Gender based Dosing of Metoprolol in the Elderly using Population Pharmacokinetic Modeling and Simulations
Eugene AR1,2
1 Division of Clinical Pharmacology, Department of Molecular Pharmacology and Experimental Therapeutics, Gonda 19, Mayo Clinic, 200 First Street SW, Rochester, MN 55905, USA.
2 Joyner Lab: Integrative Human Physiology and Pharmacology Lab, Department of Anesthesiology, Rochester, MN, USA.
*Corresponding Author
Andy R. Eugene, MD,
Division of Clinical Pharmacology, Department of Molecular Pharmacology and Experimental Therapeutics, Gonda 19, Mayo Clinic, 200 First Street SW, Rochester, MN 55905, USA.
Tel: +1-507-284-2790
Fax: +1-507-284-4455
E-mail:eugene.andy@mayo.edu
Article Type: Research Article
Received: April 12, 2016; Accepted: May 17, 2016; Published: May 19, 2016
Citation: Eugene AR (2016) Gender based Dosing of Metoprolol in the Elderly using Population Pharmacokinetic Modeling and Simulations. Int J Clin Pharmacol Toxicol. 5(3), 209-215. DOI : dx.doi.org/10.19070/2167-910X-1600035
Copyright: Eugene AR© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: This article seeks to clarify if gender-based differences occur in the pharmacokinetics of metoprolol in the elderly patients. There are a series of physiologic changes that occur in the elderly ranging from decreased hepatic blood flow to increased adiposity causing higher plasma concentrations at therapeutic doses as compared to the healthy young population.
Methods: Population pharmacokinetic modeling were performed using MONOLIX and Monte-Carlo simulations were conducted using MATLAB. The data was based from a previously published dataset where elderly patients, having multiple comorbidities, were administered a 50mg dose of metoprolol.
Results: Metoprolol was modeled using a one-compartment model and resulted in the following population pharmacokinetic parameters: volume of distribution, V=38L (CV=155%), clearance rates, CL-Men=105L/hour and CL-Women=59.1L/hour (38%), time lag, Tlag=0.469 hour (CV=17%), and the absorption rate constant, Ka=0.235 hr-1 (CV=23%).
Conclusion: Gender stratified doses resulting in an equivalent systemic metoprolol exposure in geriatric patients have been identified.Metoprolol doses resulting a similar AUC in a healthy young male administered 50mg tablet were 15mg for geriatric women and 25mg for geriatric men. Further, Metoprolol doses of 25mg for geriatric women and 50mg for geriatric men resulted in an equivalent AUC to a healthy young males dosed with a 100mg tablet. A 15mg Metoprolol tablet may need to be compounded to account for the gender differences in Metoprolol pharmacokinetics.
2.Introduction
3.Methods
3.1.Dataset
3.2.Population Pharmacokinetic Modeling and Simulations
3.3.Dose-Finding Monte-Carlo Simulations
4.Results
4.1.Population Pharmacokinetics
4.2.Monte-Carlo Simulations
5.Discussion
5.1.Potential Effects on Systolic Blood Pressure and Heart Rate
6.Conclusion
7.Acknowledgement
8.References
Keywords
Metoprolol; Gender; Geriatrics; Population Pharmacokinetics; Monolix; Dose.
Introduction
This article seeks to clarify if gender based dosing of the cardioselective beta-blocker metoprolol is warranted in the elderly. Metoprolol is a β1-adrenergic receptor blocker that was first synthesized in 1969 [1]. Therapeutically, Metoprolol serves a wide array of indications as well as a series of off-label uses. Based on its cardiac selectivity, metoprolol, has been successfully included in a series of cardiovascular management guidelines. According to the American College of Cardiology Foundation (ACCF) and the American Heart Association (AHA) 2013 guideline recommendations, metoprolol, as a beta-blocker option, may be used for the management of ST-elevation myocardial infarction (STEMI) or unstable angina/non-STEMI [2]. Further, the ACCF/AHA guidelines state thatoral beta-blockers should be initiated within the first 24-hours, of the aforementioned conditions, unless a patient presents with contraindication such as: signs of heart failure, a low-output state, at risk for cardiogenic shock, or other contraindications. In the case of administration using the intravenous formulation of metoprolol, clinical management with the intravenous form is indicated if patients present with refractory hypertension or has ongoing ischemia [2,3].
