Evaluation of Health Related Quality of Life in Patient with Oral Cavity Squamous Cell Carcinoma Receiving Chemotherapy
Mistry CB1*, Rana DS2, Batra V2
1 Department of Pharmacology, Medical College, Baroda, Vadodara, Gujarat, India.
2 Department of Radiotherapy, Medical College, Baroda, Vadodara, Gujarat, India.
*Corresponding Author
Dr. Chirag Mistry M.D,
Department of Pharmacology,
Medical College, Baroda, Vadodara,
Gujarat, India.
E-mail: drchiragm@gmail.com
Article Type: Research Article
Received: May 18, 2015; Accepted: June 25, 2015; Published: June 29, 2015
Citation: Mistry CB, Rana DS, Batra V (2015) Evaluation of Health Related Quality of Life in Patient with Oral Cavity Squamous Cell Carcinoma Receiving Chemotherapy. Int J Clin Pharmacol Toxicol, 4(2) 161-168. doi: dx.doi.org/10.19070/2167-910X-1500028
Copyright: Mistry CB© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: To evaluate impact of chemotherapy on Health Related Quality of Life (HRQOL) in patients of oral cavity squamous cell carcinoma (OCSCC) by analysis of two different treatments named Concurrent Chemo - Radiation (CTRT) and Neo-Adjuvant Chemotherapy (NACT).
Study Design and Instrument: Prospective longitudinal study by evaluation HRQOL by general quality of life (QLQC30) and head & neck specific (QLQ-H&N35) questionnaires of the European Organization for Research and Treatment of Cancer.
Setting: Tertiary care teaching hospital of India.
Participants and Methodology: Patients with histopathologically proven OCSCC were evaluated before starting chemotherapy, after completion of each cycle and one month after completion of full course of chemotherapy. Sequential changes of HRQOL scorings were statistically analyzed by repeated measures ANOVA (P < 0.05) and changes in HRQOL score between CTRT and NACT groups were measured by unpaired t-test (P < 0.05).
Results: As compared to baseline, in both the group there was significant deterioration in HRQOL due to development of sticky saliva, coughing, feeling of illness, requirement of nutritional supplements, social functioning and need of painkillers. As compared to baseline, deterioration of global health status, development of dryness of mouth, sticky saliva, sense problem and trouble with social eating were more significant in CTRT group compared to NACT group, which persisted even at one month follow up (P<0.05).
Conclusion: This study has shown that in patients of oral cavity squamous cell carcinoma, overall baseline HRQOL remained poor, which further deteriorated more in patients receiving CTRT as compared to that of NACT group.
2.Introduction
3.Methodology
3.1.Ethical Clearance
3.2.Study Participants
3.3.Sample Size
3.4.Treatment protocol
3.5.Study instrument
3.6.Prospective longitudinal study design
3.7.Data collection and follow up
3.8.Statistical Analysis
4.Results
4.1.Sociodemographic characteristics
4.2.Assessment of sequential changes in HRQOL score of CTRT or NACT group
4.3.Comparison of HRQOL between CTRT and NACT group
5.Discussion
5.1.Strength and weakness of this study
6.Conclusion
7.Acknowledgement
8.References
Abbreviations
Concurrent Chemo - Radiation (CTRT); Health Related Quality of Life (HRQOL); European Organization for Research and Treatment of Cancer (EORTC); Neo-Adjuvant Chemotherapy (NACT); Oral Cavity Squamous Cell Carcinoma (OCSCC).
Introduction
Carcinoma remains the major cause of morbidity and mortality all over the world and it is the leading cause of death with its relative position varies with age and sex. Oral and oropharyngeal carcinoma are the sixth most common cancers in the world and oral cavity squamous cell carcinoma (OCSCC) constitutes 90 % of all cases of oropharyngeal cancer [1].
The treatment of OCSCC involves chemotherapy with or without surgical resection or adjuvant radiotherapy. Despite of recent advances in diagnosis and treatment, oral cancers have significant impact on patient’s Health Related Quality of Life (HRQOL) due to disfigurement caused by not only the disease itself but also due to adverse reactions caused by treatment [2].
