Tragedies in Clinical Trials - A History Wrapped Up
Bansal P1*, Gupta S2, Christopher AF3, Gupta V4
1 Joint Director, University Centre of Excellence in Research, Baba Farid University of Health Sciences, Faridkot, India.
2 Division of Clinical Research, University Centre of Excellence in Research, Baba Farid University of Health Sciences, Faridkot, India.
3 Demonstrator, Division of Clinical Research, University Centre of Excellence in Research, Baba Farid University of Health Sciences, Faridkot, India.
4 Technical Officer, University Centre of Excellence in Research, Baba Farid University of Health Sciences, Faridkot, India.
*Corresponding Author
Dr. Parveen Bansal,
Joint Director,
University Centre of Excellence in Research,
Baba Farid University of Health Sciences, Faridkot,
151203, India.
Tel: 08872016290
E-mail: bansal66@yahoo.com
Article Type: Review Article
Received: May 06, 2015; Accepted: July 10, 2015; Published: July 17, 2015
Citation: Bansal P, Gupta S, Christopher AF, Gupta V (2015) Tragedies in Clinical Trials - A History Wrapped Up. Int J Clin Pharmacol Toxicol, 4(3) 169-178. doi: dx.doi.org/10.19070/2167-910X-1500029
Copyright: Bansal P© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Today foremost emphasis is being given to the protection of patient’s safety and ethics during the conduct of clinical trials. Serious considerations by regulatory authorities are taken to safeguard the patient’s right, safety and wellbeing involved in a clinical trial. In addition considerations like International Conference on Harmonization (ICH) guidelines, Investigational New Drug (IND) application, New Drug Application (NDA), Post Marketing Surveillance (PMS) and Periodic Benefit-Risk Evaluation Report (PBRER) formerly known as Periodic Safety Update Report (PSUR) submissions to different regulatory authorities has also been framed to strengthen ethics and patient’s safety. However modern clinical trials have evolved through serious consequences and tragedies like Thalidomide Tragedy, Sulfanilamide Disaster, Clioquinolol Tragedy, etc. associated with high morbidity and mortality. Potential reasons behind these tragedies include unethical clinical practices, inadequate preclinical safety and efficacy data, non-scientific conduct, lack of attentiveness for patient care, misinterpretation of safety data, lack of pharmaco-vigilance, slow withdrawal of drug from market etc. Hence toiling efforts have been made and should be made in investigating lacunas in national as well as international systems that encourage launch of such spurious drugs that needed withdrawals after 10-20 years of public use. This manuscript intends to collect and present data on tragic clinical trials, highlight the tragedies that occurred during the dark era of clinical trials and enumerate various corrective actions taken in response to the lessons learnt during those clinical trials.
2.Introduction
3.Below are few of the Important Tragedies in history of clinical trials
4.Other Tragedies in Clinical Trials
5.Conclusion
6.Acknowledgement
7.References
Keywords
Clinical Trials; Tragedies; Regulatory Authorities; Adverse Drug Reaction.
Introduction
Today is the era of evidence based medicine and foremost emphasis is being given for protection of ethics in the clinical trials. Serious considerations by regulatory authorities to safeguard patient rights, safety and well being have been framed. Clinical trials are research based studies performed on human beings [1] for developing therapeutic interventions and to investigate pathogenesis of disease. These trials or studies test the efficacy of a novel medicine and provide a comparative tool of novel therapy to previous one by established interventions [2]. Efforts are made to prove safety and efficacy of novel drugs in human subjects [3]. Preclinical studies are performed in animal species to study the safety and efficacy of the new drug prior to the clinical trials. Only after successful preclinical studies, permission is taken to investigate safety and efficacy in human subjects enrolled in a clinical trial [4]. Clinical trials are carried through phases from I to IV [5]. Clinical research is a complete story of the drug molecules from its invention in lab to its arrival in the market for customer benefit [4].
Irrespective of the advantages and safety provided to the subjects, accidents occurs quite frequently during the conduct of clinical trials. Clinical research laid the foundation for establishing new regulations and policies, social benefits to subjects. However the violation of ethics endangers life of the participants. Involuntary participations and unethical conduct was a pathway to injustice. On literature review it was found that there was no focus on ethical considerations from the year 1930 till 1960. During the clinical trials as a consequence, there were tragedies associated with high morbidity and mortality. Potential rationale behind all these tragedies were non scientific conduct, misinterpretation of safety data, inadequate preclinical data on safety and efficacy, victims treated as guinea pigs, lack of pharmaco-vigilance evidence, lack of attentiveness in clinical researchers engaged in patient care, inappropriate patient consent, hindrance/slow withdrawal even after denunciation of drug from market etc.
This review intends to highlight some of the unfortunate tragediesthat occurred due to some or the other reason in conduct of clinical trials. Authors also intend to highlight that despite such stringent laws in favor of patients supported by regulatory authorities like FDA; drugs were being launched and withdrawn from market so frequently. Authors have made an effort to find out the lacunas in national as well as international systems/regulatory authorities that discourage launch of such spurious drugs that need withdrawals after 10-20 years of public use.
Each tragedy led to establishment of respective regulations in the favor of human ethics. Every stage in clinical research development represented an initiative step to protect human rights [5], safety and well being of human subjects [6]. The current regulations and policies are the corrective actions in response to the past tragedies. Tragedies of clinical trials and regulations are directly related [7].
