Current Approach To Pulmonary Embolism
Ozmen C1*, Demirtas AO2, Demirtas M3
1 Cukurova University Faculty of Medicine, Department of Cardiology, Adana, Turkey.
2 Department of Cardiology, Health Sciences University Adana City Hospital, Adana, Turkey.
3 Department of Cardiology, Cukurova University Faculty of Medicine, Adana, Turkey.
*Corresponding Author
Caglar Ozmen, M.D,
Cukurova University, Faculty of Medicine,
Department of Cardiology, Adana, Turkey.
Tel: 0090-532-583 94 41
E-mail: caglarozm@hotmail.com
Received: August 05, 2018; Accepted: August 29, 2018; Published: August 30, 2018
Citation: Ozmen C, Demirtas AO, Demirtas M. Current Approach To Pulmonary Embolism. Int J Cardiol Res. 2018;5(4):124-130. doi: http://dx.doi.org/10.19070/2470-4563-1800021
Copyright: Ozmen C© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aims: We planned to provide a systematic review of catheter-based therapies in acute pulmonary embolism (PE).
Methods and Results: Studies published in peer-reviewed journals before January 2018 were included and categorised according to the mechanism of thrombus removal: fragmentation, rheolytic therapy, aspiration or catheter-directed thrombolysis. Advantages, challenges and the level of evidence of each device were evaluated. Patients suffering from acute PE,catheter-based therapies are promising options. Most of the procedures are carried using catheter-directed thrombolysis, either ultrasound-assisted or in combination with mechanical fragmentation. Aspiration therapy seems to be promising but sufficient data are not available. Considering the high number of related complications, rheolytic therapy should be applied with caution.
Conclusions: Much more detailed research into the efficiency, safety and the cost-effectiveness of the devices are necessary to be conducted. After all, it is high possibility that with proper patient selection, CBT of massive and submassive can improve the results in patients with PE.
2.Abbreviations
3.Introduction
4.Methods
5.Results
5.1 Mechanical Fragmentation
5.2 Rheolytic Therapy
5.3 Catheter - Directed Therapy
5.4 Aspiration
6.Discussion
7.Conclusions
8.References
Keywords
Aspiration; Catheter Therapy; Pulmonary Embolism; Thrombectomy
Abbreviations
PE: Pulmonary Embolism; PA: Pulmonary Arteries; RV: Right Ventricle; CBT: Catheter-Based Therapy; CDT: Catheter-Directed Thrombolysis; tPA: Tissue Plasminogen Activator.
Introduction
Pulmonary embolism (PE) is a typical case resulting in high morbidity and mortality. Deep vein thrombosis or PE [1] influences approximately 300.000-600.000 people every year. While the three-month mortality is 15% in all patients with PE, it is nearly 50% in massive PE [2].
The existence of acute PE may have different effects varying from indistinct changes in operative capacity to haemodynamic collapse and mortality depending on the thromboembolic mass obstructing the pulmonary circulation, the correlated vasoconstrictor response of the pulmonary arteries (PA), and the capability of the right ventricle (RV) to cope with the acute pressure overload.
Over the last decades, there has been achievement in the treatment of acute PE. Anticoagulation has continued to be the essential of acute PE therapy, which is all needed in the majority of PE patients. The risk stratification is vital and the assessment of the bleeding risk is highly important. In the course of strong PE suspicion and low bleeding risk consideration, anticoagulation should be operated unless contraindicated, even supposing the diagnosis has not been affirmed [3]. In order to prevent deaths from PE, it is highly effective to apply the systemic thrombolytic therapy, yet it significantly increases bleeding, including intracranial and fatal bleeding [4]. The favorable effects of thrombolysis do not compensate the bleeding risk with intermediate-risk patients [5]. For some part of these patients, surgical embolectomy may be a choice. However, the inefficient preoperative state along with a high degree of comorbidity is unable to make such patients suitable for surgery, thus leaving a considerable number of PE patients untreated. Innovative approaches to eliciting or promptly dissolving acute embolism have been recognized over the past several decades.
Unlike the risks related with systemic thrombolytic or surgical treatment, novel catheter-based therapy (CBT) could bring effective thrombus removal. The use of lower doses of thrombolytic agents with newer catheter-based devices along with increasing experience may constantly decrease the major bleeding rates. We will review the techniques utilized and the available evidence base.