In the case of hypertension, the American Heart Association, American College of Cardiology and American Society of Hypertension (AHA/ACC/ASH) 2015 scientific statement, recommends using a beta blocker, which may be metoprolol, as part of the treatment regimen of patients diagnosed with hypertension and chronic stable angina who have a history of prior myocardial infarction (MI) [4]. In terms of the prevalence among patients in the U.S., the Intercontinental Marketing Services (IMS) Institute for Healthcare Informatics report on Medicines Use and Spending Shifts shows that there has been a steady increase in the dispensed metoprolol prescriptions with 76.6 million dispensed in 2010 and increased each year to 85.3 million metoprolol dispenses in 2014 [5].
A recent, June 2015, National Institutes of Health (NIH) Office of Research on Women's Health (ORWH) guide notice titled, "Consideration of Sex as a Biological Variable in NIH-funded Research," gender will play a major role in the reporting of NIHfunded research studies going forward [6]. Thus, research studies in physiology, pharmacology, geriatrics, and more may utilize metoprolol and will have to report results on sex/gender differences, potentially resulting in unexpectedresults affecting clinical and basic science research. So, do the pharmacokinetics in elderly men and women differ when being administered the equivalent doses of metoprolol? If so, what are the optimal doses resulting in similar plasma concentration-time profiles in elderly men and women?.
Based on metoprolol tartrate’s package insert, clinicians are recommended to start a low starting dose in geriatric patients (>65-years-old) due to comorbidities, an increased prevalence of reduced organ function (i.e. liver, kidneys, and heart) and concurrent use of other drugs. However, based on the package insert no dose adjustment is recommended, even though a slight increase in the plasma concentrations is evident [7].
The aim of this population pharmacokinetic analysis is to consider gender as a variable using an existing published dataset to then quantify the metoprolol dose in elderly men and women resulting in anequivalent total metoprolol drug exposure (AUC) as found in the young healthy study participants.
Methods
Metoprolol plasma samples are based from digitizeddata-points from the Lundborg and colleagues study conducted at the University of Goteborg in Sweden and published in 1976 [8]. The original study included twelvechronically-ill geriatric inpatients with multiple comorbidities. From the original twelve patients, ten were administered a single 50mg oral dose of Metoprolol followed by 100 mL of water [8]. All patients were in a fasted state, for a minimum of 10-hours prior to the pharmacokinetic study which began at 7:30am [8].
Nonlinear mixed effects modeling of the concentration-time data were performed using the MONOLIX (MOdèlesNOnLInéaires à effetsmiXtes) software package version 4.3.3. The MONOLIX software has been designed for model-based drug development and uses the Stochastic Approximation Expectation-Maximization (SAEM) algorithm with a Markov ChainMonte-Carlo (MCMC) procedure to compute the maximum likelihood estimates of the population estimates and the respective variances [9-13]. Model selection was based in a stepwise fashion using the forward inclusion and subsequent backward elimination step reaching the lowest -2 x Log-likelihood estimate and goodnessof-fit plots. Throughout the model selection, the tested covariates included body weight (kg) and gender for the absorption rate constant (Ka), clearance rate (CL), volume of distribution (V), and time lag (Tlag). Model validation was computed using the prediction-corrected Visual Predictive Check (VPC).
Following computing of the population pharmacokinetic parameters, model-based simulations were conducted using the A4S PK/PD Simulator that runs in the MATLAB programming environment [14]. For each stochastic simulation scenario, 5000 virtual patients were simulated using 400 plasma sampling points with Metoprolol dosed every 12-hours over the course of 24-hours to simulate clinical prescription instructions provided to patients. The Monte-Carlo simulations are stratified by gender and age demographic to illustrate the wide variability of the expected plasma levels for the drug. Subsequent dose-finding model-based simulation runswere focused on identifying the equivalent total drug exposure that is measured as the area under the concentration-time curve (AUC). Based on an equivalent AUC, gender based dosing calculations identified using the AUC and maximum concentration (Cmax) from healthy young CYP2D6 Extensive Metabolizers as referenced from final population pharmacokinetic model parameters published from the Kalia and colleagues [15].
