Relationship of Drug-Drug Interactions with Hospital Diagnoses Associated to Adverse Drug Reactions: a Retrospective Study of Billing Data in Austria
W. Gall1, L. Neuhofer1, C. Rinner1, G. Endel2, W. Grossmann3, B. Marzluf4, M. Wolzt4*
1 Center for Medical Statistics, Informatics, and Intelligent Systems, Medical University of Vienna, Spitalgasse 23, 1090 Vienna, Austria.
2 Section of Evidence Based Medicine (EBM) and Health Technology Assessement (HTA), Main Association of Austrian Social Security Organisations,
Austria.
3 Research Group Knowledge Engineering, Faculty of Computer Science, University of Vienna, Währinger Strasse 29, 1090 Vienna, Austria.
4 Department of Clinical Pharmacology, Medical University of Vienna, Spitalgasse 23, A-1090 Vienna, Austria.
*Corresponding Author
Michael Wolzt MD,
Department of Clinical Pharmacology,
Medical University of Vienna,
Spitalgasse 23, A-1090 Vienna, Austria.
Tel: +43-1-40400-29810
Fax: +43-1-40400-29980
E-mail: michael.wolzt@meduniwien.ac.at
Article Type: Research Article
Received: May 08, 2015; Accepted: May 26, 2015; Published: May 27, 2015.
Citation: M. Wolzt et al., (2015) Relationship of Drug-Drug Interactions with Hospital Diagnoses Associated to Adverse Drug Reactions: A Retrospective Study of Billing Data In Austria. Int J Clin Pharmacol Toxicol, S1:001, 1-6. doi: dx.doi.org/10.19070/2167-910X-SI01001
Copyright: M. Wolzt© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: The objective of this study was to identify hospitalisations in Austria caused by adverse drug reactions (ADR) and to analyse preceding medication for the risk of drug-drug interactions (DDI) based on healthcare billing databases.
Methods: A retrospective study was performed using the billing data of the Austrian health system. The research database of the Main Association of Austrian Social Security Organisations was used, which contains hospital discharge diagnoses and all medications reimbursed from prescriptions for 5,046,325 adult Austrian patients in 2006 and 2007.
Results: 0.4% of the population was discharged with at least one diagnosis indicating an ADR during the observation period. 1.5% of hospitalised patients had a diagnosis related to an ADR. Of these, a DDI was identified in 68% (13,511 subjects) and a severe interaction in 12% (2,412 subjects), respectively.
Conclusions: Billing data provide important information to complement reporting systems for drug safety. These database searches may contribute to signal and hypothesis generation.
2.Introduction
3.Methods
3.1.Study population
3.2.Additional data sources
3.3.ADR and DDI identification
4.Results
4.1.ADR diagnoses
4.2.Drug-drug interactions
5.Discussion
6.Conclusion
7.Acknowledgments
8.References
Keywords
Adverse Drug Events; Pharmacovigilance; Drug Safety; Hospital Diagnoses; Drug Reimbursement.
Introduction
The European Directive on Pharmacovigilance [1] defines adverse drug reactions (ADR) as “a response to a medicinal product which is noxious and unintended” including medical errors. While some ADR appear preventable, others are unexpected on the basis of available product information or poorly predictable because of drug-drug interactions (DDI).
ADR affect an unknown quantity of the population and are a common cause for hospital admissions [2]. Several studies have estimated the incidence of ADR-related hospital admissions with data obtained from discharge letters and nationwide analysis, for example in Spain [3], England [4] or in the Netherlands [5].
It is estimated that 2-6% of hospitalisations are due to ADR [6-8]. A review of 25 studies [9] found a median ADR rate of 5.3% with a range between 0.2% and 15.7%. In an effort to estimate patient risks on a population-based level most studies calculate the proportion of ADR-hospital admissions, others the admissions per treated patients. For example Schneeweiss et al. [7] calculate 9.5 admissions per 10.000 treated patient in Germany. ADR admissions occur more often in elderly people [10-13] and are caused by a few number of medications [10]. Besides morbidity and mortality, ADR are responsible for a substantial utilisation of bed capacity and treatment costs in hospital [14-16] and can trigger reduced precriptions [17].
ADR reports emerge from pre- or post-marketing trials or from spontaneous case reports. Similar to other European countries [18] the reporting activity by health care professionals in Austria has increased since 2006, but remains at a very low level. In Austria with approximately 8 million inhabitants the Austrian Agency for Health and Food Safety (AGES) received 323 ADR reported in the year 2006, and an average of 704 ADR per year between 2006 and 2013 [19]. Particularly in a country where the spontaneous reporting system is underdeveloped, new highly-efficient approaches that can be realized with limited resources need to be explored.