Methods
A systematic literature search of the scientific databases PubMed and free search was carried out. Language restrictions were not applied. The references from review articles which were not found by the initial search were included as well. Several mechanical CBTs including mechanical fragmentation, rheolytic therapy, catheter-directed thrombolysis (CDT) and aspiration are available. We evaluated all studies to figure the strengths and challenges of each instrument and the evidence regarding its use in acute PE (Table 1).
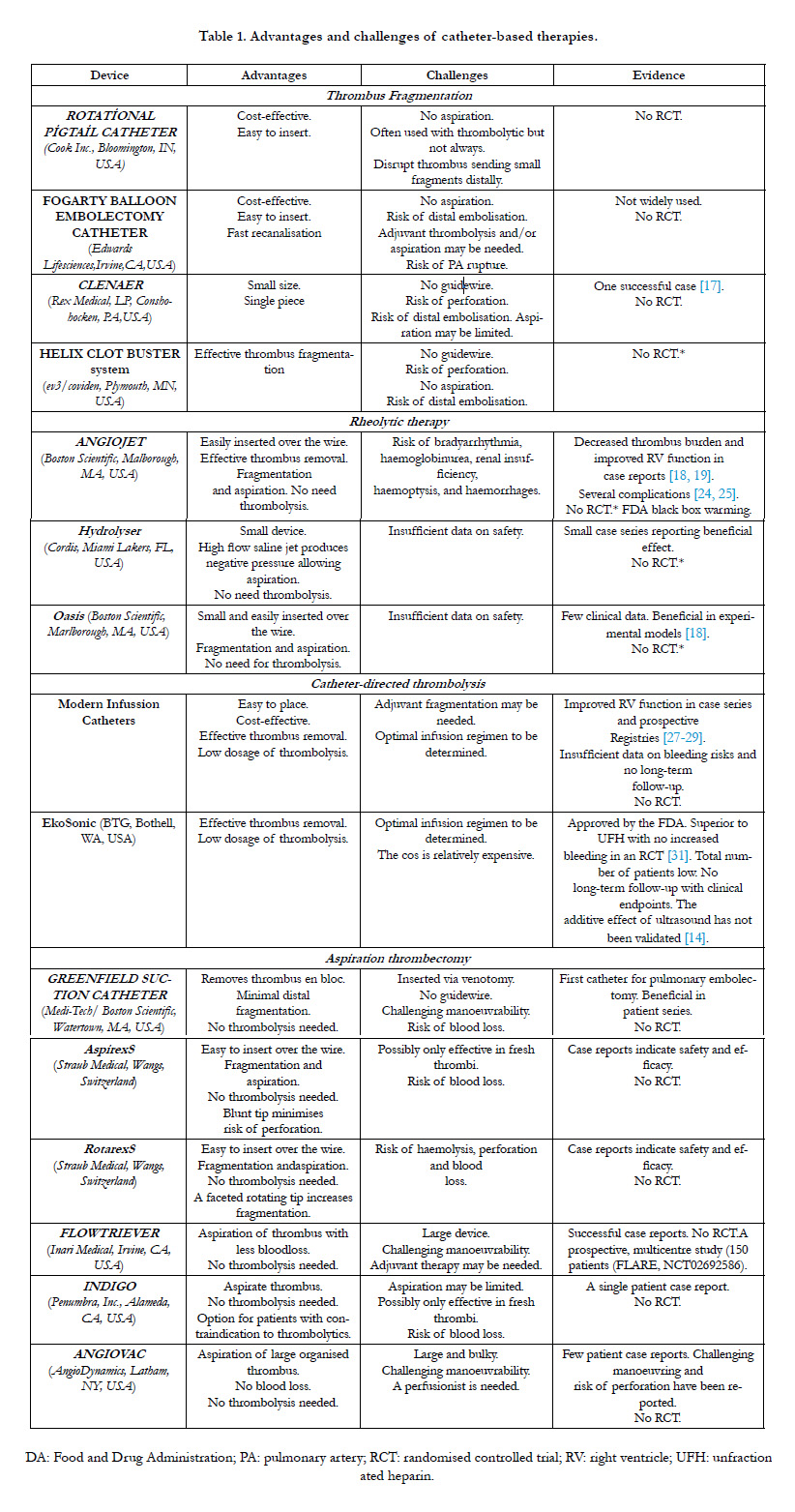

Table 1. Advantages and challenges of catheter-based therapies.
