Evaluation of the Cytotoxic Effects of Combined Application of Methotrexate and Statins on Green Monkey Kidney Cells
M. Izdebska*, I. Piątkowska-Chmiel, M. Herbet, M. Gawrońska-Grzywacz, D. Natorska-Chomicka
Department of Toxicology, Medical University of Lublin, Poland.
*Corresponding Author
Magdalena Izdebska,
Department of Toxicology, Medical University of Lublin,
Chodzki 8, 20-093 Lublin, Poland.
Tel/Fax: +48 814487400
E-mail: magdalena.izdebska@umlub.pl
Article Type : Research Article
Received: August 04, 2015; Accepted: September 30, 2015; Published: October 05, 2015
Citation: M. Izdebska, I. Piątkowska-Chmiel, M. Herbet, M. Gawrońska-Grzywacz, D. Natorska-Chomicka (2015) Evaluation of the Cytotoxic Effects of Combined Application of Methotrexate and Statins on Green Monkey Kidney Cells. Int J Clin Pharmacol Toxicol, 4(5) 185-191. doi: dx.doi.org/10.19070/2167-910X-1500031.
Copyright: M. Izdebska© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Lipid disorders that lead to cardiovascular diseases are also common with oncology patients. Therefore, this group of patients is exposed to the risk of interaction between the cytostatic drugs applied and statins. Methotrexate is widely used in cancer treatment. However, it is a highly toxic drug. Nephrotoxicity is the most common side effect following the methotrexate therapy. On the other hand, statins are reported to have possible renoprotective effects against drug-induced nephrotoxicity. The aim of this study was to evaluate the cytotoxic effects of the combined application of methotrexate and statins (atorvastatin, rosuvastatin or pravastatin) on the green monkey kidney cells (GMK), using the MTT and LDH assays. The effect of these drugs and their combination on the GMK cells apoptosis was also evaluated using the Cell Death Detection ELISA kit. The results obtained from the cytotoxicity assays suggest an adverse effect of the combined application of methotrexate (5.5 or 16.5 μM) and atorvastatin (100 μM) on the viability of GMK cells. A decrease in the cell viability in this case was attributed to apoptosis. In the study, a significant reduction in the GMK cell viability was also identified in the MTT assay after 24h of incubation with methotrexate in combination with rosuvastatin or pravastatin. However, in the LDH assay, there were no significant changes that clearly indicate the intensification of their cytotoxic effects. The obtained results, especially in the MTT test, demonstrate a negative influence of the combined application of methotrexate and statins on the viability of GMK cells.
2.Introduction
3.Materials and Methods
3.1.Drugs and reagents
3.2.Cell culture
3.3.MTT viability assay
3.4.LDH assay
3.5.Assessment of apoptosis
3.6.Statistical analysis
4.Results
4.1.The effects of MTX, statins and their combinations on the viability of GMK cells in the MTT test
4.2.Cytotoxicity of MTX, statins and their combinations on GMK cells in LDH test
4.3.Effects of MTX, statins and their combinations on the GMK cells apoptosis
5.Discussion
6.Conclusion
6.Acknowledgment and Declaration
7.References
Keywords
Methotrexate; Statins; MTT Assay; LDH Assay; Apoptosis.
Introduction
Today’s pharmacotherapy of diseases connected with the dynamic civilization development, such as cancer, atherosclerosis and hypertension, faces a very serious problem. The key issue in patient treatment is the appropriate choice of drugs for the individual disease. Such drugs should not only lead to satisfactory therapeutic results, but also be free from negative mutual interaction. Such an interaction between the applied drugs can influence the treatment duration as well as, in some cases, threatening the patient’s health. Patients with cancer represent a special risk group with regard to drug-drug interactions because they are usually administered other drugs during their treatment, which is likely to eventuate in often rather unpredictable interactions. In addition, the majority of cancer patients are over 65-year-olders with age-related changes in the hepatic and renal functions – this poses even a greater risk drug-drug interactions [1]. Methotrexate (MTX), the focus of this study, is a cytostatic, antimetabolite, folic acid antagonist used in cancer treatment [2]. In small doses, it reveals anti-inflammatory and immunosuppressive activity. Thanks to its properties, it finds application in the treatment of inflammatory and autoimmune diseases, such as rheumatoid arthritis or psoriasis [3-5]. MTX is an inhibitor of dihydrofolate reductase (DHFR), a key enzyme in intracellular folate metabolism. DHFR catalyses the conversion of folic acid into tetrahydrofolate. As a consequence of DHFR inhibition, the intracellular level of tetrahydrofolate coenzymes is decreased, resulting in the inhibition of thymidylate, purine and, consequently, in the DNA biosynthesis. MTX inhibits cell replication, specifically on the S-phase of the cell cycle. Unfortunately, MTX is a highly toxic drug [3, 6]. Patients need to be monitored throughout the treatment, in particular their renal and liver functions. Kidneys are the major route of MTX elimination. The renal dysfunction after MTX treatment is a clinically important side effect, especially if the drug is administrated in high doses. The long-lasting MTX therapy can also cause the permanent impairment of kidney functions, thus slowing down the drug elimination from the body and an increase in its toxicity. Acute renal failure is the result of intratubular precipitation of the drug crystals in acidic pH of urine [7-9]. But this is not the only cause of methotrexate-induced nephrotoxicity. The pathogenesis of this process is also associated with oxidative stress and inflammation.