- No scientific knowledge and lack of integrity of trials
- No approved Protocol
- Lack of ethical considerations
- Patient consent not received
- Lack of preclinical studies for safety and efficacy
- Participation in trials against subject’s willingness
Below are few of the Important Tragedies in history of clinical trials
Tuskegee Syphilis study began in 1932 and was concluded in 1972, in Alabama. This biomedical research study was performed for a longer duration of 40 years [9]. This study involved unethical experiments and practice [11]. Victims were not informed about the details of the experiment [10]. The aim of the study was to investigate the progression of syphilis in untreated people [12]. Stage of disease was asymptomatic during study. The subjects enrolled were neither informed about the disease nor treated despite the availability of the treatment and facilities. Drug available in the market for treatment was Penicillin [10]. The experiments were terminated in 1972 as a consequence of public disclosure by media. Following which National Research Act (1974) founded National Commission for protection of human subjects of biomedical and behavioral research. In an attempt to protect ethics Belmont report was proposed in 1979 [6]. This report was prepared by National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. It stated guidelines for ethics [13]. This report was an effort to encourage safety of human subjects during experiments [14].
This incident happened in East Virginia and West California. More than 100 people died in 15 states in U.S. [15]. This tragedy occurred in 1937 following consumption of Sulfanilamide indicated as antibacterial to cure streptococcal infections. Earlier drug was sold in solid form like capsule and tablets but later its manufacturers decided to formulate a liquid suspension for oral consumption to increase its market value by using a solvent named diethylene glycol [16]. The suspension was sweet with raspberry flavor having good color, fragrance and acceptable taste [17]. As there were no established regulations to conduct preclinical or clinical trials, new suspension was not studied for safety and toxicity. Diethylene glycol: an antifreezing agent was tested as toxic ingredient by the AMA laboratory and a warning was made via newspapers and radio to the public that elixir Sulfanilamide was toxic and deadly poison. Few simple animal studies had demonstrated the elixir was toxic and could result in renal damage but regulations were not strengthened enough to stop marketing of toxic drugs [15]. Federal Food and Drug Act, 1938 was established in response to this tragedy making the premarketing safety data for novel drugs mandatory. This act brought profound changes in Food and Drug Administration [18].
This was another chain of unethical studies enrolling Human subjects (Prisoners and disabled) started in early 1940s in Germany. Participation was a forceful act and informed consent ware not obtained. A large number of people died in these experiments and several others were killed to perform autopsy. Survivors of experiments suffered from mental torture, mutilation. There were a number of experiments conducted under this trial [19]. Some of them are listed below:
These experiments were performed to gather knowledge about reproductive system and racial duplication of twins. Several twin children were involved in these studies [20].
These experiments led to unethical acts like painful and involuntary removal of limbs, muscle in concentration camps to study process of transplantation from one person to another [19, 20].
These experiments were performed to obtain efficacious therapy for subjects of immersion hypothermia [21]. Participants were forced to remain in coldicy water either naked or dressed to simulate the conditions of German pilots and to see tolerance to intense cold [5, 19, 21].
These were carried by way of induction of malaria parasitic infection in human subjects and treatment with pharmaceutical products to find out immunity against parasitic infection.
Another example of inhuman studies in which wound were induced in participants by exposure to mustard gas and investigations were done to obtain therapy for mustard gas burns.
These were conducted to find natural protection against Tuberculosis. These include induction of tuberculosis in the participants.
These experiments were conducted to study the efficacy of sulfonamide on wounds. Supply of blood to wound was blocked to provide Warfield wound appearance. Wound was infected and then treated with drug. These experiments were carried from July 1942 to September 1943, to investigate the effectiveness of drug sulfonamide against streptococcus and clostridium Perfringens.
These experiments were performed to know if sea water can be used for drinking [19]. These were inhuman efforts resulting in death. Victims were deprived of drinking water and only sea water was given. These led to severe dehydration and subsequent death [20].
Here subjects were unaware of the experiment. Chemicals were injected into the genital organs of men and women [19] and were exposed to radiations rendering them sterile. Later they presented with various complications like painful uterus, infertility, gastric bleeding and carcinomas [19, 20].
These were conducted to find out the actions of different toxic substances on human subjects. The toxic substances were injected without informing them or combined with meals. Those who survived were killed and autopsies were performed on dead subjects [19]. The logic behind was to assess death rate with poison [20].
In these experiments victims were suspended to high altitude to find consequences of high altitude exposure in an attempt to aid German pilots. A large number of victims died during these experiments [5, 19].
As a consequence of Nuremberg Trial also known as doctor’s trial, Nuremberg code was established in 1947. This code stated ethical guidelines for research on human subjects. These trials were carried in Nuremberg, Germany. These trials were performed on physicians responsible for conducting unethical experiments in concentration camps. They justified in their defense about lack of rules and regulations regarding experiments [22]. This code addressed protection of human rights in form of informed consent, social advantage, preclinical experiments, voluntary participation and withdrawal from study, risk/ benefit assessment, protection against mortality, disfigurement, performed by qualified physician [5].
This study was performed in Guatemala (A country in Central America) during 1946 to 1948 [23, 24]. Normal human subjects were unwillingly enrolled in these experiments. Informed Consent was not obtained from participants [25]. They were infected with syphilis and other sexually transmitted diseases [24]. This study was done to establish the knowledge about the prevention of sexually transmitted diseases (STD’s) and therapeutic efficacy of Penicillin in syphilis treatment [25]. Penicillin treatment was made available only to one third of infected people only. Eighty three people died in these experiments. Such experiments and procedures adopted were unethical [26].