Fragmentation of emboli is a relatively simple and rapid technique, does not require complex resources and easily performed in almost any center. Theoretically, this decreases mechanical obstruction and makes the emboli more accessible for endogenous fibrinolysis. The potential disadvantage of fragmentation is the possibility for hemodynamic deterioration when large initially nonobstructive clots are disrupted and embolize more distally causing occlusion. Therefore, distal embolization may cause an acute, paradoxical elevation of pulmonary vascular resistance and increase strain on the RV [6]. But it does not use lyrics and therefore avoids the attendant bleeding risk, which may be as high as 20% with systemic lysis although likely lower with direct catheter therapy.
Massive PE were approached initially with the “fragmentation technique,” which involves advancing a guide wire into the thrombus, placing a pigtail over the wire and into the clot burden [7], and reforming and manually spinning the pigtail. This is used either alone or in combination with other methods in 70% of patients worldwide undergoing CDT [8]. The rotational pigtail Hunter catheter can be used to access each PA [9]. Alternatively, preshaped catheters such as a Grollman, Monti, or Van Aman catheters (Cook Inc., Bloomington, IN, USA), may be used. The catheter is positioned in the distal aspect of the clot and rotated back and forth through the thrombus while retracting proximally. Studies have shown successful recanalization through the thrombosed vessel, with concomitant reduction in PA pressure and shock index by this method [10]. The strategy is cost-effective, easy to insert and is readily available in most centers, making it one of the most commonly used CBT for acute PE.
The Fogarty arterial balloon embolectomy catheter was the induction of an angioplasty balloon into the thrombus, and then the inflation of the balloon to reduce a large proximally occlusive thrombus into smaller parts passing distally. In order to minimize the risk of PA rupture, it is recommended that smaller balloon be used. Still, the concerns related with residual thrombus and distal embolization bring out the consideration of the balloon angioplasty combined with aspiration or CDT.
The Cleaner rotational thrombectomy system can be applied through a 6 Fr sheath and is an agreeable option in view of its comparably small form and its considerably atraumatic tip. The distal end of the device is in a sinusoidal shape that can rotate up to 4000 RPM to fragment thrombus. Introducing without the use of a guidewire may deduce a risk of vessel perforation. Additionally, it is not certain if the aspiration of thrombus through the small sheath is adequate since it evokes a risk of distal fragmentation. Just one patient with PE has been reported regarding the use of Cleaner off-label [11].
The Helix Clot Buster System is a relatively low profile single-use catheter with a 7 Fr outer diameter that can be advanced into the pulmonary arteries. It works via an impeller at the catheter tip that rotates at over 140,000 RPM aspirating and macerating thrombus to less than 10 microns.
Rheolytic thrombectomy involves thromboembolic fragmentation using a saline jet directed from the tip of the catheter with simultaneous emulsified thrombus removal via a separate channel. In the pulmonary arteries, a 6 or 8 Fr system is typically advanced over an 0.035-in guidewire directly into the thrombus. Based on the Bernoulli principle, pressurized jet streams are used to create a relatively low-pressure zone localized around the catheter [12].
The AngioJet thrombectomy device permits the local injection of thrombolytic agents by the “power pulse” spray technique, forcing the drug into the emboli. The AngioJet device rapidly infuses heparinized saline, up to 360 mph, via the catheter endhole, reducing local pressure to a -600 mmHg, extracting soft thrombus into the catheter via a distal sideport. Initially, the catheter can be moved slowly back and forth in the affected main or lobar PA in pulse spray mode to infuse low dose tissue plasminogen activator (tPA) (18-20 mg mixed in 100mL normal saline) throughout the thrombus. Following a prolonged pause, in regular mode, the catheter is again advanced and retracted within the thrombus in thrombectomy mode to aspirate clot [13]. However, significant limitations have included the development of bradycardia, possibly due to the release of bradykinin, adenosine, or potassium secondary to hemolysis. This complication usually occurs with prolonged runs of more than 20 seconds and may lead to heart block or asystole [14]. Also, massive hemoptysis, renal failure, and death from bradycardia and apnea have been reported [15]. With all these complications, prompting FDA to issue a black-box warning on the device. Based on safety concerns, some nonetheless advocate for its use as a second line option for PE, given prior success and it is still being used in some European centers. A temporary pacemaker and close monitoring of hemodynamics, renal function and electrolyte status are however pivotal.
It works by using the Venturi effect and is a 6-French/7-French triple lumen catheter with a small injection lumen, a larger exhaust lumen, and a 0.020- inch guidewire lumen. The device is available in different lengths and is activated with a standard pressure injector filled with saline.
This is a 6-French thrombectomy system, very similar to the Hydrolyser device. It works on the Venturi principle and has just two lumens.