ADR may be identified from healthcare system databases. The Main Association of Austrian Social Security Organisations maintains a data repository of patient- and treatment- related medical data (GAP-DRG) for accountancy and billing for all subjects treated in Austria. For research purposes this database has added information of all reimbursed medications dispensed at pharmacies and diagnoses from hospital discharges covering the years 2006 and 2007.
The goal of this study was to capture ADR-related hospital discharge diagnoses on a population level in Austria based on billing data and to search for possible DDIs of medications dispensed preceding these hospital stays.
Methods
The study protocol was approved by the Ethics Committee of the Medical University of Vienna (EK #1131/2013).
Data in the GAP-DRG database from 2006 and 2007 were collected by the Main Association of Austrian Social Security Organisations and anonymised. All hospital diagnoses and reimbursed medications dispensed at pharmacies upon prescription (including resident physicians with in-house pharmacies) for the Austrian population during the years 2006 and 2007 were available for analysis. Data from patientsyounger than 20 were excluded from analysis.
A list of 505 ADR-related diagnoses from a study of Stausberg and Hasford [20] was used to identify a relationship between medicines and hospital discharge diagnosis. The diagnoses were encoded in the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, German Modification (ICD-10-GM) and grouped in seven categories of ADR likelyhood (Table 1).
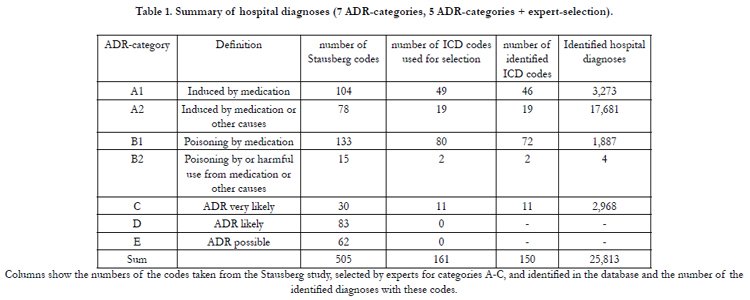

Table 1. Summary of hospital diagnoses (7 ADR-categories, 5 ADR-categories + expert-selection).
For the analysis of possible DDIs the Austria-Codex was integrated into the GAP-DRG-database. The Austria-Codex contains all medications available in Austria and flags DDI information [21]. The Austria Codex categorizes the DDI warnings into severe, moderate and minor interactions. Severe DDIs may be lifethreatening or cause permanent damage.
For this study the ICD-10 list of Stausberg and Hasford [20] was adapted by pharmacological experts. ADR caused by medicines dispensed during hospitalisations were reviewed. Where appropriate, an ADR was removed when the effect was not unexpected. For example, code D 61.10 (Drug-induced aplastic anaemia) was removed when the diagnosis was linked to cytotoxic chemotherapy during a preplanned hospital stay. Further, direct drug-induced ADR such as allergic/hypersensitivity reactions or the code L27.0 “generalized skin eruption due to drugs and medicaments” were not considered for DDI analysis due to the monocausal nature of event. After this careful revision the list of ICD-10 codes in the database was reduced to 161 diagnoses (see Appendix).
Hospital discharge diagnoses from 1.7.2006–30.9.2007 were analysed. The remaining two quarters before and the quarter after this period were taken for the evaluation of medications before and after index hospitalisation.For the analysis of a relationship between an ADR-diagnosis and DDIs, only ICD-10 diagnoses with ≥100 occurences in these five quarters were considered. Other diagnoses were considered as too rare to provide a clinically relevant signal, unless categorized as induced directly by medication.
The prescribed daily dosage was not accessible from the database. Thus, the nominal intake period per drug was set to 30 days. This was intentionally chosen as standard package sizes cover mostly a 30 days period, except for antibiotics. In addition, this conservative definition prevents an overestimation of possible interactions and attributes DDIs mainly to long-term use of medication. Further, this strategy mitigates a bias resulting from different reporting periodicities of the medication data by health insurances.
Data were prepared using the PostgreSQL database Version 9.1.3. Descriptive statistical analyses were performed with Excel.
Results
5,046,325 subjects had a medical consultation or a prescription reimbursed during the five quarters between 01.07.2006 and 30.09.2007. 1,324,320 subjects were admitted to a hospital in this period, with a total of 2,530,313 hospitalisations.