Morsy et al. [10] reported that MTX increases the concentrations of renal malondialdehyde (an indicator of renal lipid peroxidation) and nitrite/nitrate (an indicator of renal nitric oxide level). MTX also significantly reduced the renal glutathione peroxidase and superoxide dismutase activities while increasing the renal tumour necrosis factor α (TNFα), compared with the control group. MTX can inhibit NADP malic enzymes, and this could decrease the availability of NADPH in cells. NADPH is known to be a cofactor of glutathione reductase (GR) – the enzyme responsible for maintaining the level of reduced glutathione (GSH) [11]. Presently, a large part of the population suffers from arteriosclerosis and hypertension. Therefore, in cancer patients especially of mature age, there is a risk of interaction between cytostatic drugs and statins (lipid-lowering drugs). Statins are a group of drugs whose mechanism of action is based on the inhibition of 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase, the enzyme responsible for cholesterol production [12]. Statins have many pleiotropic effects, including improved endothelial function, reduced and stabilized atheromatous plaques, and anti- inflammatory and antioxidative activities [13, 14]. Statins also have potential anti-cancer properties. They inhibit cell growth and diminish the tumour cell viability. In addition, statins inhibit DNA synthesis and selectively induce apoptosis in the cell lines of human tumours [15-17]. In their study, Kabel et al. [18] demonstrated that the administration of a combination of MTX and atorvastatin to mice with solid Ehrlich carcinoma resulted in a significant decrease in the tumour volume compared with the group that received MTX or atorvastatin alone. Statins also show some renoprotective activities against drug-induced nephrotoxicity (especially antioxidant and anti-inflammatory effects) [19]. The combined use of MTX and statins may be beneficial for the patient in terms of the effectiveness of polytherapy, but can also amplify side effects of these drugs. Treatment with statins is associated with the risk of side effects affecting mainly the liver and muscles (such as myopathy and rhabdomyolysis) [20, 21]. Rhabdomyolysis can cause acute renal failure. Statins are the most commonly prescribed drugs, but unfortunately are likely to interact with other drugs [22]. Our previous study on green monkey kidney cells demonstrated a potentiation of the cytotoxic effects of MTX in combination with simvastatin, both in the MTT as well as LDH assay [23]. These results prove the necessity of further study concerning the in vitro evaluation of interaction between MTX and commonly used statins (atorvastatin, rosuvastatin or pravastatin).
Materials and Methods
The following substances were used in the study: methotrexate (Ebewe Pharma, Unterach, Austria), atorvastatin (Pfizer Europe, United Kingdom), rosuvastatin (Astra Zeneca, Schweden), pravastatin (Ranbaxy, Poland), MTT (Thiazolyl blue tetrazolium bromide, Sigma-Aldrich, Steinheim, Germany), DMSO (dimethyl sulfoxide, POCH S.A. Gliwice, Poland). The cell culture medium RPMI-1640 (with L-glutamine and phenol red), Foetal Bovine Serum (FBS) and antibiotics solutions: penicillin, streptomycin, and amphotericin B were supplied by PAA – The Cell Culture Company GmbH, Pasching, Austria. Ready-made diagnostic kits (Cytotoxicity Detection Kit LDH and Cell Death Detection ELISAPLUS from Roche Diagnostic GmbH, Mannheim, Germany) were used. Atorvastatin, rosuvastatin and pravastatin were dissolved in DMSO and diluted to the required concentration with the RPMI- 1640 medium. The solutions of methotrexate were ex tempore prepared in the culture medium.