Thalidomide Tragedy is also known as Canadian Tragedy [27]. Thalidomide was manufactured by Chemie Grunthal and marketed in Germany in 1957 as an over-the-counter drug for sleeplessness (insomnia), cold and cough [28, 29]. It was marketed as a ‘drug with safety profile’ for everyone, including pregnant mother and child [17]. Animal studies were found to be safe but safety studies on human were not preformed [28]. It was an Australian physician Dr. William McBride who first noticed that the thalidomide could relieve pregnant women from morning sickness. Therefore he started prescribing thalidomide to his pregnant patients [29]. Subsequently it became extremely popular [17]. In year 1960 thalidomide was distributed in 46 countries. Expecting mothers started using Thalidomide without prescription. In 1961, congenital anomalies were reported in newborns e. g. Phocomelia (the stunting or lack of limbs). Later, it was confirmed that the Thalidomide caused severe congenital malformations. The drug interrupted the normal development process at that stage when thalidomide was exposed during pregnancy. It was reported that 161 babies suffered from phocomelia resulting in discontinuation of drug in Germany [29]. Mortality was approximately 2,000 and morbidity was more than 10,000 [30]. In 1962, the drug was withdrawn from market [31]. Anomalies occurred due to lack of knowledge of drug’s pharmacokinetics and pharmacodynamics and insufficient preclinical safety data [32]. In response to thalidomide disaster “Kefauver Harris Amendment” was released in the same year 1962 which was an amendment to Federal Food Drug and Cosmetic Act 1938. This act made it mandatory to the pharmaceutical company to state preapproval safety and efficacy of their drug and describing the possible side effects of the drug [33]. Thalidomide was again approved by FDA in 1998 for treatment of Hansen’s disease and multiple myeloma [34]. Due to its adverse effects on embryogenesis, System for Thalidomide Education and Prescribing Safety [S.T.E.P.S.] program was initiated by Celgene pharmaceuticals which provide regulations for drug marketing and essential patient education [29]. This program is now a day’s named as Thalomid REMS (Risk Evaluation Mitigation Strategy) Program [35].
Clioquinolol (Iodochlorhydroxyquin) was approved as over-thecounter drug in Japan for the treatment of diarrhea and gastric disorders [36]. Drug was marketed in 1953 by Ciba-Geigy [37]. By 1957 to 1970 Japanese people started suffering from SMON (sub acute myelo-optic neuropathy) a complication affecting brain and gastrointestinal System. Approximately 10,000 people were affected [38]. These complications stemmed from lesions in spinal long tracts and optic tracts e. g. distal dominant axonopathy. Similar complications occurred in animals [39]. A number of 30,000 cases of blindness and paralysis were reported in Japan [40]. Causal relationship with drug was established later in1969-70 [38]. Preclinical animal studies were conducted with safe results [40]. Eventually in 1970 Clioquinol was removed from market following neuropathies in Japanese population [41].
Accutane is a vitamin A formulation, developed in 1979, used to cure acne [42, 43]. Accutane was indicated for treatment of acne of serious type [43]. Accutane was manufactured by Roche Pharmaceuticals. It got US FDA approval in 1982. When no other alternative therapy was available, it was the only treatment of choice for acne [44]. Later drug was found to be associated with cases of ulcerative colitis [45], crohan’s Disease, depression, hepatic damage, congenital defects and miscarriage. It was banned by FDA in 2009. Accutane is not being manufactured currently, but its generic version Isotretinoin is still marketed [44]. In 2006 FDA had put forward a proposal in reaction to the adverse effects of Accutane, called “iPLEDGE” Program. Under this program physician, chemist and consumer will have to fulfill certain guidelines for drug safety [46] i.e. drug not to be taken in case of allergy to isotretinoin, history of pregnancy, heart problem, bone disorder, hepatic disorder, and intestinal disease. If administered during pregnancy fatal defects can occur. Drug is contraindicated in pregnancy. Pregnancy test is the first requirement of iPLEDGE Programme [42].
Pergolide (Permax) was approved in 1982 for the treatment of Parkinson’s disease which is a neuromuscular disorder [47, 48]. During the course of therapeutical use several cases of cardiac abnormalities like valvular diseases were reported as compared to patients not medicated with medicine [49]. For the reasons of human safety drug was removed from market [50]. Cardiac abnormalities were linked to incompetency of heart valves [51]. This occurred as a result of interaction of drug with receptors of cardiac muscles resulting in proliferation [52]. In year 1996, FDA released a black box warning about adverse effects. For the reasons of human safety, drug was removed from US market in 2007, but was still used for vetenary practice (for treatment of horses) [50, 52].
Cerivastatin (Baycol, Lipobay) has been used as preventive therapy for cardiovascular diseases with the property of lowering cholesterol [53]. Baycol was introduced in market in 1997 after approval by FDA. Indications of drug were to use as an adjunctive therapy to diet [54]. First case of death after marketing was found in 2000. Subsequently several cases of deaths were reported. These death cases were proportionally related to increased dose level. Despite of this information available FDA took no action [53]. Serious anomaly associated with the drug was Rhabdomyolysis. Patients taking Cerivastatin were at higher risk than other types of statin [55]. Rhabdomyolysis is inflammation of muscles resulting in splitting of muscle cells leading to release of its components in circulation. Renal blockage leading to renal failure was the cause of patient’s death. Since other statin drugs are available in market for patient use Baycol withdrawal has not eliminated fatal complication [53]. Several cases of drug interactions were also reported [56]. Some patients were asymptomatic but affected ones had severe morbidity [57]. Adverse effects were dose related and old aged females were involved more frequently [58]. Approximately 60 patients died of Rhabdomyolysis leading to removal of drug from market [53]. Laboratory finding were associated with increased levels of myoglobin in blood circulation which is a positive indicator of myopathy [59].