So therapeutic success in management of OCSCC not only should be measured on the basis of a patient’s survival, absence of recurrence or metastasis but also should be based on the patient’s overall quality of life, as increased survival is not necessarily associated with improvement in HRQOL.
According to the WHO, HRQOL has been defined as “an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, standards and concerns. It is a broad ranging concept affected in a complex way by the person’s physical health, psychosocial state, level of independence, social relationships, and their relationships to salient features of their environment” [3].
In developed countries HRQOL measurement is an essential tool for assessment of outcome cancer treatment, but in developing countries like India, it is still in the infancy phase at present [4].
In India, oral cancer represents a major health problem, constituting up to 40% of all cancers and is the most prevalent cancer in males and the third most prevalent cancer in females. In spite of such heavy burden of disease, no such type of study has yet been carried out in patients of OCSCC in India [5, 6].
The European Organization for Research and Treatment (EORTC) introduced Quality of Life Questionnaire 30-QLQ-C30 that
evaluates general aspects of Quality of Life (QOL) associated with various tumors. Another portion of questionnaire named QLQ-H&N35 contains special questions for patients with head and neck tumors. This questionnaire has gained worldwide acceptance, validation and has been translated into different languages [7].
So, in the current study, to evaluate impact of treatment on patients' HRQOL, comparative analysis of the effects of two different treatments named Concurrent Chemo - Radiation (CTRT) and Neo-Adjuvant Chemotherapy (NACT) on HRQOL was done using EORTC given disease specific questionnaires on Indian patients suffering from oral cavity squamous cell carcinoma.
Methodology
The present study was carried out after obtaining permission of local Scientific and Ethical Review Committee (SERC) of a tertiary care teaching hospital of India and ethical principles of biomedical research were followed throughout this study.
All newly diagnosed patients of histopathologically proven cases of OCSCC, who were to receive chemotherapy and agreed to participate in the study at tertiary care teaching hospital of Western India.
All newly diagnosed patients who were to receive chemotherapy with or without radiation therapy for histopathologically proven OCSCC, attending the outpatient department of radiotherapy unit of tertiary care teaching hospital of India, were enrolled in this study.
Patients with age above 18 years, who agreed to give informedwritten consent to participate in the study voluntarily and who were able to communicate with any one of the Indian languages of study instrument, were included in the study.
Following patients were excluded from this study: (1) unwillingness to participate the study (2) taking treatment at other centres (3) diagnosed case of psychiatric illness or cognitive impairment (4) pregnant or nursing mother (5) suffering from terminal illness.
In India, oral cavity cancer constitutes 29.54% among all malignant biopsies and 95% oral cavity carcinoma with squamous cell type. Considering previous records of radiotherapy department, average 15-20 new patients of OCSCC were receiving chemotherapy every month, after using this information for calculating sample size at 5% confidence interval with 95% confidence level, total estimated minimum sample size for this study was 30.
The standard treatment for patients with OCSCC is Concurrent Chemo radiation -CTRT followed by definitive surgery [8,9], while NACT is either given with the intent of achieving: (1) surgical resection for extensive soft tissue disease, oropharyngeal involvement, extensive disease with cartilage erosion or (2) organ preservation for bulky disease with inner cartilage erosion, exolaryngeal disease without cartilage erosion or large N3 nodes [10-13, 16].
In CTRT group, patients were treated with 25-30 fractions of 50 - 60 Gray/day External Beam Radiotherapy for 5-6 weeks, using reducing fields at site of OCSCC with weekly chemotherapy as a radiation sensitizer. For chemotherapy patients were treated with prophylactic Palonosetron, Dexamethasone, Pheniremine Maleate, Mannitol and Hydration with 500 ml Dextrose Noraml Saline (DNS), 5% Dextrose & Ringger’s Lactate (RL), followed by Cisplatin 12 mg/m2 and 5-flurouracil (5 FU) 600 mg/m2 every week for six cycles. Overall event based - HRQOL evaluation of patients of OCSCC was carried out before starting first cycle of chemotherapy (C0), and patients were again evaluated every week after completion of each cycle of chemotherapy at the end of C1,C2,C3,C4,C5,C6 [14]. The last evaluation of HRQOL was done one month after completion of the last cycle of chemotherapy (i.e. C7).