The research was performed on green monkey kidney cells (GMK) obtained from Biomed Serum and Vaccine Production Plant Ltd in Lublin, Poland. A GMK cell line was grown in RPMI-1640 medium (with L-glutamine and phenol red) supplemented with a 10% heat-inactivated foetal bovine serum, 100 U/ml penicillin, 100 μg/ml streptomycin and 2,5 μg/ml amphotericin B on 25 cm2 tissue culture flasks (EasYFlasks™Nunclon™Δ, Nunc GmbH Wiesbaden, Germany). GMK cells were cultured in a monolayer in a CO2 cell incubator at 37°C in an atmosphere of 5% CO2. Afterwards, the cells were counted in a Neubauer hemocytometer (BlauBrand, BRAND GmbH) by the compact inverted microscope Olympus CKX41. The assays of cytotoxicity GMK cells were prepared at a density of 1×106 cells/cm3.
To assay cell viability, an MTT test was used based on the MTT Assay DB-ALM Protocol n°17, ECVAM – European Centre for the Validation of Alternative Methods, Database Service on Alternative Methods to Animal Experimentation. The experiment was begun by designation of the IC10 and IC50 values of drugs. To determine the effects on cell viability, the drugs were added to the GMK cells in the same volume (100 μl/well) and incubated for 24 h at the following initial concentrations: MTX (5.5 μM), atorvastatin (100 μM), rosuvastatin (2.0 μM), pravastatin (1.5 μM) and in their three times higher concentrations: MTX (16.5 μM), atorvastatin (300 μM), rosuvastatin (6.0 μM), pravastatin (4.5 μM). These initial concentrations of drugs were less than the determined IC10 inhibitory concentration of 10% to the GMK cell line after 24h of incubation in the MTT test. The combinations of MTX with statins were used in the following three proportions of concentrations: 1:1 i.e. MTX (5.5 μM) with atorvastatin (100 μM) or rosuvastatin (2.0 μM), or pravastatin (1.5 μM) and 1:3 MTX (5.5 μM) with atorvastatin (300 μM), or rosuvastatin (6.0 μM), or pravastatin (4.5 μM) and 3:1 i.e. MTX (16.5 μM) with atorvastatin (100 μM), or rosuvastatin (2.0 μM), or pravastatin (1.5 μM). After incubation, 10 μl MTT solution (5 mg/ml) was added to each well microplate and incubated for 3 h at 37°C. At the end of incubation, the culture medium was removed carefully from each well, and 100 μl DMSO were added. The absorbance of each well was measured at 550 nm using the automated absorbance microplate reader ELx808IU (Bio-Tek Instruments Inc.). The viability of GMK cells was expressed in % of the control group.
The cytotoxicity detection kit (LDH) is a colorimetric assay for the quantitation of cytotoxicity/cytolysis based on the measurement of LDH activity revealed by damaged cells. The drugs were added to the GMK cell line and incubated for 24 h at the same concentrations as in the MTT assay. After incubation, a 100 μl cell-free culture medium was removed carefully from each well and transferred into the corresponding wells of a new optically clear 96-well microplate. To determine the LDH activity in cellfree culture medium, 100 μl of reaction mixture (diaphorase/ NAD+ and iodotetrazolium chloride and sodium lactate) was added ex tempore to each well and incubated for up to 30 min at 15-25°C. The absorbance of each well was measured immediately after incubation at 490 nm using an automated absorbance microplate reader ELx808IU (Bio-Tek Instruments Inc.). Cytotoxicity of methotrexate, statins and their simultaneous treatment was calculated with a formula provided in the manufacturer’s instructions. Cytotoxicity was expressed in %.
The Roche Cell Death Detection ELISA kit uses a quantitative detection of histone-associated DNA fragments in mono-and oligonucleosomes (a marker for apoptotic cells). The rate of apoptosis is reflected by the enrichment of nucleosomes in the cytoplasm. For the evaluation of GMK cell apoptosis, the drugs and their combinations were added to a GMK cell line and incubated for 24h. At the end of the incubation period, the cells were lysed and the level of apoptosis was determined using the ELISA method which measured the cytoplasmic histone-associated DNA fragments (mono- and oligonucleosomes). Absorbance was measured at 405 nm using an automated absorbance microplate reader ELx808IU (Bio-Tek Instruments Inc.). the results were expressed by the enrichment factor (the specific enrichment of mono-and oligonucleosomes released into the cytoplasm). The enrichment of mono-and oligonucleosomes released into the cytoplasm is calculated as the absorbance of sample cells/absorbance of control cells. The enrichment factor was used as a parameter of apoptosis.