Direct drug-induced or very likely ADR were found in 25,813 discharge diagnoses of 25,535 hospitalisations from 19,760 subjects. These ADR comprised 150 different ICD codes (Table 1). Thus approximately 0.4% of all subjects had a hospitalisation with an ADR-related diagnosis.
19,760 patients (1.5% of hospitalised subjects) had an ADRrelated diagnosis.In this group with an ADR-related diagnosis, a higher proportion of females was observed across all age groups. This sex difference of ADR incidence persisted when data were normalized for age-group proportions in the Austrian population [22] (Figure 1).
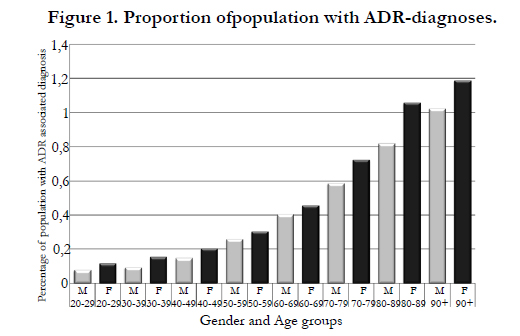
Figure 1. Proportion ofpopulation with ADR-diagnoses.
All ADR-related hospital diagnoses were analysed for potential DDIs. In 13,511 subjects (68%) an interaction could be identified. This DDI was classified as severe in 2,412 subjects (12%). Most frequent DDI signals are presented in Table 2. Table 3 lists the substance groups involved in the DDI warnings.
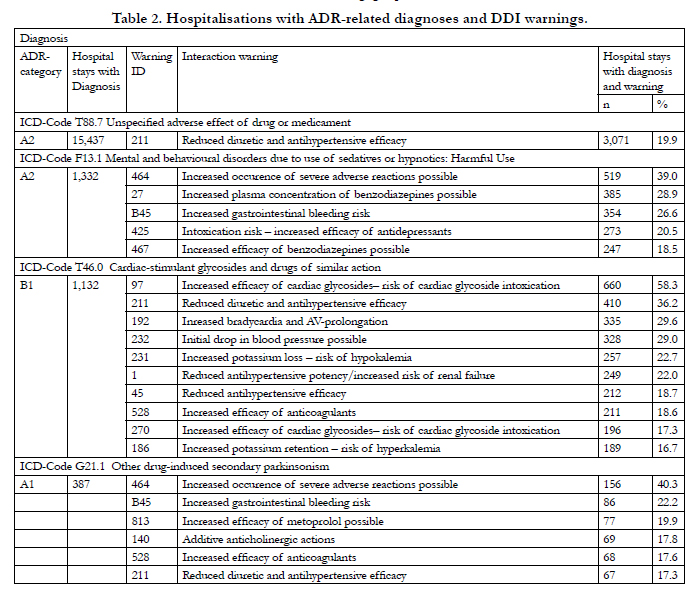
Table 2. Hospitalisations with ADR-related diagnoses and DDI warnings.
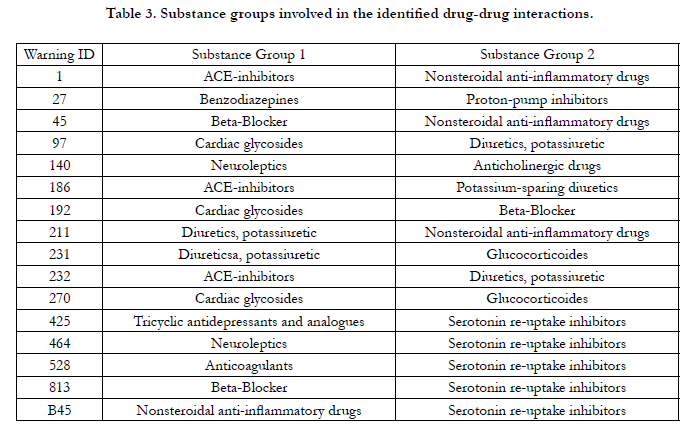
Table 3. Substance groups involved in the identified drug-drug interactions.
Diagnosis T88.7 “Unspecified adverse effect of drug or medicament” was found in 15,437 hospital records. In 19.9% of these cases, the DDI warning “reduced diuretic and antihypertensive efficacy” was available for the combination of the prescribed medication. No other signal was detectable in this group, suggesting that a majority of these diagnoses is a non-specific effect from multiple medicines or caused by a single drug.