This treatment strategy requires selective infusion catheter placement in the pulmonary artery within the embolus, followed by continuous infusion of thrombolytic drugs over a period. The treatment objective is to accelerate thrombus dissolution and achieve rapid reperfusion of the pulmonary arteries. The central location of clot is especially important in consideration for (CDT). An ideal candidate is one with main or lobar bulky thrombus into which a lysis cathetermay be securely embedded. Thrombolysis may be administered by standard infusion catheters, or by newly designed catheters such as the Uni*FuseTM or Pulse*Spray® (both AngioDynamics, Latham, NY, USA) which have special side holes for optimal intra-thrombus drug delivery. Depending on individual bleeding risk, CDT may be performed with under 30 mg tPA injection, significantly lower than the systemic dose of 100 mg. A meta-analysis evaluated 16 studies of CDT and found a major complication rate of 4.7 percent and intracranial hemorrhage rate of 0.35 percent [16]. A recent propensity-matched analysis of inhospital outcomes utilized the National Readmission Database to compare systemic vs. CDT and demonstrated lower in-hospital mortality and bleeding in patients who received CDT [17]. But, there have been no prospective, randomized trials comparing systemic to CDT. The goal of CDT is rapid debulking of central occlusive thrombus to relieve life-threatening heart strain and improve pulmonary perfusion and oxygenation.
USAT uses ultrasonic waves purportedly to disrupt the fibrin structure of the thrombus, allowing more binding sites for the thrombolytic agent. The 5.2-F infusion catheter contains three lumens with one for the inner ultrasound cable, one for the drug infusion, and one for the coolant. The total tPA dose is typically between 12 and 24 mg, delivered over 12 to 24 hours. The best studied and only U.S. Food and Drug Administration-approved catheter-directed device for management of PE is the EkoSonic Endovascular System (BTG, Bothell, WA, USA).
The ULTIMA trial randomized 59 intermediate-risk patients to either anticoagulation alone or USAT with 10 mg of tPA delivered to each treated lung over 15 hours in addition to anticoagulation. The study showed CDT improved right ventricular dilation and dysfunction more quickly without increased risk of death, major bleeding, or intracranial hemorrhage. However, at the 90-day follow-up, the RV/LV ratio was equalized between the two groups. The SEATTLE II study supported these findings, a prospective, multicentre, single-arm trial of 150 intermediate- and high-risk patients [18]. The findings demonstrated that USAT resulted in decreased RV dilation and reduced pulmonary pressures, and they further demonstrated reduced anatomic thrombus burden using the modified Miller index. As with ULTIMA, there were no ICH events. The other study which named PERFECT was a prospective registry with 101 patients with massive or submassive PE [19]. In all, 86% of massive and 97% of submassive patients with PE achieved clinical success without major complications.
A randomized trial (SUNSET sPE, NCT02758574) will investigate whether ultrasound improves outcome compared to non-ultrasound-assisted CDT, which is currently unknown. In patients suffering from deep vein thrombosis, there are no additional beneficial effects of USAT [20]. The other randomized trial (OPTALYSE PE) can offer additional data on whether lower doses and shorter infusions are beneficial in the intermediate-risk PE population. Treatment with USAT using a shorter delivery duration and lower-dose tPA (4 mg infusion over two hours) was associated with improved RV function and reduced clot burden compared with baseline [21].
Simple vacuum assisted thrombectomy is an easy mechanical option using an end hole catheter. Several aspiration techniques have been employed and can be attempted using regular 8-F or larger guide catheters or more specialized catheters. The end hole catheter is directed to the thrombus and manual suction is performed through the catheter with a large syringe.
The Greenfield embolectomy device was the first catheter designed for percutaneous embolectomy via thromboaspiration. The device allowed extraction of the centrally located emboli by using sustained suction with a large syringe. The guide catheter is advanced into the embolism in the right or left PA. Suction is applied with a 20- to 50- mL syringe while the catheter is moved slowly back and forth over several centimeters within the clot. The device is inserted by a surgical venotomy as insertion is not possible through conventional sheath access. Despite reports of a success rate of 76%, the catheter has not achieved broad use in clinical practice [22].