The results are expressed as mean ± SEM. The statistical significance among the groups was determined by using the analysis of variance (ANOVA). Double-drug groups were compared with groups of single drug using two-way ANOVA accompanied by a post-hoc Newman-Keuls test. P-values less than 0.05 were considered significant.
Results
The IC50 values of methotrexate, atorvastatin, rosuvastatin and pravastatin were determined from dose–response curves and were shown in Table 1.
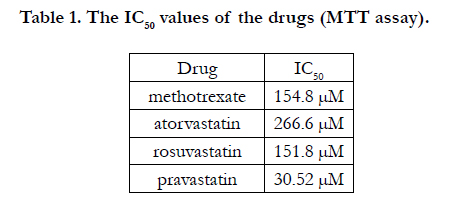

Table 1. The IC50 values of the drugs (MTT assay).
The viability of GMK cells after 24h incubation with the combination of MTX (5.5 or 16.5 μM) with atorvastatin (100 μM) was about 55% (Figure 1A). This cell viability was significantly lower compared with MTX or atorvastatin only. It should be noted that after 24h incubation of the GMK cell line with methotrexate only (5.5 or 16.5 μM) a reduced cell viability was observed (by about 21% and 27%, respectively). Atorvastatin in the initial concentration of 100 μM decreased the GMK cell viability by 37 % but in a three times higher a concentration of 300 μM it caused a decrease
of cell viability by 67.15%. After 24h incubation of the GMK cells with MTX (5.5 μM) and atorvastatin (300 μM) simultaneously, cell viability dwindled by 67.49 %. The lowered viability of the GMK cells does not result from drug combination from a higher concentration of atorvastatin. Rosuvastatin (2.0 or 6.0 μM) decreased cell viability by about 38 % or 52 %, respectively (Figure 1B). After 24h incubation of the GMK cells with MTX (5.5 or 16.5 μM) in combination with rosuvastatin (2.0 or 6.0 μM), their viability was significantly reduced compared with the viability of GMK cells incubated only with MTX or only with rosuvastatin, which, in this case, points to the intensification of their cytotoxic effect. Similarly, pravastatin (1.5 μM) also decreased cell viability by 39.47 % and by 54.64% in a three times higher a concentration (Figure 1C). Incubation of the GKM cells with the combination of MTX (5.5 or 16.5 μM) and pravastatin (1.5 or 4.5 μM) significantly inhibited cell growth compared with the groups incubated with each of the two drugs separately.
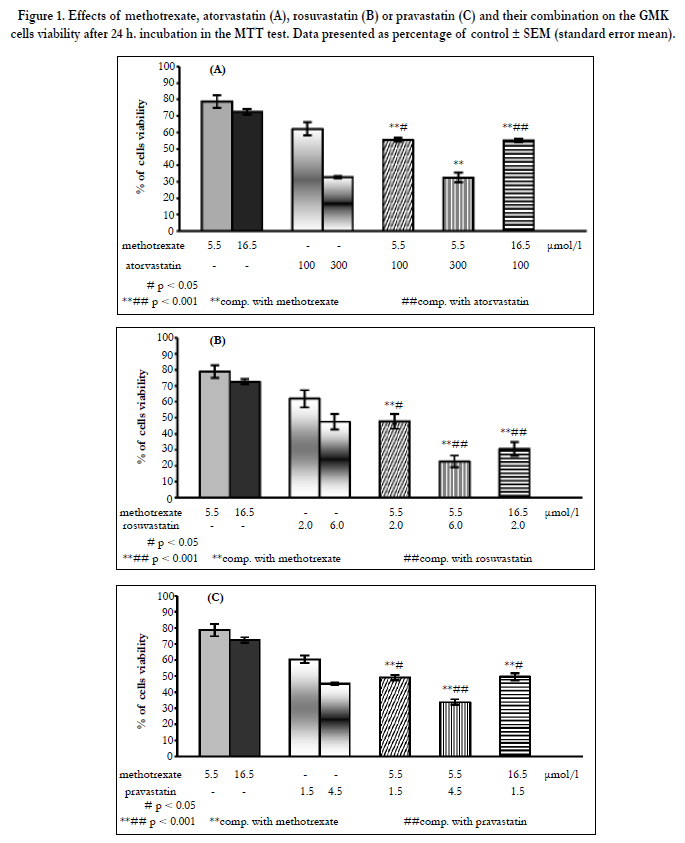

Figure 1. Effects of methotrexate, atorvastatin (A), rosuvastatin (B) or pravastatin (C) and their combination on the GMK cells viability after 24 h. incubation in the MTT test. Data presented as percentage of control ± SEM (standard error mean).
