMID: 26276418.
- Gristwood RE, Venables WN. Pregnancy and otosclerosis. Clin Otolaryngol Allied Sci. 1983 Jun;8(3):205-10. PubMed PMID: 6883784.
- Gapany-Gapanavicius B. The incidence of otosclerosis in the general population.Isr J Med Sci. 1975 May;11(5):465-8. PubMed PMID: 1158659.
- Lippy WH, Berenholz LP, Schuring AG, Burkey JM. Does pregnancy affect otosclerosis?. Laryngoscope. 2005 Oct;115(10):1833-6. PubMed PMID: 16222205.
- Khosla S, Oursler MJ, Monroe DG. Estrogen and the skeleton. Trends Endocrinol Metab. 2012 Nov;23(11):576-81. doi: 10.1016/j.tem.2012.03.008. PubMed PMID: 22595550.
- Vessey M, Painter R. Oral contraception and ear disease: findings in a large cohort study. Contraception. 2001 Feb;63(2):61-3. PubMed PMID: 11292468.
- Hirt H, Kimelman J, Birnbaum MJ, Chen EY, Seeburg PH, Eberhardt NL, et al. The human growth hormone gene locus: structure, evolution, and allelic variations. DNA. 1987 Feb;6(1):59-70. PubMed PMID: 3030680.
- Newbern D, Freemark M. Placental hormones and the control of maternal metabolism and fetal growth. Curr Opin Endocrinol Diabetes Obes. 2011 Dec;18(6):409-16. doi: 10.1097/MED.0b013e32834c800d. PubMed PMID: 21986512.
- Verhaeghe J. Does the physiological acromegaly of pregnancy benefit the fetus?. Gynecol Obstet Invest. 2008;66(4):217-26. doi: 10.1159/000147167. PubMed PMID: 18645254.
- Alsat E, Guibourdenche J, Couturier A, Evain-Brion D. Physiological role of human placental growth hormone. Mol Cell Endocrinol. 1998 May 25;140(1-2):121-7. PubMed PMID: 9722179.
- Vila G, Luger A. Growth hormone deficiency and pregnancy: any role for substitution?. Minerva Endocrinol. 2018 Mar 8. doi: 10.23736/S0391- 1977.18.02834-1. PubMed PMID: 29521487.
- Nishiyama K, Sugimoto TO, Kaji HI, Kanatani MA, Kobayashi TA, Chihara K. Stimulatory effect of growth hormone on bone resorption and osteoclast differentiation. Endocrinology. 1996 Jan;137(1):35-41. PubMed PMID: 8536635.
- Morel G, Chavassieux P, Barenton B, Dubois PM, Meunier PJ, Boivin G. Evidence for a direct effect of growth hormone on osteoblasts. Cell Tissue Res. 1993 Aug;273(2):279-86. PubMed PMID: 8364969.
- Declau F, van Spaendonck M, Timmermans JP, Michaels L, Liang J, Qiu JP, et al. Prevalence of histologic otosclerosis: an unbiased temporal bone study in Caucasians. Adv Otorhinolaryngol. 2007;65:6-16. PubMed PMID: 17245017.
- Liao S, Vickers MH, Taylor RS, Jones B, Fraser M, McCowan LM, et al. Human placental growth hormone is increased in maternal serum at 20 weeks of gestation in pregnancies with large-for-gestational-age babies. Growth Factors. 2016 Dec;34(5-6):203-209. doi: 10.1080/08977194.2016.1273223. PubMed PMID: 28122472.
- Solomon G, Reicher S, Gussakovsky EE, Jomain JB, Gertler A. Largescale preparation and in vitro characterization of biologically active human placental (20 and 22K) and pituitary (20K) growth hormones: placental growth hormones have no lactogenic activity in humans. Growth Horm IGF Res. 2006 Oct-Dec;16(5-6):297-307. PubMed PMID: 17010651.
- Ohlsson C, Bengtsson BA, Isaksson OG, Andreassen TT, Slootweg MC. Growth hormone and bone. Endocr Rev. 1998 Feb;19(1):55-79. PubMed PMID: 9494780.
- Ernst M, Rodan GA. Increased activity of insulin-like growth factor (IGF) in osteoblastic cells in the presence of growth hormone (GH): positive correlation with the presence of the GH-induced IGF-binding protein BP-3. Endocrinology. 1990 Aug;127(2):807-14. PubMed PMID: 2164921.
- Slootweg MC, van Buul-Offers SC, Herrmann-Erlee MP, Van der Meer JM, Duursma SA. Growth hormone is mitogenic for fetal mouse osteoblasts but not for undifferentiated bone cells. J Endocrinol. 1988 Mar;116(3):R11-3. PubMed PMID: 3351425.
- Scheven BA, Hamilton NJ, Fakkeldij TM, Duursma SA. Effects of recombinant human insulin-like growth factor I and II (IGF-I/-II) and growth hormone (GH) on the growth of normal adult human osteoblast-like cells and human osteogenic sarcoma cells. Growth Regul. 1991 Dec;1(4):160-167. PubMed PMID: 1842348.
- Kassem M, Mosekilde L, Eriksen EF. Growth hormone stimulates proliferation of normal human bone marrow stromal osteoblast precursor cells in vitro. Growth Regul. 1994 Sep;4(3):131-5. PubMed PMID: 7858486.
- Guicheux J, Heymann D, Rousselle AV, Gouin F, Pilet P, Yamada S, et al. Growth hormone stimulatory effects on osteoclastic resorption are partly mediated by insulin-like growth factor I: an in vitro study. Bone. 1998 Jan;22(1):25-31. PubMed PMID: 9437510.
- Ahmed SF, Farquharson C. The effect of GH and IGF1 on linear growth and skeletal development and their modulation by SOCS proteins. J Endocrinol. 2010 Sep;206(3):249-59. doi: 10.1677/JOE-10-0045. PubMed PMID: 20631046.