The AspirexS and RotarexS have a metal helix that can be rotated inside the catheter to create a vacuum at the tip of the catheter based on the principle of Archimedes’ screw. Once within thrombus, an inner spiral coil undergoes highspeed rotation (40,000 rpm) aspirating thrombus through the port and transporting it down the spiral shaft much like a screw. The catheter is connected to an external collecting system where thrombus is deposited. The tip of the AspirexS is fixed and blunt, so fragmentation is limited. The device is therefore only indicated for use with fresh thrombus. The tip of the RotarexS is faceted and rotates together with the helix which enables fragmentation of more rigid thrombus material, but with a risk of damaging the vessel. Kucher et al., [23] described the first use in PEand one study of 30 patients with massive and submassive PE reported a complete clearance rate of >90% in over 80% of patients, with improvement in right heart strain; there were two major (bradycardia) and four minor (two access site hematomas, and two hemoptysis) procedure-related complications [24].
The Flowtriever system is a catheter-based mechanical device for percutaneous endovascular retrieval of emboli with the aim of use in the proximal pulmonary arterial system. It consists of a catheter with a self-expanding nitinol mesh including three adjacent nitinol disks.The collapsed Flowtriever is passed into the thrombus via the guide catheter inside a delivery catheter so that the sheared nitinol discs are placed within the thrombus. The delivery catheter is retracted that positions the self-expanding discs and entraps the thrombus. Next, the discs are resheathed by the use of the Retraction Aspirator Device, regulating the mechanical retraction of clot through the Flowtriever and aspiration of the thrombus through the guide catheter. Both clot extraction and improved perfusion may achieve clinical improvement through penetrating the emboli. Insufficient thrombus removal and maneuverability may be the challenges.
The case of a successful use of the Flowtriever on a critically ill massive PE patient having failed systemic thrombolysis has been reported [25]. The device is being examined in a large prospective trial regarding intermediate-risk (submassive) PE patients. Patients are now being engaged in a prospective, multicenter, single-arm study. The goal of the Flowtriever Pulmonary Embolectomy Clinical Study (FLARE, NCT02692586) is to evaluate the safety and success of the Flowtriever in 150 patients with acute PE from 20 sites in the USA [26].
The Indigo mechanical thrombectomy system consists of an aspiration catheter, a pump providing suction and a separator wire. Although the catheter aspirates, a Penumbra Separator is rapidly advanced and quickly retracted through the catheter tip. The Separator works to break down thrombus and facilitate aspiration. An advantage of this technique is that it only requires an 8-F venous sheath for access. One limitation of any aspiration/suction device is blood loss. Only a few cases of PE treatment have been reported with this device [27].
The Angiovac Cannula is A 22 Fr catheter with a funnel-shaped tip is directed to the thrombus at which point the thrombus is aspirated into a cardiopulmonary pump. The thrombus is retained within the pump and the aspirated blood is reperfused into the patient via a second 17 Fr venous cannula. Because of the circuit required, a unique requirement of the AngioVac system is a perfusionist, who must maintain the pump while thrombus is being aspirated. The other limitation of this device is include the large dual sheaths required for access, leading to a higher likelihood of bleeding complications, and the relatively stiff suction catheter, which can be difficult to maneuver into the RV and PA. It hasbeen used offlabel in small case series of patients with PE withsome success [28]. The complexity of the setup, size of the device, and limited maneuverability may limit its use but very large amounts of clot can be removed very quickly once the procedure is initiated.
It is reported that modern suction thrombectomy catheters such as the Prono XL extraction catheter available in 10-,12- and 14-Fr sizes are effective in acute massive PE as they reduce the evident thrombus or the mean PA pressure. The extraction of thromboembolism from the main PA can be managed via the pigtail version while the straight version is for segmental PAs. Besides, the pigtail version can be used like a rotational catheter for fragmenting thrombus manually, concurrently suctioning clot via distal sideholes with the use of a 60-ml syringe.
Discussion
While the use of CBTs for PE is increasing, the definite number of acute PE patients receiving CBT is not known. In one recent longitudinal report, it was stated that 9% of patients with acute PE received CBT [29]. yet in most hospitals, the only available treatment sources are anticoagulation and systematic thrombolysis. Before 2008, 70% of CBTs included mechanical fragmentation through pigtail catheter [30]. Following the FDA approval of the EkoSonic, the involvement of mechanical fragmentation as the preferred CBT has been surpassed by USAT. While rheolytic catheters were used largely, the black-box warning from the FDA has limited its current use. Aspiration therapy is encouraging, the devices still need further development and data are lacking though. The requirement of more than 12 hours of therapy with CDT may be a long process in high-risk patients, introducing that aspiration therapy with faster thrombus removal may present a valid treatment option.