After 24h of simultaneous incubation of the GMK kidney cells with the combination of MTX (5.5 μM) with atorvastatin (100 μM), the cytotoxicity of the drugs was below 10% and was significantly lower compared with the result in the group of cells incubated only with atorvastatin (Figure 2A). The cytotoxicity of combination of MTX (16.5 μM) with atorvastatin (100 μM) increased to 32.74 % as compared with the results of the groups of GMK cells incubated with each drug separately, with indicates adverse interaction of both drugs. The highest increase in cytotoxicity (about 62%) was noted after the simultaneous incubation of the GMK cells with MTX (5.5 μM) and atorvastatin (300 μM). This significant increase in cytotoxicity was caused by the action of atorvastatin at the higher concentration.
A similar effect was observed in the MTT test. It is worth noting that after the GMK cell incubation, a significant increase of cytotoxicity was found only with atorvastatin (100 or 300 μM) (by 19.08% and 59.06%, respectively). In the case of MTX in the concentrations of 5.5 or 16.5 μM, minimal cytotoxicity was noted (below 10%). The cytotoxicity of the combination of MTX (5.5 μM) with rosuvastatin (2.0 μM) did not exceed 10% (Figure 2B). After 24h of incubation of the GMK kidney cells with the combination of MTX (5.5 μM) and rosuvastatin (6.0 μM), an over 20% increase in cytotoxicity was observed compared with the groups of cells incubated with each of the two drugs separately. The combined use of MTX (16.5 μM) and rosuvastatin (2.0 μM) also revealed a slight increase in their cytotoxicity. After the incubation of the GMK cells with MTX (5.5 μM) with pravastatin (1.5 or 4.5 μM), no significant changes were reported indicative of their cytotoxic action in the LDH assay (Figure 2C). Only a slight increase (by about 25 %) was found in the cytotoxicity of the combination of MTX (16.5 μM) with pravastatin (1.5 μM).
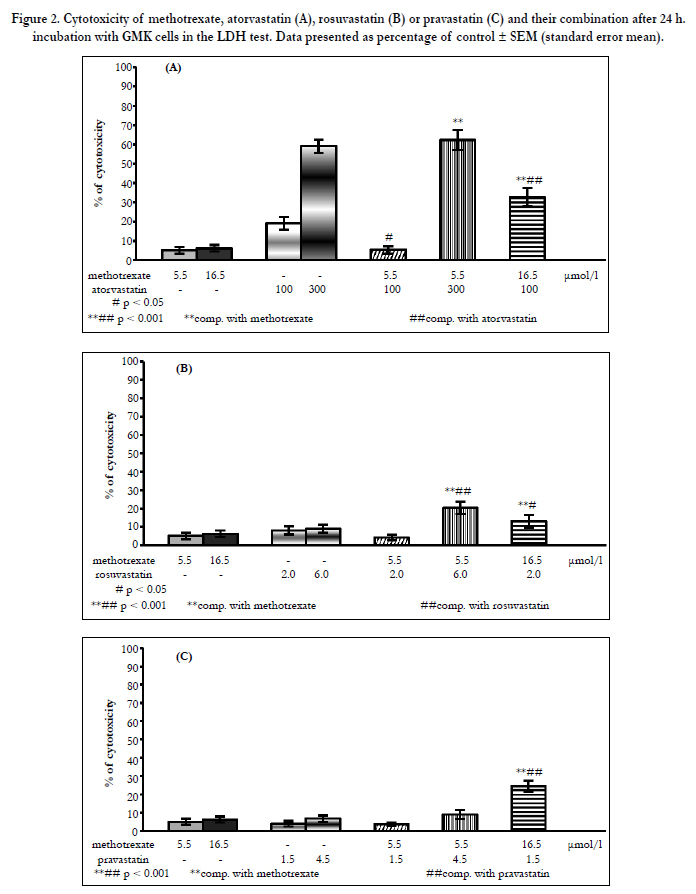

Figure 2. Cytotoxicity of methotrexate, atorvastatin (A), rosuvastatin (B) or pravastatin (C) and their combination after 24 h. incubation with GMK cells in the LDH test. Data presented as percentage of control ± SEM (standard error mean).