Results
The analysis included a total of seven patients (females: n=3, males=4) from the original ten study participants receiving the 50mg dose. The age ranged from 61 to 88 years with a population mean ± SD of 75 ± 9 years (males: 65 ± 6 years; females: 83 ± 13 years). The body weight ranged from 45 to75 kilograms with a population mean ± SD of 62kg ± 10kg (males: 65 ± 6kg; females: 58 ± 13kg). To adequately account for the low sample size, the final population model was compared to metoprolol population pharmacokinetic model parameter estimates from the Kaila and colleagues 2007 publication that studied 35 healthy males, the Luzierand colleagues 1999 article, which studied 10 healthy males and 10 healthy women, and finally the Taguchi and colleagues 1994 article that studied the effect of the CYP2D6 polymorphic alleles in forty-four patients between the ages of 56 and 83 years old [15-17]. The model comparisons are provided in the discussion section of this paper.
To be consistent with the previous population pharmacokinetic model of metoprolol, a one-compartment model with first-order elimination and first-order absorption was chosen and adequately described the dataset [15]. The log-likelihood was estimated by the linearization method and the final model resulted in a -2 x Log-Likelihood (-2xLL) of 592.59 and an Akaike Information Criteria (AIC) of 612.59. The results of the final population pharmacokinetic parameter estimates are shown in Table 1.
Figure 1 displays the model diagnostics of the observed versus predicted goodness-of-fit plots for the population and individual metoprolol plasma concentrationpredictions. Further model evaluation was based on the normalized prediction distribution error plot and the individual weighted residual plots shown in Figure 2. The overall final diagnostic plot, the visual predictive check (VPC), is displayed in Figure 3 for the population.
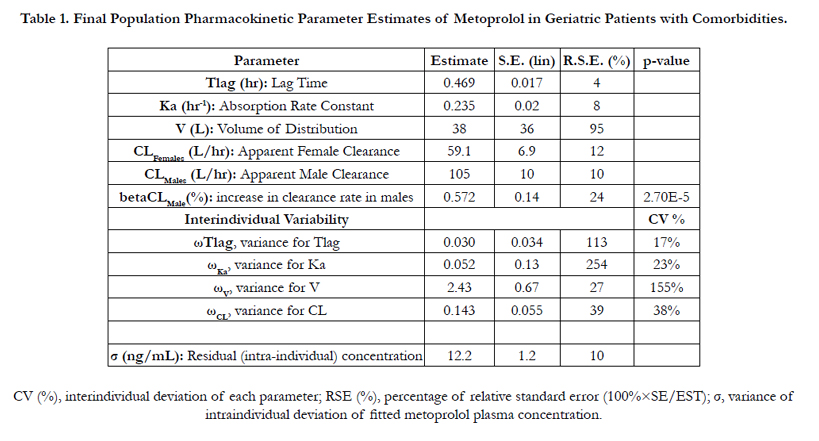

Table 1. Final Population Pharmacokinetic Parameter Estimates of Metoprolol in Geriatric Patients with Comorbidities.
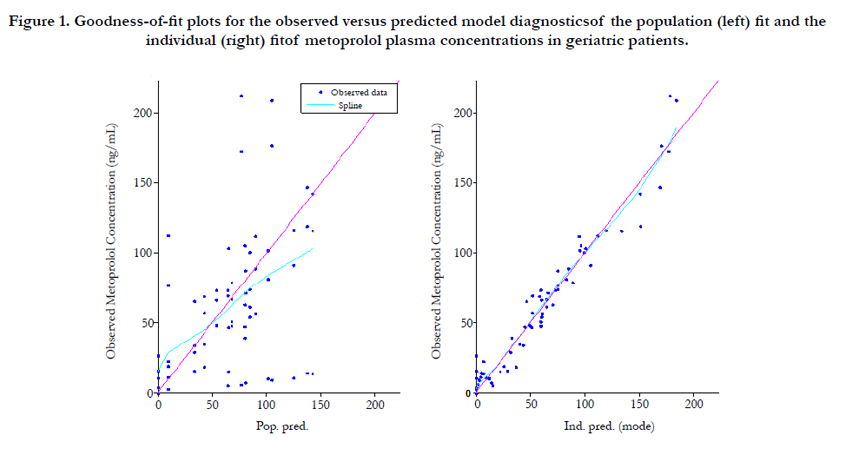
Figure 1. Goodness-of-fit plots for the observed versus predicted model diagnosticsof the population (left) fit and the individual (right) fitof metoprolol plasma concentrations in geriatric patients.