The second most frequent diagnosis suggesting drug-drug interaction with 1,332 records was coded as ICD-10 F13.1 “Mental and behavioural disorders due to use of sedatives or hypnotics: Harmful Use”. In this group, available interaction flags included “Increased occurence of severe adverse reactions possible” (39.0%), “Increased plasma concentration of benzodiazepines possible” (28.9%), „Increased gastrointestinal bleeding risk“ (26.6%), ”Intoxication risk – increased efficacy of antidepressants” (20.5%), and “Increased efficacy of benzodiazepines possible” (18.5%).
1,132 cases were found for the third most frequent diagnosis T46.0, “Poisoning by agents primarily affecting the cardiovascular system: Cardiac-stimulant glycosides and drugs of similar action”. Most DDI warnings were “Increased efficacy of cardiac glycosides– risk of cardiac glycoside intoxication (58.3%)”, followed by “Reduced diuretic and antihypertensive efficacy” (36.2%). Of note, the interaction warning “Increased efficacy of cardiac glycosides– risk of cardiac glycoside intoxication” also occurred in a second set of DDI (Table 3) with 196 cases, adding clinical relevance for the association between use of cardiac glycosides, co-medication and hospitalisations.
Other diagnosis were less frequent and included G21.1 “Other drug-induced secondary parkinsonism” (387 cases; most frequent DDI warning “Increased occurence of severe adverse reactions possible” in 40.3%), G44.4 “Drug-induced headache, not elsewhere classified” (298 cases, interaction warning “Increased gastrointestinal bleeding risk” in 34.2%), E16.0 “Drug-induced hypoglycaemia without coma” (296 cases, interaction warning “Reduced glucose-lowering efficacy” in 40.9%, „Increased glucose-lowering efficacy“ in 36.8%), and I95.2 „Drug-induced hypotension“ (282 cases, “Reduced diuretic and antihypertensive efficacy” in 34.4%).
Discussion
It is generally accepted that ADR monitoring can prevent hospital admissions [23]. However, public awareness is limited and underreporting of ADRs is a challenge for implementation of pharmacovigilance surveillance systems. Current legislation addresses primarily reporting and distribution of drug safety information but not analysis of collected data. In addition, discussions about data protection and personalisation of therapies deflect from the usefulness of drug safety databases. A public European database and validated methodology is not available to benchmark regional or national data or to gather information about the incidence or clinical severity of DDIs.
Collected medical and billing data are not popular as a source of pharmacovigilance signal generation. An analysis of healthcare reimbursement information linked with clinical diagnoses may represent a powerful complementary tool to support pharmacovigilance activities. In the present retrospective study the GAPDRG administrative database enabled the analysis of associations between ADR-related hospital discharge diagnosis and preceding medication on a population level. In our cohort, approximately 26% of subjects had a hospitalisation during the observation period, with direct or very likely ADR as a discharge diagnosis in 1.5% of hospitalised subjects.
The present analysis has associated hospitalisations with drug prescriptions preceding the index event. However, due to its dependence on billing data, the study has several limitations. Firstly, the actual intake of medicines cannot be derived from the database information. For this reason, a nominal intake per drug was used. Secondly, the database does not contain over-the-counter drugs, herbal medicines or medication dispensed in hospitals and does not include data from medicines which are not reimbursed such as oral contraceptives. Consequently, DDIs resulting from those substances may have been underreported, even if self-medication may play only a limited role in ADR and DDI leading to hospitalisation [24]. Retrospective drug utilisation reviews show that the incidence of potentially serious DDIs is <1% in ambulatory settings, depending on the case finding methods [25]. In this Austrian cohort, a severe DDI was identified in approximately 12% of hospitalised patients with an ADR-related diagnosis. While this number is small compared to total hospitalisations, it nevertheless indicates a significant and potentially preventable group of ADRs, as flaging of DDIs can be implemented easily as prescription quality check in physician’s electronic drug prescription and pharmacy’s dispense systems. However, in the absence of a control group, the descriptive natur of a DDI does not allow for risk quantification or qualification of the clinical relevance of drug interactions.
The results obtained in this study are difficult to compare with the settings in the various other studies. For example, in Austria the admission diagnoses of hospitalisations are not available as in Germanyand this analysis is limited to discharge diagnoses accordingly. In addition, this limits the causality assessment between the drugs taken before hospitalisation and the ADR diagnoses as a measure of clinical relevance. Nevertheless, the results are similar to other findings, i.e. with regard to the highest risk group of elderly females [12] and the increase of ADR-diagnosis with age. For example, the proportions of ADR-related hospitalisations in 2001 varied between 1.3% for the age group 18-64 years and 2.8% for subjects aged>64 years in the Netherlands [5]. Likewise, the finding that non-steroidal anti-inflammatory drugs are frequently involved DDI is consistent with reviews [26].