The examination of apoptosis demonstrated a significant increase in DNA fragmentation as a consequence of rising apoptosis in the GMK cells incubated for 24h with atorvastatin only at the concentration of 100 μM (Figure 3A). The combined application of MTX (5.5 or 16.5 μM) with atorvastatin (100 μM) also significantly raised the level of mono-and oligonucleosomes in the cytoplasm of the tested cells in comparison to the results obtained in the cell groups incubated only with MTX or only with atorvastatin at appropriate concentrations. Yet, it should be noted that in the group of cells subjected to combined action of MTX (5.5 μM) with atorvastatin (300 μM), no increase of cell apoptosis was found. The studies also showed a slight increase in DNA fragmentation in the GMK cells incubated for 24h with MTX 5.5 μM in combination with rosuvastatin at 6.0 μM (Figure 3B) or pravastatin at 4.5 μM (Figure 3C). Still, it should be noted that these results were statistically significant only in comparison to MTX and were similar to the results obtained in the cell groups incubated only with statins. These results may suggest that the increase in the apoptosis of the GMK cells should be attributed to statins used in higher concentrations.
All of the above-mentioned parameters were evaluated in the presence of statins solvents (control GMK cells + solvents), and there were no significant differences between the control and the solvent-treated cells.
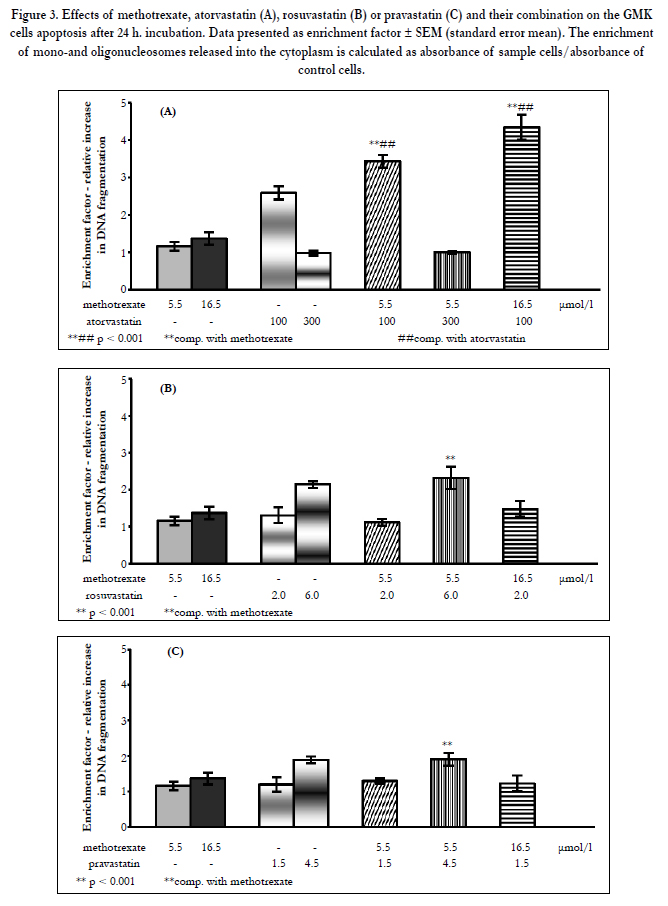
Figure 3. Effects of methotrexate, atorvastatin (A), rosuvastatin (B) or pravastatin (C) and their combination on the GMK cells apoptosis after 24 h. incubation. Data presented as enrichment factor ± SEM (standard error mean). The enrichment of mono-and oligonucleosomes released into the cytoplasm is calculated as absorbance of sample cells/absorbance of control cells.