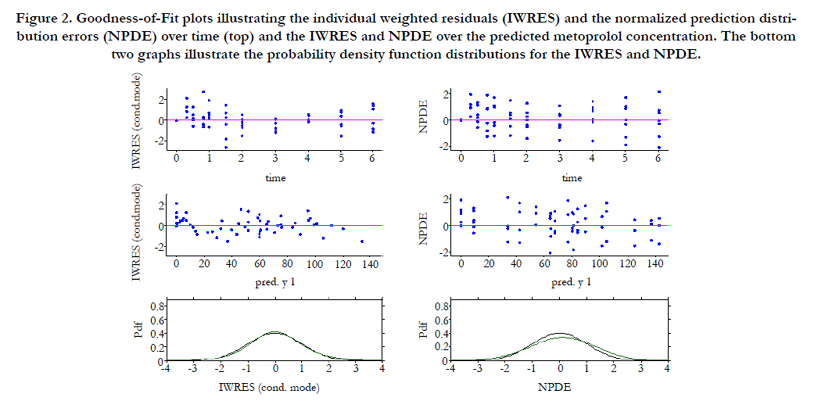
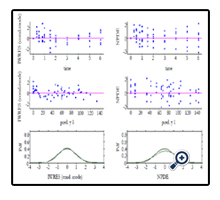
Figure 2. Goodness-of-Fit plots illustrating the individual weighted residuals (IWRES) and the normalized prediction distribution errors (NPDE) over time (top) and the IWRES and NPDE over the predicted metoprolol concentration. The bottom two graphs illustrate the probability density function distributions for the IWRES and NPDE.
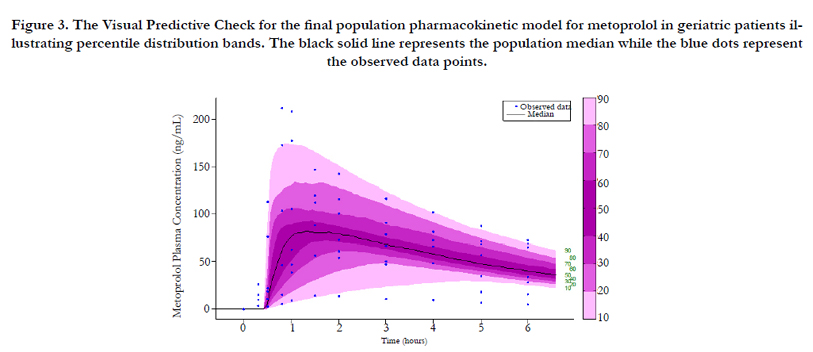
Figure 3. The Visual Predictive Check for the final population pharmacokinetic model for metoprolol in geriatric patients illustrating percentile distribution bands. The black solid line represents the population median while the blue dots represent the observed data points.
As for guidance in dosing geriatric patients, as previously stated, the metoprolol package insert recommends that clinicians start with a low dose in the elderly patients with no quantitative value being recommended [7]. Clearly, with five dosing formulations (25mg, 50mg, 100mg, and 200mg) available most physicians would choose 25mg or 50mg in elderly patients. However, being that the clearance rates between elderly men and women have a 57% difference no guidance on gender based dosing is currently available. Further, with geriatric females having lower clearance rates than in healthy CYP2D6 Poor Metabolizers, and realizing thatthe Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines from the Royal Dutch Association for the Advancement of Pharmacy's Pharmacogenetics Working Group recommends a 75% dose reduction for metoprolol in patients defined as poor metabolizers [18], a hypothesis would be that a 75% reduction in the elderly patients may be a reasonable starting dose.
To test this hypothesis, Monte-Carlo simulations will be conductedusing the area under the concentration-time curve (AUC) in healthy male extensive metabolizers as benchmark for the total drug exposure with the aim of identifying doses for both elderly men and women resulting in equivalentdrug exposures for metoprolol. The reasoning for this is to minimize any potentialsideeffects of prolonged beta-blockade in frail elderly patients that may result in excessive sympathetic modulation at the adrenergic receptors.
The Monte-Carlo simulation results for metoprolol doses resulting in an approximately equivalent total drug exposure are provided in Table 3. Based on these findings a 15mg tablet would provide the best single dose for elderly females, but this current dose strength is not available for purchase. For elderly males, the 25mg dose would result in similar system exposures as found in healthy young males taking a 50mg tablet. To illustrate the differences in plasma levels, alternative dosing strengths were simulated to identify an approximately similar area under the concentrationtime curve as found in young males administered either a 50mg tablet or 100mg tablet. In this instance that a 15mg tablet would not be manufactured for purchase, a 25mg table for elderly females would potentially be the best alternative option, and is currently available.