Rezulin was indicated for treatment of type 2 Diabetes Mellitus [60]. It was approved by FDA in 1997 though the results of clinical trials were not safe [61, 62]. In post marketing survey, drug was found to be associated with hepatic manifestations resulting in 63 deaths due to hepatic failure [62, 63]. Subsequently FDA decided to remove drug from market and in 2000 Drug was removed from market by manufacturer Parke – Davis [63, 64].
Rapacuronium was approved by US FDA in 1999 as an adjunctive anesthesia for ease of endotracheal intubation [65]. The drug resulted in fatal events like bronchospasm. The air passage became noncompliant during operative procedure which caused death. Patients presented with breathlessness mimicking asthma. Morbidity associated with Raplon was 90. In additions several children and adults suffered from spasmodic attack [66]. In 2001 Raplon was removed from market [65]. During clinical trials of Raplon negative results regarding safety were observed however no death cases were reported. In premarketing clinical trial of Raplon, 3.2% patients suffered with bronchospasm and this information was listed in package insert of drug [67].
Rofecoxib was manufactured by Merck and Co. under brand name Ceeoxx Vioxx, Ceoxx as a Nonsteroidal anti-inflammatory drug (NSAID) to relieve short term pain, pain due to arthritis and pain during menstruation period. Rofecoxib was largely recognized for relieving pain. In 1999 it was approved by FDA. Rofecoxib was available in market in the form of tablet, suspension and injection [68]. Adverse events reported were cardiovascular complications like myocardial infarction and heart stroke on chronic use [69]. VIGOR (Vioxx Gastrointestinal Outcomes Research) study was conducted by Merck for gathering safety data of Rofecoxib. During this study cardiovascular complications were reported and additional data from clinical trials was submitted to FDA. It was analysed from this study that chances of developing heart problem were greater with Rofecoxib than other anti inflammatory drugs [70]. Another study named as “Approve study” proved double risk of cardiac problems with Vioxx. As a consequence vioxx manufacturers removed the drug from market in September 2004 [71].
Raptiva was approved in 2003 for the treatment of psoriasis in adults [72]. Patients were reported with serious infections of nervous system [73]. Later on drug was found to be associated with life threatening diseases of nervous system e. g. Progressive Multifocal leukoencephalopathy (PML), meningitis. The mechanism of action of Raptiva included suppression of immune system to relieve symptoms of psoriasis [72]. The resultant immunosupression was found to be the possible cause for infections and the increased mortality [74, 75]. In October 2008 FDA released a ‘black box’ warning on Raptiva. In June 2009 decision for removal of drug from European market was taken and Raptiva was eventually removed from market [73, 76].
Other Tragedies in Clinical Trials
Lotronex was indicated for the treatment of Irritable Bowel Syndrome (IBS) and severe diarrhea in women [77]. It was marketed in US [78]. In February 2000 drug was approved by FDA. Use of Drug was associated with gastrointestinal complications like constipation and ischemic colitis. This led to withdrawal of drug after some weeks of approval in November 2000. These gastrointestinal complications also required surgical intervention [79]. Lotronex was reapproved under a ‘Risk Management Programme’ following requests by large number of patient who had no alternative treatment. Subsequently the drug was marketed under a program ‘Prometheus Prescribing Program for Lotronex’ to prevent undesired complications [80-82].
Acomplia was drug manufactured by Sanofi- Avenitis to manage body weight and risk factor associated with obesity and was also indicated to decrease appetite. The drug came in the market in 2006 [76, 83, 84]. Acomplia was approved only for the management of obesity by European Union but drug was also used to quit smoking for which it was not approved. Acomplia was not marketed in United States [85-87]. Acomplia was administered along with dietary precautions and exercises [83]. Drug was found to increase the chances of psychiatric disorders i.e. depression and ideas of suicidal attempts [84]. People suffered from several other side effects like nausea, vomiting, headache, dizziness [85]. Benefits from drug were lesser as compared to side effects. In 2008 Acomplia was withdrawn by EMEA [76].
Bextra was marketed as non-steroidal anti-inflammatory drug (NSAID). It was indicated for the management of rheumatoid arthritis, osteoarthritis, symptoms of menstruation period. In 2001 Bextra got FDA approval. It was available without prescription in the form of tablet. Clinical use of Bextra was reported with serious complications like heart attack and stroke and gastrointestinal complications [88-89]. Drug was banned in 2005 [88]. FDA took this step after reevaluation of safety data obtained from the clinical trials of Valdecoxib and risk-benefit assessment as there was no information regarding the association of cardiac safety even with the prolonged use of Bextra [89].
Lumiracoxib as a non steroidal anti-inflammatory drug was marketed by Novartis in 2006. Cases of hepatic complications were reported with use of drug [90]. In 2007 Prexige was withdrawn from market by EMEA [76]. During clinical trials, the laboratory findings revealed significant elevation of liver transaminase level. Prexige was also associated with fatal liver defects which were due to generation of auto antibodies. While in other cases Liver was damaged to the extent requiring transplantation [91].