The interpretation of DDI warnings with clinical discharge diagnoses is also hampered by the fact that some interactions denote symptoms contrary to the actual clinical presentation, eg., E16.0 drug-induced hypoglycaemia or I95 hypotension. Likewise, the frequent flag for “increased GI bleeding risk” is obvioulsy not an ADR related to the index hospital discharge code F13.1 “Mental disorder due to sedatives or hypnotics”, but confounded by coprescription of serotonin re-uptake inhibitors with non-steroidal anti-inflammatory medicines or antithrombotic drugs. Guidance from automated warning systems for the prescribing physician may therefore result in incorrect clinical expectations or too hesitant dose adjustments. Surprisingly the discharge diagnosis of “Drug-induced headache” (G44.4) was not frequently found in the database. This typical symptom of analgesic medication overuse is commonly observed in chronic pain patients [27], which suggests that some discharge diagnoses may be underreported in the present cohort.
The GAP-DRG database does not provide information on inhospital medication, over-the-counter medicines, or non-reimbursed medications. It is therefore unknown if the clinical course of patients admitted to hospitals is complicated by ADRs from this analysis. Further, other medications, nutrients or products that might interfere with pharmacokinetics or –dynamics of medicines cannot be assessed or risk attributed. The current data does no allow for a comparison of ADR trends over time. The growing importance of this topic is shown by a study in England [4], where an increased rate of ADR admissions as well as in-hospital mortality due to ADR admissions is evident from ten-years trends between 1999 and 2009.
Conclusion
Systematic studies of administrative databases such as GAPDRG can be used to identify ADRs. As recently reported from hospitals in England, USA and Germany, observed differences in the adverse event rates are smaller using routine date than those of other study types [28]. However, the analysis of coded hospital discharge diagnoses does not capture the clinical relevance of drug interactions and cannot be extrapolated to ADRs observed in outpatient care. Additional medical information would be necessary to analyse the severity of DDIs and to avoid hospitalisations early.
Acknowledgments
Financial support for this study was provided by the Main Association of Austrian Social Security Organisations.The auhors wish to thank Mrs. Terraka Jones for her editorial suggestions on preparing the manuscript.
References
- European Medicines Agency (EMA). EMA/186974/2012. New EU pharmacovigilance legislation – Key concepts 2012. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Newsletter/2012/09/WC500132187.pdf
- Muehlberger N, Schneeweiss S, Hasford J (1997) Adverse drug reaction monitoring--cost and benefit considerations. Part I: frequency of adverse drug reactions causing hospital admissions. Pharmacoepidemiology and drug safety 6(3): 71-7.
- Carrasco-Garrido P, de Andres LA, Barrera VH, de Miguel GA, Jimenez- Garcia R (2010) Trends of adverse drug reactions related-hospitalizations in Spain (2001-2006). BMC health services research 10:287.
- Wu TY, Jen MH, Bottle A, Molokhia M, Aylin P, et al. (2010) Ten-year trends in hospital admissions for adverse drug reactions in England 1999- 2009. Journal of the Royal Society of Medicine 103:239-50.
- van der Hooft CS, Sturkenboom MC, van Grootheest K, Kingma HJ, Stricker BH (2006) Adverse drug reaction-related hospitalisations: a nationwide study in The Netherlands. Drug Saf. 29:161-8.
- Hardmeier B, Braunschweig S, Cavallaro M, Roos M, Pauli-Magnus C, et al. (2004) Adverse drug events caused by medication errors in medical inpatients. Swiss medical weekly 134:664-70.
- Schneeweiss S, Hasford J, Gottler M, Hoffmann A, Riethling AK, et al. (2002) Admissions caused by adverse drug events to internal medicine and emergency departments in hospitals: a longitudinal population-based study.European journal of clinical pharmacology. 58:285-91.
- van der Hooft CS, Dieleman JP, Siemes C, Aarnoudse AJ, Verhamme KM, et al. (2008) Adverse drug reaction-related hospitalisations: a population-based cohort study. Pharmacoepidemiology and drug safety. 17:365-71.