CBTs are recommended by European guidelines as an lternative treatment for patients with high-risk PE and having contraindications to or insufficient effect of systemic thrombolysis (Class IIa, level C). The application of CBTs is recommended in patients with a high bleeding risk (Class IIb, level B), with the ULTIMA trial as the only reference in the event of a lack of evidence.
The literature approving CBTs in acute PE is mainly derived from case reports and recollective patient series,bringing in a risk of publication bias. Moreover, the patient population in these reports may be highly selected. Consequently, the reported promising success rates and small complication rates should be delicately interpreted [30]. Exceptional studies comparing the various CDT against each other or systemic thrombolysis are not available.The data regarding the current rate of CDT use in intermediate-risk PE and the potential risks and costs of these interventions, assessment of long-term outcomes, including pulmonary hypertension and exercise tolerance, along with higher quality short-term clinical outcome are necessary.
Additionally, these studies all focused on the investigation of the effects of CDT, thus the evidence supporting this approach is increasing whereas the evidence for other approaches is rare. Still, a prospective study has not evaluated the long-term favors of CDT in the submassive PE population. The effect of CDT to prevent the commonly named ‘post PE syndrome’ 2-3 years following the acute PE event has not been studied yet. It would be ideal to conduct a prospective study in high-risk submassive PE patients to compare anticoagulation alone to CDT using both short and long-term endpoints.
Due to the high bleeding risk of systemic thrombolysis, the clinical use to patients at the highest risk of early mortality is limited. Provided that large-scale randomized clinical trials assure that novel CBTs provide adequate reduction in thrombus burden with a lower complication scale, this could bring a paradigm shift likely of acute myocardial infarction and eventually make systemic thrombolysis dated in the treatment of acute PE.
Considering the category of submassive PE patients, we believe that there may be subset of patients that will probably benefit from CDT more compared to others. Presently, it seems to be a gap between the high morbidity and mortality rate of intermediate-risk PE treated with anticoagulation only and the insufficiency of the overall benefit of systemic thrombolysis in this patient subgroup [31]. Besides, it is crucial that hospitals have developed PE response teams (PERT) to focus on these issues, let open dialogue and attain experience with this complex patient population.
We support a more systematic approach where through assisting proper scientific inquiry, clinicians and researchers take the leading role of advancing this promising field. Using committed technological advances, such as the development of catheters and pharmacomechanical devices, especially for massive and submassive PE, it is probable that this disease may become a predominantly endovascularly treated one. The improvement of current strategies along with future technologic developments will enable physicians and patients with a selection of options to ease symptom burden, delay morbidity and mortality and to promote the quality of life.
The cost of CBTs for PE is another issue. The price range of the devices vary greatly and it can be high. With the few efficient data in our hands and due to the lack of long-termfollow-up, it is not possible to figure out the cost-effectiveness of these novel CBTs at present.
Conclusions
The most common treatment approach for massive PE is systemic thrombolysis, yet there is a considerable subset of that patient population with no tolerance to thrombolytic therapy. Besides, systemic anticoagulation may not give the desired clinical improvement in patients with submassive PE. As a result, for patients suffering from acute PE, CBTs are promising options. Newer guidelines employ CDT in treatment protocols. Also, the FDA approved USAT for the treatment of PE. Most of the procedures are carried using CDT, either ultrasound-assisted or in combination with mechanical fragmentation. Aspiration therapy seems to be promising but sufficient data are not available. Considering the high number of related complications, rheolytic therapy should be applied with caution. After all, it is high possibility that with proper patient selection, CBT of massive and submassive can improve the results in patients with PE.
A notably individualized treatment approach giving highly importance to the selection of patients.The type of therapy and operator and hospital experience can maximize the benefits of an interventional approach and minimize the harm. It is necessary that much more detailed research into the efficiency, safety and the cost-effectiveness of the devices be conducted.
References
- Zarghouni M, Charles HW, Maldonado TS, Deipolyi AR. Catheterdirected interventions for pulmonary embolism. Cardiovasc Diagn Ther. 2016 Dec;6(6):651-661. doi: 10.21037/cdt.2016.11.15. PubMed PMID: 28123985.
- Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999 Apr 24;353(9162):1386-9. PubMed PMID: 10227218.
- Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016 Feb;149(2):315-352. doi: 10.1016/j. chest.2015.11.026. Epub 2016 Jan 7. PubMed PMID: 26867832.