Sibutramine was a drug used for decreasing apetite and indicated in obesity management [92]. Sibutramine was advertised for weight management as slimming beauty bitter orange slimming capsules [93]. Drug was manufactured by Abott laboratories. Several cases with serious complications were reported like heart attack and stroke [92]. These effects were pronounced in patients with existing cardiac problems [94]. Drug was linked with hypertension and tachycardia requiring daily basis monitoring. Drug had several other side effects like difficulty in breathing, edema, bleeding in stools, vomiting, high temperature and pain in chest etc. It also manifested with drug interactions. Drug trials were not conducted on geriatric patients sufficiently so FDA excluded use of drug for them. In 2010 drug was withdrawn by FDA on the basis of results of SCOUT (Sibutramine cardiovascular outcome trial) Study [92].
Zelmid was marketed in 1982 for the treatment of depression.Post marketing reports revealed association of Zelmid with Zimelidine syndrome (a condition resembling flu), Guillain-Barré syndrome (condition associated with neurological defect) and suicidal thoughts [95-96]. Fatalities were linked with Guillain-Barré syndrome which caused deaths due to respiratory muscle paralysis [97]. Zelmid usage also resulted in congenital anomalies like persistent pulmonary hypertension (PPHN) of neonate as blood circulation system was not developed properly [96]. Preclinical studies were safe but exposure of Zelmid to human subjects resulted in numerous side effects for example damage of nerves, liver, defects of cranium and defects of gastrointestinal system. In 1983 Zelmid was withdrawn from the Market [98].
Ticrynafin was marketed as loop diuretic drug and it lowered the uric acid levels. It got approval by FDA in 1979 for treatment of hypertension. Safety profile of drug was not available. Side effects of Ticrynafin were hepatic complications i.e. hepatitis[99]. Patients presented with pain in the abdomen, elevated body temperature, jaundice, elevated serum transaminase. About 340 Patients suffered side effects associated with Ticrynafin. These hepatic complications were due to induced liver cell antigens and autoantigen alteration followed by sensitization [100]. In 1982 Ticrynafin was withdrawn from market [99].
Omniflox is an oral fluoroquinolone antibiotic [101]. It was manufactured by Abbott Laboratories. It was approved in January 1992 by FDA [102]. Omniflox was used for the treatment of respiratory, urogenital tract infections and infections of skin and soft tissue [101, 103]. After four months of marketing patients suffered with Temafloxacin syndrome featuring chills, high temperature, hemolytic anemia, allergic reactions, malfunctioning of liver and kidney [104]. Six cases of death were also reported. 73 patients were reported with serious adverse drug reactions. In 1992 Omniflox was removed from U S market [103].
Trasylol was administered prior to major surgical procedures of heart and liver to control bleeding [105]. Trasylol was manufactured by Bayer Pharmaceuticals [106]. Drug was approved in 1993 by FDA to be used for subjects of Cardio Pulmonary Bypass Graft Surgery. But Trasylol was used by physicians for the surgeries other than indicated by FDA. This was not in compliance with safety and efficacy requirements by FDA [107]. Trasylol retarded process of fibrin breakdown and loss of blood during surgery maintaining blood pressure. Hence the need for transfusion of blood during surgery reduced [105]. Use of drug was associated with fatal myocardial infarction or cardiac failure, cerebral stroke, kidney failure and hypersensitivity reactions [105, 107]. These complications occurred in dose dependent manner [108]. FDA put forward a Black Box warning in association with hypersensitivity reports which were more significant in patients other than undergoing cardiac surgery [107]. In 2007 Trasylol was provisionally pulled out of market because of risk of these complications. This action was taken to reevaluate safety data [105]. Additional studies (Canadian study) proved the increased chances of mortality with Trasylol [109]. In 2007 Trasylol was removed from U. S., Canada and Germany market [110].
Table 1 represents the important tragedies of Clinical trials and necessary action taken in response to different tragedies.
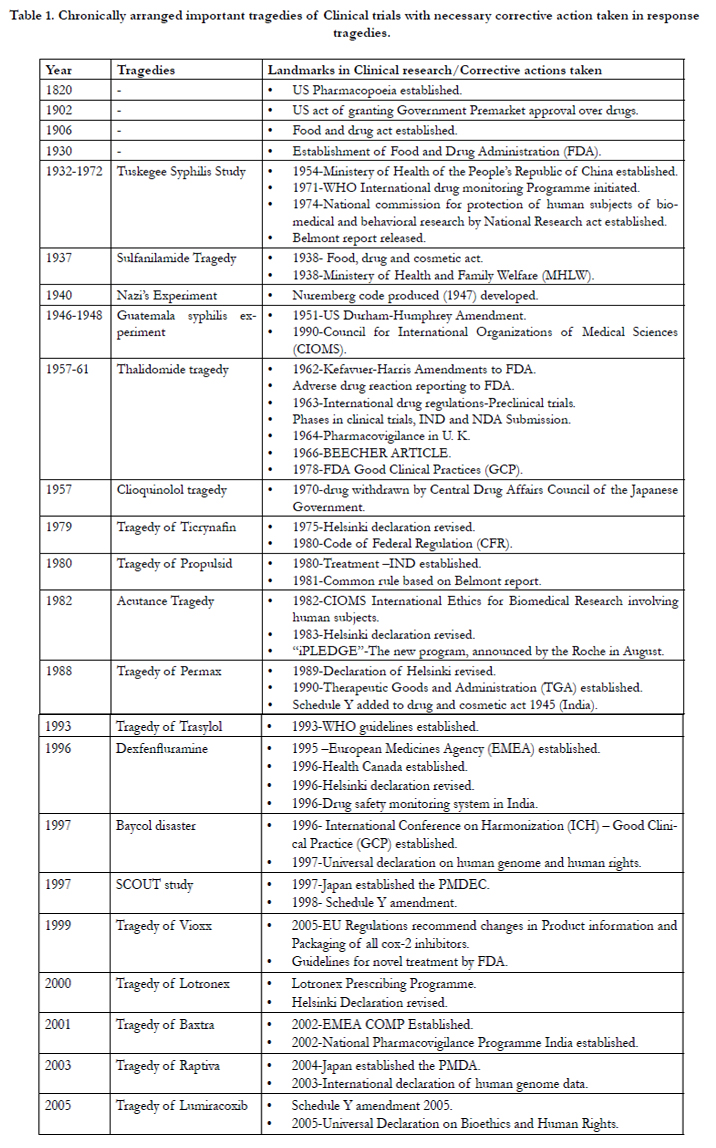

Table 1. Chronically arranged important tragedies of Clinical trials with necessary corrective action taken in response to tragedies.