Discussion
This paper quantified the gender differences in the pharmacokinetics of metoprolol in elderly patients having multiple comorbidities. The only significant covariate found in the popPK model was gender and the addition of body weight increased the AIC, and thus reduced the biological plausibility of the parameters. Therefore, the reduced model stratifying the clearance rate based on gender was chosen and resulted in a 57% decrease in clearance rate in female geriatric patients as compared to males of similar age and health status.
The metoprolol model comparisons are shown in Table 2. Based on the three publication references, the key parameter of interests is the clearance rates between groups. The Kaila and colleagues 2007 publication showed that the clearance rates of CYP2D6 Poor Metabolizers (PM) and Extensive Metabolizers (EM) of metoprolol were similar to the findings in this paper’s predictions for elderly female and elderly males, respectively [15]. Even though the Taguchi and colleagues article would have been an excellent comparison, due to the inclusion of the elderly population, the group chose a one-compartment model with repetitive bolus dosing and later commented that approximation errors may be due to their selection of the bolus model to describe the population pharmacokinetic distribution of time [17]. Furthermore, Taguchi and colleagues stated that the pharmacokinetics of metoprolol in Japanese patients classified as having CYP2D6 Extensive Metabolizers are different from Extensive Metabolizers in the Caucasian population and attributed the findings to large interethnic differences in the CYP2D6*10 gene frequency [17]. So, to evaluate the frequency of normal versus slow hepatic metabolism rates of CYP2D6 among ethnicities, the Bradford 2002 article was reviewing the gene frequency among populations was identified [19].
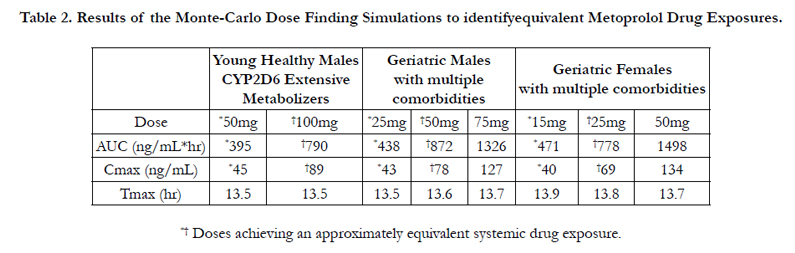
Table 2. Results of the Monte-Carlo Dose Finding Simulations to identifyequivalent Metoprolol Drug Exposures.
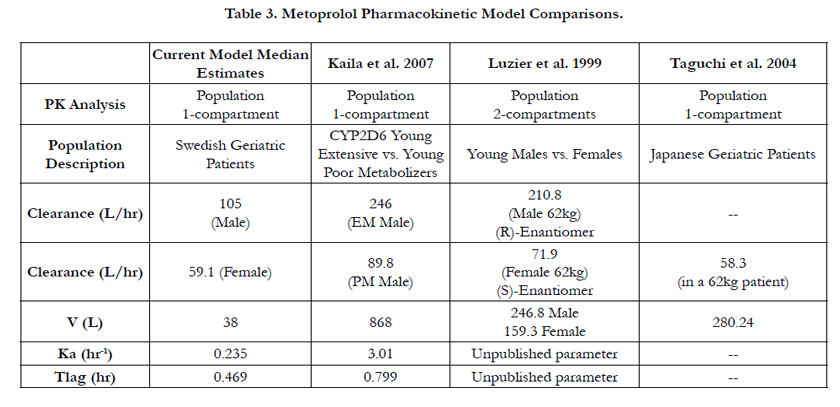
Table 3. Metoprolol Pharmacokinetic Model Comparisons.

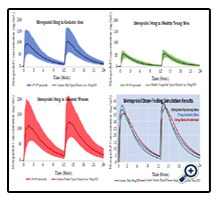
Figure 4. Monte-Carlo simulation results illustrating Metoprolol pharmacokinetic profiles for 5000 virtual patients and dose-finding simulation results identifyingequivalent systemic drug exposures measured as area under the concentrationtime curve.