- Chatterjee S, Chakraborty A, Weinberg I, Kadakia M, Wilensky RL, Sardar P, et al. Thrombolysis for pulmonary embolism and risk of all-cause mortality, major bleeding, and intracranial hemorrhage: a meta-analysis. JAMA. 2014 Jun 18;311(23):2414-21. doi: 10.1001/jama.2014.5990. PubMed PMID: 24938564.
- Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, PEITHO Investigators, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014 Apr 10;370(15):1402-11. doi: 10.1056/ NEJMoa1302097. PubMed PMID: 24716681.
- Nakazawa K, Tajima H, Murata S, Kumita SI, Yamamoto T, Tanaka K. Catheter fragmentation of acute massive pulmonary thromboembolism: distal embolisation and pulmonary arterial pressure elevation. Br J Radiol. 2008 Nov;81(971):848-54. doi: 10.1259/bjr/93840362. PubMed PMID: 18941044.
- Furlan A, Patil A, Park B, Chang CC, Roberts MS, Bae KT. Accuracy and reproducibility of blood clot burden quantification with pulmonary CT angiography. AJR Am J Roentgenol. 2011 Mar;196(3):516-23. doi: 10.2214/ AJR.10.4603. PubMed PMID: 21343492.
- Sckmitz-Rode T, Janssens U, Schild HH, Basche S, Hanrath P, Günther RW. Fragmentation of massive pulmonary embolism using a pigtail rotation catheter. Chest. 1998 Nov;114(5):1427-36. PubMed PMID: 9824024.
- Rosen G, Kowalik KJ, Ganguli S, Hunter DW. The Hunter pulmonary angiography catheter for a brachiocephalic vein approach. Cardiovasc Intervent Radiol. 2006 Nov-Dec;29(6):997-1002. PubMed PMID: 16779693.
- Schmitz-Rode T, Janssens U, Duda SH, Erley CM, Günther RW. Massive pulmonary embolism: percutaneous emergency treatment by pigtail rotation catheter. J Am Coll Cardiol. 2000 Aug;36(2):375-80. PubMed PMID: 10933345.
- Barjaktarevic I, Friedman O, Ishak C, Sista AK. Catheter-directed clot fragmentation using the Cleaner™ device in a patient presenting with massive pulmonary embolism. J Radiol Case Rep. 2014 Feb 1;8(2):30-6. doi: 10.3941/jrcr.v8i2.1455. PubMed PMID: 24967017.
- Chechi T, Vecchio S, Spaziani G, Giuliani G, Giannotti F, Arcangeli C, et al. Rheolytic thrombectomy in patients with massive and submassive acute pulmonary embolism. Catheter Cardiovasc Interv. 2009 Mar 1;73(4):506-13. doi: 10.1002/ccd.21858. PubMed PMID: 19235240.
- Jaber WA, Fong PP, Weisz G, Lattouf O, Jenkins J, Rosenfield K, et al. Acute pulmonary embolism: with an emphasis on an interventional approach. J Am Coll Cardiol. 2016 Mar 1;67(8):991-1002. doi: 10.1016/j. jacc.2015.12.024. PubMed PMID: 26916490.
- Zhu DW. The potential mechanisms of bradyarrhythmias associated with AngioJet thrombectomy. J Invasive Cardiol. 2008 Aug;20(8 Suppl A):2A-4A. PubMed PMID: 18830014.
- Arslan B, Turba UC, Matsumoto AH. Acute renal failure associated with percutaneous mechanical thrombectomy for iliocaval venous thrombosis. Semin Intervent Radiol. 2007 Sep;24(3):288-95. doi: 10.1055/s-2007-985736. PubMed PMID: 21326470.
- Bloomer TL, El‐Hayek GE, McDaniel MC, Sandvall BC, Liberman HA, Devireddy CM, et al. Safety of catheter‐directed thrombolysis for massive and submassive pulmonary embolism: Results of a multicenter registry and meta‐analysis. Catheter Cardiovasc Interv. 2017 Mar 1;89(4):754-760. doi: 10.1002/ccd.26900. PubMed PMID: 28145042.
- Arora S, Panaich SS, Ainani N, Kumar V, Patel NJ, Tripathi B, et al. Comparison of in-hospital outcomes and readmission rates in acute pulmonary embolism between systemic and catheter-directed thrombolysis (from the National Readmission Database). Am J Cardiol. 2017 Nov 1;120(9):1653- 1661. doi: 10.1016/j.amjcard.2017.07.066. PubMed PMID: 28882336.