Behind every episode there is a reason or cause. Determination of cause is a forward step to cure. Tragedies in clinical trials are associated with certain causes. Possible reasons of Tragedies are listed below:
- Unsafe clinical trials conducted in reliance to preclinical data e. g. Raplon [67].
- Approval of drugs despite poor clinical safety profile e. g.Rezulin [64].
- Marketing of drugs not approved by regulatory authorities (USFDA) e. g. Thalidomide [30].
- Approval of drug having poor risk benefit ratio – Rezulin [64].
- Preclinical safety results not compatible with human safety data e. g. Thalidomide [34].
- Poor design and planning of drug trials [28].
- Unethical conduct of Clinical trials [26].
- Preclinical and clinical trials results are not similar.
- Preliminary evaluation of drug for their efficacy and safety is necessary.
- Safety and efficacy data analysis to be conducted in more than one animal species [34].
- Requirement of regulatory bodies and setting of policies and regulations.
- Lack of Scientific rationale [28].
Conclusion
Over the years Clinical Trials have improved significantly with the integration of ethics, scientific reasoning, safety measures and drug efficacy. Now the clinical trials are quiet safe as compared to trials conducted earlier. This has imparted expansion of new, safe therapeutic facilities. Dark phase of clinical trials are first step to further new advances in research. The clinical practitioners have learned a lot from the history of Clinical Trials. The tragedies in clinical trials have transformed the behavior of trials. Fruition of new landmarks in clinical researches have permitted better result i.e. rights, safety and well being of human volunteers are protected. Clinical trials are the only pathway to establish safety, therapeutic action of medicines which is not feasible without conducting them. Since these are experiments and despite adequate measures tragedies do occur. Successful Clinical Trials provide benefits to millions after marketing of investigational drugs.
As there is confirmation of safety and effectiveness from preclinical studies, trials are approved by regulatory authorities to proceed further. Trials are a foundation (key stone) for manufacture of novel medicines to cure illness. Trials are necessary for proving the effectiveness and safety of innovated drugs and other process cannot replace trials for drug studies. Tragedies in trials had led to evolution and establishment of various rules and regulations, amendments to the existing regulations.
Acknowledgement
Authors would like to thanks to Baba Farid University of Health Sciences, Faridkot for their technical support.
References
- http://en.wikipedia.org/wiki/Clinical_trial.
- http://www.nlm.nih.gov/medlineplus/clinicaltrials.html.
- https://clinicaltrials.gov/ct2/info/understand.
- Singh H, Srivastva A (2013) Recent Trends in Scope and Opportunity of Clinical Research in India. Indian Journal of Research in Pharmacy and Biotechnology 1(3): 299-304.
- Lasker SP (2013) History of Clinical Research and Ethics. Bangladesh Journal of Bioethics 4(1): 20-29.
- http://www.drugstudy.md/resource6.html.
- http://www.psoriasiscouncil.org/docs/chapter_01.pdf.
- http://www.iupui.edu/~histwhs/G504.dir/irbhist.html.
- Katz RV, Russell SL, Kressin NR, Green BL, Wang MQ, et al. (2006) The Tuskegee Legacy Project: Willingness of Minorities to Participate in Biomedical Research. J Health Care Poor Underserved 17(4): 698-715.
- http://en.wikipedia.org/wiki/Tuskegee_syphilis_experiment.
- http://www.sciencemuseum.org.uk/broughttolife/techniques/tuskegee.aspx.
- Crenner C (2011) The Tuskegee Syphilis Study and the Scientific Concept of Racial Nervous Resistance. J Hist Med Allied Sci 67(2): 244-280.
- http://www.cgu.edu/pages/1722.asp.
- http://en.wikipedia.org/wiki/Belmont_Report.
- http://www.fda.gov/aboutfda/whatwedo/history/productregulation/sulfanilamidedisaster/default.htm.
- http://en.wikipedia.org/wiki/Clinical_trial.http://www.thescientist.com/?articles.view/articleNo/35714/title/The-Elixir-Tragedy--1937/.
- http://www.independent.org/pdf/policy_reports/2010-02-10-fda.pdf.
- Wax PM (1995) Elixirs, Diluents, and the Passage of the 1938 Federal Food, Drug and Cosmetic Act. Ann Intern Med 122(6): 456-461.
- http://en.wikipedia.org/wiki/Nazi_human_experimentation.
- http://www.jewishvirtuallibrary.org/jsource/Judaism/naziexp.html.
- Berger RL (1990) Nazi Science — The Dachau Hypothermia Experiments. N Engl J Med 322(20): 1435-1440.