Discussion
Pharmacotherapy of cancer diseases is associated with many therapeutic problems. One of them are the interactions between cytostatic drugs and drugs from other pharmacological groups [1]. Cancer patients often suffer from cardiovascular diseases with lipid disorders and they have to take the statins. Therefore, the aim of this study was a preliminary assessment of cytotoxicity of MTX, statins (atorvastatin, rosuvastatin or pravastatin) and their combinations in green monkey kidney cells. In our study, was used initial concentrations of drugs: MTX (5.5 μM), atorvastatin (100 μM), rosuvastatin (2.0 μM) and pravastatin (1.5 μM) for the examination of drug-drug interaction. The starting assumption for the evaluation of the drugs interaction was to use drug concentrations lower than previously determined IC10 values after 24h of incubation GMK cell line in the MTT test. To assess the nature of the interaction of drugs was also utilized the concentration of three times higher ie.: MTX (16.5 μM), atorvastatin (300 μM), rosuvastatin (6.0 μM), pravastatin (4.5 μM). Combinations of drugs were used only in three following proportions of concentrations ie.: 1:1, 1:3 and 3:1 in order to carry out an additional assessment of the nature of drugs interaction using isobolographic analysis (data not included in this study). The literature shows that these concentrations of statins used in the study are effective for various cancer cells line [24-26]. In the case of MTX, the range of cytotoxicity doses for tumor cells used in the works of different authors was quite high and it ranged from 10-9 – 10-6 mol/l [27-29]. It is worth noting that in cancer patients treated with MTX, the serum levels above 10 μM increases the risk of kidney damage [30]. The study found that the combined use of MTX with atorvastatin (100 uM) significantly amplify the cytotoxic effect of the combination of both drugs in the GMK cells both in the MTT as well as LDH assay, which indicates their unfavourable interaction. In order to distinguish between the types of GMK cells death as a result of incubation with the combination of the studied drugs, ELISA test (Cell Death Detection) was applied. Apoptosis plays a key role in many processes, both physiological and pathological, such as carcinogenesis, cancer progression, and the killing of cancer cells by cytostatic drugs [31, 32]. The study demonstrated an increase in apoptosis of the GMK cells treated with MTX in combination with atorvastatin (100 μM). In the cell group incubated with MTX and atorvastatin (300 μM), there was no increase in cell apoptosis, which, in this case, suggests a different type of cell death: necrosis. This study also revealed a significant decrease in the viability of GMK cells in the MTT assay after incubation with MTX in combination with rosuvastatin or pravastatin. However, in the LDH assay, there were no significant changes clearly indicating the intensification of the cytotoxic effects. Based on the obtained results, it appears that the MTT test was more sensitive as shown in the examination of the cytotoxic effect of combination of these drugs. The absence of clear results in the LDH assay showing an increased cytotoxicity of MTX in combination with rosuvastatin or pravastatin may be due to the differences in the evaluation of cytotoxicity in both the assays. The LDH assay is based on the measurement of the activity of lactate dehydrogenase, an enzyme released from injured cells. In a situation where the cell membrane is not damaged, the increased release of the enzyme is not seen.
Conclusion
The results obtained in this study, especially in the MTT test, indicate a negative impact of the combined application of methotrexate and statins on cell viability, and these changes cannot be ignored. These observations, in addition to the cognitive aspect, may have a practical importance in the treatment of patients with a malignant disease and suffering from a lipid disorder. In patients treated with methotrexate and statins should be carefully monitor of renal function, because may be increased the renal toxicity of these drugs.
Acknowledgment and Declaration
Financial support for this study was provided by the Medical University of Lublin, Poland. The authors report no conflicts of interest. This article is approved by all co-authors. The authors alone are responsible for the content and writing of this article.
References
- Blower P, de Wit R, Goodin S, Aapro M (2005) Drug – drug interactions on oncology: Why are they important and can they be minimized? Crit Rev Oncol Hematol 55(2): 117-142.
- McGuire JJ (2003) Anticancer antifolates: current status and future directions. Curr Pharm Des 9(31): 2593-2613.
- Bangert CA, Costner MI (2007) Methotrexate in dermatology. Dermatol Ther 20(4): 216-228.
- Shen S, O’Brien T, Yap LM, Prince HM, McCormack CJ (2012) The use of methotrexate in dermatology: a review Australas J Dermatol 53(1): 1-18.
- Tian H, Cronstein BN (2007) Understanding the mechanisms of action of methotrexate. Implications for the treatment of rheumatoid arthritis. Bull NYU Hosp Jt Dis 65(3): 168-173.
- Świerkot J (2007) Toxicity of low dose methotrexate in rheumatoid arthritis. Adv Clin Exp Med 16(2): 287-295.
- Green MR, Chamberlain MC (2009) Renal dysfunction during and after high-dose methotrexate. Cancer Chemother Pharmacol 63(4): 599-604.
- Strang A, Pullar T (2004) Methotrexate toxicity induced by acute renal failure. J R Soc Med 97(11): 536-537.
- Widemann BC, Adamson PC (2006) Understanding and managing methotrexate nephrotoxicity. Oncologist 11(6): 694-703.
- Morsy MA, Ibrahim SA, Amin EF, Kamel MY, Rifaai RA, et al. (2013) Curcumin ameliorates methotrexate-induced nephrotoxicity in rats. Adv Pharmacol Sci 2013: 1-7. http://dx.doi.org/10.1155/2013/387071.