- Piazza G, Hohlfelder B, Jaff MR, Ouriel K, Engelhardt TC, Sterling KM, et al. A prospective, single-arm, multicenter trial of ultrasound-facilitated, catheter-directed, low-dose fibrinolysis for acute massive and submassive pulmonary embolism: the SEATTLE II study. JACC Cardiovasc Interv. 2015 Aug 24;8(10):1382-92. doi: 10.1016/j.jcin.2015.04.020. PubMed PMID: 26315743.
- Kuo WT, Banerjee A, Kim PS, DeMarco Jr FJ, Levy JR, Facchini FR, et al. Pulmonary embolism response to fragmentation, embolectomy, and catheter thrombolysis (PERFECT): initial results from a prospective multicenter registry. Chest. 2015 Sep;148(3):667-673. doi: 10.1378/chest.15-0119. PubMed PMID: 25856269.
- Avgerinos ED, Mohapatra A, Rivera-Lebron B, Toma C, Kabrhel C, Fish L, et al. Design and rationale of a randomized trial comparing standard versus ultrasound-assisted thrombolysis for submassive pulmonary embolism. J Vasc Surg Venous Lymphat Disord. 2018 Jan;6(1):126-132. doi: 10.1016/j. jvsv.2017.09.004. PubMed PMID: 29248101.
- Tapson VF, Sterling K, Jones N, Elder M, Tripathy U, Brower J, et al. A randomized trial of the optimum duration of acoustic pulse thrombolysis procedure in acute intermediate-risk pulmonary embolism: the OPTALYSE PE trial. JACC Cardiovasc Interv. 2018 Jul 23;11(14):1401-1410. doi: 10.1016/j.jcin.2018.04.008. PubMed PMID: 30025734.
- Greenfield LJ, Proctor MC, Williams DM, Wakefield TW. Long-term experience with transvenous catheter pulmonary embolectomy. J Vasc Surg. 1993 Sep;18(3):450-7. PubMed PMID: 8377239.
- Kucher N, Windecker S, Banz Y, Schmitz-Rode T, Mettler D, Meier B, et al. Percutaneous catheter thrombectomy device for acute pulmonary embolism: in vitro and in vivo testing. Radiology. 2005 Sep;236(3):852-8. PubMed PMID: 16014440.
- Dumantepe M, Teymen B, Akturk U, Seren M. The efficacy of rotational thrombectomy on the mortality of patients with massive and submassive pulmonary embolism. J Card Surg. 2015 Apr;30(4):324-32. doi: 10.1111/jocs.12521. PubMed PMID: 25683156.
- Weinberg AS, Dohad S, Ramzy D, Madyoon H, Tapson VF. Clot extraction with the FlowTriever device in acute massive pulmonary embolism. J Intensive Care Med. 2016 Sep 6. PubMed PMID: 27601482.
- FlowTriever Pulmonary Embolectomy Clinical Study (FLARE).
- Young S, Pritzker M, Rosenberg M. Vacuum-assisted thrombectomy of massive pulmonary embolism. J Vasc Interv Radiol. 2016 Jul;27(7):1094-6. doi: 10.1016/j.jvir.2016.01.145. PubMed PMID: 27338502.
- Al-Hakim R, Park J, Bansal A, Genshaft S, Moriarty JM. Early experience with AngioVac aspiration in the pulmonary arteries. J Vasc Interv Radiol. 2016 May;27(5):730-4. doi: 10.1016/j.jvir.2016.01.012. PubMed PMID: 27106647.
- Heberlein WE, Meek ME, Saleh O, Meek JC, Lensing SY, Culp WC. New generation aspiration catheter: Feasibility in the treatment of pulmonary embolism. World J Radiol. 2013 Nov 28;5(11):430-5. doi: 10.4329/wjr. v5.i11.430. PubMed PMID: 24349647.
- Kabrhel C, Rosovsky R, Channick R, Jaff MR, Weinberg I, Sundt T, et al. A multidisciplinary pulmonary embolism response team: initial 30-month experience with a novel approach to delivery of care to patients with submassive and massive pulmonary embolism. Chest. 2016 Aug;150(2):384-93. doi: 10.1016/j.chest.2016.03.011. PubMed PMID: 27006156.
- Kuo WT, Gould MK, Louie JD, Rosenberg JK, Sze DY, Hofmann LV. Catheter-directed therapy for the treatment of massive pulmonary embolism: systematic review and meta-analysis of modern techniques. J Vasc Interv Radiol. 2009 Nov;20(11):1431-40. doi: 10.1016/j.jvir.2009.08.002. PubMed PMID: 19875060.