- http://en.wikipedia.org/wiki/Nuremberg_Code.
- http://en.wikipedia.org/wiki/Guatemala.
- Cuerda E, Lopez-Munoz F (2013) Ethical Considerations of the Human Research: Syphilis Experiments and Denial of Drug Therapy. Clin Exp Pharmacol 3(4): e124.
- Reverby SM (2012) Ethical Failures and History Lessons: The U.S. Public Health Service Research Studies in Tuskegee and Guatemala. Public Health Reviews 34(1): 1-18.
- http://en.wikipedia.org/wiki/Guatemala_syphilis_experiment.
- http://www.thalidomide.ca/the-canadian-tragedy/.
- Moghe VV, Kulkarni U, Parmar UI (2008) Thalidomide. Bombay Hospital Journal 50(3): 472-476.
- https://helix.northwestern.edu/article/thalidomide-tragedy-lessons-drugsafety-and-regulation.
- Thalidomide: http://en.wikipedia.org/wiki/Thalidomide.
- http://www.theguardian.com/society/2012/sep/01/thalidomide-scandaltimeline/.
- Akhurst RJ (2010) Taking thalidomide out of rehab. Nature medicine 16(4): 370-372.
- http://en.wikipedia.org/wiki/Kefauver_Harris_Amendment.
- Kim JH, Scialli AR (2011) Thalidomide: The Tragedy of Birth Defects and the Effective Treatment of Disease. Toxicol Sci 122(1): 1-6.
- http://www.fda.gov/downloads/Drugs/DrugSafety/PostmarketDrugSafety-InformationforPatientsandProviders/UCM222649.pdf.
- http://www.locostindia.com/chapter_4/Drug%20Marketing_10.htm.
- Paul H, Steinbrecher R, Keyek D, Michaels L (2003) Hungary corporations (1st edtn), Zed Books Ltd., UK.
- Meade TW (1975) Subacute myelo-optic neuropathy and Clioquinol. An epidemiological case-history for diagnosis. Br J Prev Soc Med 29(3): 157-169.
- Tateishi J (2000) Subacute myelo-optico-neuropathy: Clioquinol intoxication in humans and animals. Neuropathology 20: S20-24.
- http://newint.org/features/1981/01/01/devils/.
- Mao X, Schimmera AD (2008) The toxicology of Clioquinol. Toxicol Lett 182(1-3): 1-6.
- http://www.drugs.com/accutane.html.
- http://www.acne.org/accutane.html.
- http://www.drugwatch.com/accutane/side-effects.php.
- http://www.drugwatch.com/accutane/.
- Choi JS, Koren G, Nulman I (2013) Pregnancy and isotretinoin therapy. CMAJ 185(5): 411-413.
- http://www.drugbank.ca/drugs/db01186.
- http://www.parkinsoninfo.org/?gclid=CK2Ux4yYucICFQ4pjgod648AHg.
- http://www.fda.gov/Drugs/DrugSafety/DrugSafetyPodcasts/ucm078944.htm.
- http://www.healio.com/endocrinology/neuroendocrinology/news/print/endocrine-today/%7Bd41efd98-9475-4378-b54f-baf86b74281c%7D/pergolide-voluntarily-withdrawn-from-market.
- http://consumer.healthday.com/general-health-information-16/miscdrugs-news-218/parkinson-s-drug-pergolide-withdrawn-over-heart-concerns-603251.html.
- http://en.wikipedia.org/wiki/Pergolide.
- http://www.spacedoc.com/baycol.htm.
- https://www.centerwatch.com/drug-information/fda-approved-drugs/drug/302/baycol-cerivastatin-sodium.
- Psaty BM, Furberg CD, Ray WA, Weiss NS (2004) Potential for conflict of interest in the evaluation of suspected adverse drug reactions: use of Cerivastatin and risk of rhabdomyolysis. JAMA 292(21): 2622-2631.
- http://en.wikipedia.org/wiki/Cerivastatin.
- http://www.webmd.com/cholesterol-management/news/20050322/baycolremoved-from-market.
- http://www.seegerweiss.com/drug-injury/baycol/.
- http://www.consultox.com/toxicology-baycol.shtml.
- http://www.medicinenet.com/script/main/art.asp?articlekey=12814.
- http://en.wikipedia.org/wiki/Troglitazone.
- http://diabeteshealth.com/read/2000/05/01/4832/rezulin-pulled-afterdeath-toll-mounts/.
- https://nfb.org/images/nfb/publications/vod/vsum0003.htm.
- http://www.pulitzer.org/archives/6485.
- http://en.wikipedia.org/wiki/Rapacuronium.
- http://www.nytimes.com/2001/03/31/us/anesthesia-drug-is-removedfrom-market-after-the-deaths-of-5-patients.html.
- http://www.fda.gov/downloads/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/UCM173891.pdf.
- http://en.wikipedia.org/wiki/Rofecoxib.
- http://money.cnn.com/2004/09/30/news/fortune500/merck.
- http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2004/ucm108361.htm.
- http://www.pharmaceutical-journal.com/news-and-analysis/feature/stillfeeling-the-vioxx-pain/20066485.article.
- http://www.streetdirectory.com/etoday/popular-psoriasis-drug-raptivalinked-to-deadly-brain-infection-ucpwfu.html.
- http://en.wikipedia.org/wiki/Efalizumab.
- http://www.webmd.com/skin-problems-and-treatments/psoriasis/news/20081016/psoriasis-drug-raptiva-gets-black-box.