Bradford summarized that CYP2D6 allele frequencies among the various racial/ethnic groups showed that European Caucasians had a 26% prevalence of non-functional alleles, while Africans and African Americans had a 35% reduced function alleles. Lastly, the article stated that Asians and Pacific Islanders had a 41% median prevalence of the reduced function allele, indicating a slower metabolism [19]. Thus, the findings in Table 2, showing that the Taguchi and colleagues popPK analysis in the Japanese patients resulted in the slowest clearance rate, is consistent with the findings from Bradford’s findings.
Further, based on the popPK model parameters by the Taguchi and colleagues paper, pharmacokinetic simulation results show that a 20mg dose results in an AUC of 341mcg*hr/L in24-hours, allowing for 65mcg*hr/L less than young male CYP2D6 extensive metabolizers. Further, a 25mg dosing simulation results in a total drug exposure of 426mcg*hr/L in 24-hours; only 20mcg*hr/L greater than healthy extensive metabolizers in 24-hours. Thus, based on these mathematical simulations, the 25mg metoprolol tablet is results in reasonably similar metoprolol exposure for the elderly Japanese patients as compared to the healthy young male CYP2D6 population from the parameters by Kaila et al. [15].
Using the metoprolol pharmacodynamic parameters reported from the Luzier et al publication, the maximum reduction (Emax) in systolic blood pressure (SBP) and heart rate (HR) are 18% (CV%˜20%) and 30% (CV˜10%), respectively [16]. The Hill constant (γ) creating the sigmoidal behavior of the concentrationeffect curves are SBP: γ-men=6.15 and γ-women=2.45 for HR:γ- men=1.1 and γ-women=1.3 [16]. Moreover, the metoprolol plasma concentrations resulting in a 50% reduction (EC50) in SBP and HR are reported as SBP: men=28ng/mL and women=25ng/mL and for HR: men=15ng/mL and women=21ng/mL [16]. Physiologically, 25-28ng/mL will reduce the SBP by approximately 10% from baseline levels and similarly, this same plasma range will a decrease a patient’s HR by greater than 15% from baseline levels. Based on these reported pharmacodynamic values from healthy young male and female study participants and using the new dose findings calculated in this paper, a geriatric patient with a SBP of 160mmHg and resting HR of 100beats/minute dosed at 15mg for geriatric females and 25mg for geriatric males would result in approximate new SBP of 144mmHg and HR of 85beats/minute. Otherwise, using 25mg (Cmax ˜ 70ng/mL) in an elderly woman would drop her a baseline SBP of 160mmHg to ˜130mmHg and HR from 100beats/minute to 70beats/minute. It is quite possible that such wide fluctuations in the daily blood pressure by 30mmHg throughout the day may unnecessarily modulate the autonomic nervous system resulting in potential complications. Further, since most elderly are taking more than one prescription medication, there is a possibility that one’s patient is taking a drug that is an inhibitor of CYP2D6 (e.g. paroxetine) which may further increases the plasma levels of metoprolol that is metabolized by the same cytochrome P450 pathway [20]. Lastly, due to the high lipophilic nature of metoprolol resulting in its ability to cross the blood-brain-barrier, avoidance in high plasma levels may improve the quality of life and activities of daily living in elderly patients.
From the original Lundborg 1976 publication, the maximal reduction in systolic blood pressure in was 30 ± 10 mmHg and the average reduction of heart rate was 19 ± 3 beats per minute following the 50mg metoprolol dose [8]. The Luzier et al article evaluating the gender differences of metoprolol pharmacokinetics and pharmacodynamics (heart rate and systolic blood pressure), showed similar clearance rates from the current population pharmacokinetic results to the calculations in this analysis [16].
Conclusion
Based from the population pharmacokinetic modeling and Monte-Carlo simulations, indeed gender differences in metoprolol exists in geriatric patients. Based from the findings, gender stratified doses for metoprolol yielding relatively similar systemic drug exposures were calculated to be 15mg for geriatric women and 25mg for geriatric men resulting in that found in healthy young males administered a 50mg dose. The consideration for compounding a 15mg tablet of metoprolol would lead to avoiding the unnecessary high systemic drug exposures in geriatric women and account for the gender differences in the pharmacokinetics of metoprolol. For the elderly males, the 25mg tablet already exists and therefore therapeutic drug management would proceed as best seen by the prescribing clinicians.
Acknowledgement
The author declares no conflict of interests. Research reported in this publication was supported by National Institute of General Medical Sciences of the National Institutes of Health under award number T32 GM008685. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
- B. Carlsson (1997) Technological Systems and Industrial Dynamics. (1stedn), Springer Science & Business Media, New York.10: 1-329.