- Kongkaew C, Noyce PR, Ashcroft DM (2008) Hospital admissions associated with adverse drug reactions: a systematic review of prospective observational studies. The Annals of pharmacotherapy. 42:1017-25.
- Budnitz DS, Lovegrove MC, Shehab N, Richards CL (2011) Emergency hospitalizations for adverse drug events in older Americans. The New England journal of medicine. 365:2002-12.
- Chan M, Nicklason F, Vial JH (2001) Adverse drug events as a cause of hospital admission in the elderly. Internal medicine journal. 31:199-205.
- Hofer-Dueckelmann C, Prinz E, Beindl W, Szymanski J, Fellhofer G, et al. (2011) Adverse drug reactions (ADRs) associated with hospital admissions - elderly female patients are at highest risk. International journal of clinical pharmacology and therapeutics. 49:577-86.
- Schuler J, Dückelmann C, Beindl W, Prinz E, Michalski T, et al. (2008) Polypharmacy and inappropriate prescribing in elderly internal-medicine patients in Austria. Wiener Klinische Wochenschrift. 120:733-41.
- Perez Menendez-Conde C, Bermejo Vicedo T, Delgado Silveira E, Carretero Accame E (2011) Adverse drug reactions which provoke hospital admission. Farmacia hospitalaria: organo oficial de expresion cientifica de la Sociedad Espanola de Farmacia Hospitalaria. 35:236-43.
- Pirmohamed M, James S, Meakin S, Green C, Scott AK, et al. (2004) Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ (Clinical research ed). 329:15-9.
- Rottenkolber D, Hasford J, Stausberg J (2012) Costs of adverse drug events in German hospitals--a microcosting study. Value in health : the journal of the International Society for Pharmacoeconomics and Outcomes Research. 15:868-75.
- Sultana J, Cutroneo P, Trifiro G (2013) Clinical and economic burden of adverse drug reactions. Journal of pharmacology & pharmacotherapeutics. 4(Suppl1):S73-S7.
- Srba J, Descikova V, Vlcek J (2012) Adverse drug reactions: analysis of spontaneous reporting system in Europe in 2007-2009. European journal of clinical pharmacology. 68:1057-63.
- (2012) AGES Medizinmarktaufsicht. Arzneimittelsicherheit: Erstmeldungen von Angehörigen der Gesundheitsberufe: Bundesamt für Sicherheit im Gesundheitswesen (BASG). http://www.basg.gv.at/news-center/statistiken/arzneimittelsicherheit/.
- Stausberg J, Hasford J (2010) Identification of Adverse Drug Events: The Use of ICD-10 Coded Diagnoses in Routine Hospital Data. Dtsch Arztebl International. 107:23-9.
- (2013) Apotheker-Verlag. Austra-Codex. http://www3.apoverlag.at/dynasite.cfm?dsmid=106234.
- (2012) Statistik Austria. Jahresdurchschnittsbevölkerung seit 2002 nach fünfjährigen Altersgruppen und Geschlecht. Available from: http://www.statistik.at/web_de/statistiken/bevoelkerung/bevoelkerungsstruktur/bevoelkerung_nach_alter_geschlecht/023427.html.
- Goettler M, Schneeweiss S, Hasford J (1997) Adverse drug reaction monitoring--cost and benefit considerations. Part II: cost and preventability of adverse drug reactions leading to hospital admission. Pharmacoepidemiology and drug safety. 6(3):S79-90.
- Schmiedl S, Rottenkolber M, Hasford J, Rottenkolber D, Farker K, et al. (2014) Self-medication with over-the-counter and prescribed drugs causing adverse-drug-reaction-related hospital admissions: results of a prospective, long-term multi-centre study. Drug Saf. 37(4):225-35.
- Peng CC, Glassman PA, Marks IR, Fowler C, Castiglione B, et al. (2003) Retrospective drug utilization review: incidence of clinically relevant potential drug-drug interactions in a large ambulatory population. Journal of managed care pharmacy 9:513-22.
- Dechanont S, Maphanta S, Butthum B, Kongkaew C (2014) Hospital admissions/ visits associated with drug-drug interactions: a systematic review and meta-analysis. Pharmacoepidemiol Drug Saf. 23:489-97.
- Colas R, Munoz P, Temprano R, Gomez C, Pascual J (2004) Chronic daily headache with analgesic overuse: epidemiology and impact on quality of life. Neurology. 62:1338-42.
- Stausberg J (2014) International prevalence of adverse drug events in hospitals: an analysis of routine data from England, Germany, and the USA. BMC health services research. 14:125.