- http://www.fda.gov/downloads/Drugs/DrugSafety/PostmarketDrugSafety-InformationforPatientsandProviders/UCM143346.pdf.
- Gupta SK (2011) Drug Discovery and Clinical Research. (1stedn), Jaypee Brothers Medical Publishers (P) Ltd., New Delhi.
- http://en.wikipedia.org/wiki/Alosetron.
- http://www.ibstales.com/lotronex.htm.
- http://www.nytimes.com/2002/06/08/us/us-lets-drug-tied-to-deaths-backon-market.html.
- Moynihan R (2002) Alosetron: a case study in regulatory capture, or a victory for patients’ rights? BMJ 325(7364): 592–595.
- http://www.drugs.com/lotronex.html.
- Lewis JH (2010) Alosetron for severe diarrhea-predominant irritable bowel syndrome: safety and efficacy in perspective. Expert Rev Gastroenterol Hepatol 4(1): 13-29.
- Pi-Sunyer FX, Aronne LJ, Heshmati HM, Devin J, Rosenstock J (2006) Effect of Rimonabant, a cannabinoid-1 receptor blocker, on weight and cardiometabolic risk factors in overweight or obese patients: RIO-North America: a randomized controlled trial. The Journal of American Medical Association 295(7): 761-775.
- http://en.wikipedia.org/wiki/Rimonabant.
- http://www.bestdietpillreviewsforwomen.com/acomplia-review-side-effects/.>
- http://www.drugs.com/nda/acomplia_060217.html.
- http://www.dietspotlight.com/acomplia-review/.
- http://en.wikipedia.org/wiki/Valdecoxib.
- http://www.medscape.com/viewarticle/502642.
- http://en.wikipedia.org/wiki/Lumiracoxib.
- https://espace.library.uq.edu.au/view/UQ:276187.
- http://en.wikipedia.org/wiki/Sibutramine.
- http://www.medscape.org/viewarticle/730515.
- Scheen AJ (2011) Sibutramine on Cardiovascular Outcome. Diabetes Care34(Suppl 2): S114-S119.
- Greenberg G (2013) Manufacturing Depression: The Secret History of a Modern Disease. Bloomsbury Publishing, New Delhi.
- http://www.aboutbirthdefects.org/zelmid/.
- http://www.nyupress.org/webchapters/0814736696intro.pdf.
- http://www.vivisectionresearch.ca/ch2.htm.
- http://en.wikipedia.org/wiki/Tienilic_acid.
- Neuberger J, Williams R (1989) Immune mechanisms in tienilic acid associated hepatotoxicity. Gut 30(4): 515-519.
- Gentry LO (1991) Review of quinolones in the treatment of infections of the skin and skin structure. J Antimicrob Chemother 28: 97-110.
- Dudley MN (1991) A review of the pharmacokinetic profile of temafloxacin.J Antimicrob Chemother 28: 55-64.
- Finch RG (1993) The Withdrawal of Temafloxacin. Are there implications for other quinolones? Drug Saf 8(1): 9-11.
- http://www.fda.gov/ohrms/dockets/ac/98/briefingbook/1998-3454B1_03_WL49.pdf.
- http://en.wikipedia.org/wiki/Aprotinin.
- http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm142720.htm.
- http://www.lawyersandsettlements.com/articles/drugs-medical/trasylolfraud-00515.html#.VaYlWNKqqko.
- Magana DT, Tudor IC, Dietzel C (2006) The risk associated with aprotininin cardiac surgery. N Engl J Med 354(4): 353–365.
- http://www.rightinginjustice.com/news/2008/05/26/fda-announces-withdrawal-of-remaining-trasylol/.
- http://www.yourlawyer.com/topics/overview/trasylol.
- http://indiatoday.intoday.in/story/drug-trials-kill-10-bhopal-gas-victims/1/129397.html.
- http://www.independent.co.uk/news/world/asia/from-tragedy-to-travestydrugs-tested-on-survivors-of-bhopal-6262412.html.
- http://www.ndtv.com/article/india/illegal-drug-trials-on-victims-of-bhopalgas- tragedy-137952 Illegal drug trials on victims of Bhopal gas tragedy.
- http://ibnlive.in.com/news/12-bhopal-gas-tragedy-victims-die-in-drugtrials/272086-3-236.html.
- http://www.thehindu.com/todays-paper/tp-national/tp-newdelhi/bhopalgas-leakvictims-subjected-to-unethical-clinical-trials/article2345651.ece.
- http://en.wikipedia.org/wiki/TGN1412.
- Suntharalingam G, Perry MR, Ward S, Brett SJ, Castello-Cortes A, et al. (2006) Cytokine Storm in a Phase 1 Trial of the Anti-CD28 Monoclonal Antibody TGN1412. N Engl J Med 355(10): 1018-1028.
- Sandilands GP, Wilson M, Huser C, Jolly L, Sands WA, et al. (2010) Were Monocytes Responsible for Initiating the Cytokine Storm in the TGN1412 Clinical Trial Tragedy? Clin Exp Immunol 162(3): 516-527.
- http://www.outsourcing-pharma.com/Preclinical-Research/Northwicktrial- tragedy-scientists-reveal-how-cytokine-storm-started.
- http://timesofindia.indiatimes.com/india/49-babies-die-during-clinicaltrials-at-AIIMS/articleshow/3374492.cms?referral=PM/.
- http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(12)60855-1/fulltext.
- http://nsnbc.me/2013/05/08/bill-gates-polio-vaccine-program-caused- 47500-cases-of-paralysis-death/.