- Devrim E, Cetin R, Kiliçoğlu B, Ergüder BI, Avci A, et al. (2005) Methotrexate causes oxidative stress in rat kidney tissues. Ren Fail 27(6): 771-773.
- Merx MW, Weber C (2008) Benefits of statins beyond lipid lowering. Drug Discovery Today: Dis Mech 5(3): e325-e331.
- Davignon J (2004) Beneficial cardiovascular pleiotropic effects of statins. Circulation 109(23 Suppl 1): III39-43.
- Liao JK, Laufs U (2005) Pleiotropic effects of statins. Annu Rev Pharmacol Toxicol 45: 89-118.
- Duncan RE, El-Sohemy A, Archer MC (2005) Statins and cancer development. Cancer Epidemiol Biomarkers Prev 14(8): 1897-1898.
- Graaf MR, Richel DJ, van Noorden CJ, Guchelaar HJ (2004) Effects of statins and farnesyltransferase inhibitors on the development and progression of cancer. Cancer Treat Rev 30(7): 609-641.
- Hindler K, Cleeland CS, Rivera E, Collard CD (2006) The role of statins in cancer therapy. Oncologist 11(3): 306-315.
- Kabel AM, Abdel-Rahman MN, El-Sisi AD, Haleem MS, Ezzat NM, et al. (2013) Effect of atorvastatin and methotrexate on solid Ehrlich tumor. Eur J Pharmacol 713(1-3): 47-53.
- Dashti-Khavidaki S, Moghaddas A, Heydari B, Khalili H, Lessan-Pezeshki M, et al. (2013) Statins against drug-induced nephrotoxicity. J Pharm Pharm Sci 16(4): 588-608.
- Armitage J (2007) The safety of statins in clinical practice. Lancet 370(9601): 1781-1790.
- Bellosta S, Paoletti R, Corsini A (2004) Safety of statins: focus on clinical pharmacokinetics and drug interactions. Circulation 109(23 Suppl 1): III50-57.
- Shitara Y, Sugiyama Y (2006) Pharmacokinetic and pharmacodynamic alterations of 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors: Drug–drug interactions and interindividual differences in transporter and metabolic enzyme functions. Pharmacol Ther 112(1): 71- 105.
- Izdebska M, Natorska-Chomicka D, Jagiełło-Wójtowicz E (2014) Preliminary studies evaluating cytotoxic effect of combined treatment with methotrexate and simvastatin on green monkey kidney cells. Acta Pol Pharm 71(3): 515-520.
- Gauthaman K, Richards M, Wong J, Bongso A (2007) Comparative evaluation of the effects of statins on human stem and cancer cells in vitro. Reprod Biomed Online 15(5): 566-581.
- Hijona E, Banales JM, Hijona L, Medina JF, Arenas J, et al. (2012) Pravastatin inhibits cell proliferation and increased MAT1A expression in hepatocarcinoma cells and in vivo models. Cancer Cell Int 12: 5.
- Miraglia E, Högberg J, Stenius U (2012) Statins exhibit anticancer effects through modifications of the pAkt signaling pathway. Int J Oncol 40(3):867-875.
- Decker S, Winkelmann W, Nies B, van Valen F (1999) Cytotoxic effect of methotrexate and its solvent on osteosarcoma cells in vitro. J Bone Joint Surg Br 81(3): 545-551.
- Hattangadi DK, DeMasters GA, Walker TD, Jones KR, Di X, et al. (2004) Influence of p53 and caspase 3 activity on cell death and senescence in response to methotrexate in the breast tumor cell. Biochem Pharmacol 68(9):1699-1708.
- Kimura E, Nishimura K, Sakata K, Oga S, Kashiwagi K, et al. (2004) Methotrexate differentially affects growth of suspension and adherent cells. Int J Biochem Cell Biol 36(5): 814-825.
- Al-Turkmani MR, Law T, Narla A, Kellogg MD (2010) Difficulty measuring methotrexate in a patient with high-dose methotrexate-induced nephrotoxicity. Clin Chem 56(12): 1792-1794.
- Lowe SW, Lin AW (2000) Apoptosis in cancer. Carcinogenesis 21(3): 485- 495.
- Ulukaya E, Acilan C, Yilmaz Y (2011) Apoptosis: why and how does it occur in biology? Cell Biochem Funct 29(6): 468-480.