- O’Gara PT, Kushner FG, Ascheim DD, Casey DE, Chung MK, de Lemos JA, et al. (2013) 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 61(4): e78–140.
- Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, et al. (2007) ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise th. J Am Coll Cardiol 50(7): e1–157. doi:10.1016/j.jacc.2007.02.013.
- Rosendorff C, Lackland DT, Allison M, Aronow WS, Black HR, Blumenthal RS, et al. (2015) Treatment of hypertension in patients with coronary artery disease: a scientific statement from the American Heart Association, American College of Cardiology, and American Society of Hypertension. Hypertension 65(6): 1372–1407.
- IMS Health. Medicines Use and Spending Shifts: A Review of the Use of Medicines in the U.S. in 2014. IMS Inst Healthc Informatics 2015.
- National Institutes of Health. NOT-OD-15-102: Consideration of Sex as a Biological Variable in NIH-funded Research 2015.
- Novartis Pharmaceuticals Corporation. DailyMed - LOPRESSOR- metoprolol tartrate tablet 2012.
- Lundborg P, Steen B (1976) Plasma levels and effect on heart rate and blood pressure of metoprolol after acute oral administration in 12 geriatric patients. Acta Med Scand 200(5): 397–402.
- Savic RM, Mentré F, Lavielle M (2011) Implementation and evaluation of the SAEM algorithm for longitudinal ordered categorical data with an illustration in pharmacokinetics-pharmacodynamics. AAPS J 13(1): 44–53. doi:10.1208/s12248-010-9238-5.
- Kuhn E, Lavielle M (2005) Maximum likelihood estimation in nonlinear mixed effects models. Comput Stat Data Anal 49(4): 1020–1038. doi:10.1016/j.csda.2004.07.002.
- Savic R, Lavielle M (2009) Performance in population models for count data, part II: A new SAEM algorithm. J Pharmacokinet Pharmacodyn 36(4): 367–379. doi:10.1007/s10928-009-9127-7.
- Delyon B, Lavielle M, Moulines E (1999) Convergence of a stochastic approximation version of the EM algorithm. Ann Stat 27(1): 94–128. doi:10.2307/120120.
- Samson A, Lavielle M, Mentré F (2007) The SAEM algorithm for group comparison tests in longitudinal data analysis based on non-linear mixedeffects model. Stat. Med 26(27): 4860–4875. doi:10.1002/sim.2950.
- Germani M, Del Bene F, Rocchetti M, Van Der Graaf PH (2013) A4S: a user- friendly graphical tool for pharmacokinetic and pharmacodynamic (PK/PD) simulation. Comput Methods Programs Biomed 110(2): 203–214. doi:10.1016/j.cmpb.2012.10.006.
- Kaila N, Straka RJ, Brundage RC (2007) Mixture models and subpopulation classification: a pharmacokinetic simulation study and application to metoprolol CYP2D6 phenotype. J Pharmacokinet Pharmacodyn 34(2): 141–156. doi:10.1007/s10928-006-9038-9.
- Luzier AB, Killian A, Wilton JH, Wilson MF, Forrest A, et al. (1999) Gender- related effects on metoprolol pharmacokinetics and pharmacodynamics in healthy volunteers. Clin Pharmacol Ther 66(6): 594–601. doi:10.1053/cp.1999.v66.103400001.
- Taguchi M, Nozawa T, Mizumaki K, Inoue H, Tahara K, et al. (2004) Nonlinear mixed effects model analysis of the pharmacokinetics of metoprolol in routinely treated Japanese patients. Biol Pharm Bull 27(10): 1642–1648. doi:10.1248/bpb.27.1642.
- Swen JJ, Nijenhuis M, de Boer A, Grandia L, Maitland-van der Zee a H, et al. ( 2011) Pharmacogenetics: from bench to byte--an update of guidelines. Clin Pharmacol Ther 89(5): 662–673. doi:10.1038/clpt.2011.34.
- Bradford LD (2002) CYP2D6 allele frequency in European Caucasians, Asians, Africans and their descendants. Pharmacogenomics 3(2): 229–243. doi:10.1517/14622416.3.2.229.
- Parker RB, Soberman JE (2011) Effects of paroxetine on the pharmacokinetics and pharmacodynamics of immediate-release and extended-release metoprolol. Pharmacotherapy 31(7): 630–641. doi: 10.1592/phco.31.7.630.