In NACT group, patients were treated with Palonosetron, Dexamethasone, Pheniremine Maleate, Mannitol and Hydration with 500 ml DNS, 5% Dextrose & RL, followed by Neo Adjuvant chemotherapy was given as two (platinum with taxane) or three drug with Platinum, Taxane with 5-flurouracil (5 FU) every 3 week regimen with Cisplatin and Docetaxel as 75 mg/m2 each, 5-FU as 1000 mg/m2. In this group, HRQOL of patients of OCSCC was evaluated before the first cycle of chemotherapy (C0) and patients were evaluated every third week after completion of each cycle of anticancer drugs (e.g. C1,C2,C3,C4). The last evaluation of HRQOL was done one month after completion of the last cycle of chemotherapy (i.e. C5) [15].
Prior permission was taken from the EORTC group for use of their latest (version 3.0) of general Quality of Life QLQ-C30 questionnaire and its Head & Neck Cancer specific QLQ-H&N35 questionnaires, which is validated in various Indian languages.
It consists of 30 questions, out of 30 questions 24 from nine multi-item scales presenting various aspects of HRQOL. It considers five functional scales named physical functioning (PF); social functioning (SF); emotional functioning (EF); role functioning (RF); cognitive functioning (CF). It includes eight symptom scales named fatigue, pain, insomnia, constipation, diarrhea, dyspnoea, appetite loss, nausea and vomiting, single scale of financial difficulty and global health and quality of life [16].
It is disease-specific for patients having cancer of head and neck region. It consists of 35 questions organized in 7 symptoms multiitem scales having 24 questions related to pain, swallowing, sense problem, speech problem, trouble with social eating, trouble with social contact and less sexuality and 11 single-item scales describing different specific concerns of these head and neck cancer patients i.e. teeth problem, opening mouth, dry mouth, sticky saliva, coughing, felt ill, pain killer, nutritional supplement, feeding tube, weight loss and weight gain [16].
Patients were given a HRQOL questionnaire in the vernacular language and patient reported outcome of HRQOL was noted. HRQOL ordinal data were scored as per the developer’s manual and scores were linearly transformed in 0 to 100. They were grouped according to various symptom scales and functional scale [16].
In this observational study, after getting consent, patients’ with OCSCC were enrolled in the study from January 2013 to April 2013, they were divided into CTRT or NACT group as per general health status, willingness for surgical treatment, eligibility for radiotherapy. Consequenty, patients of OCSCC were followed up from January 2013 to September 2013 to evaluate patient reported quality of life.
After enrolment in the study, baseline demographic and clinical data of the patients were recorded. HRQOL was evaluated by providing EORTC QOL C30 and QOL H&N- C35 questionnaires of vernacular language to the patients and they were evaluated before starting chemotherapy, after completion of each cycle of chemotherapy and one month after completion of full course of treatment.
All the patients completed the HRQOL questionnaires, in the presence of the study investigator, who had assisted in case of difficulties in understanding the questions. To maintain patients' compliance, patient or relative was reminded about their next visit by telephonic communication.
Overall, HRQOL was scored as per EORTC developer’s instrucinstructions by linearly converting raw EORTC QLQ-C30 scores into 0 to 100 to facilitate comaprision and readability of overall score.
For global health status and functioning scales, a score of 100 corresponds to a high or best HRQOL. For financial difficulties and the eight symptoms, a score of 100 implies maximum difficulty or symptom burden likewise the worst HRQOL.
On the whole, sequential changes of HRQOL scorings were statistically analyzed using repeated measures ANOVA with post hoc Tukey’s comparisons (P < 0.05). Moreover, changes in HRQOL score between CTRT and NACT groups were measured by unpaired t-test (P < 0.05). All stastical analysis was done by using GraphPad Instat (version 3) software.
In the present study, NACT and CTRT group of patients with OCSCC were evaluated for event based HRQOL analysis, (1) prior to starting chemotherapy - C0, (2) during active treatment period of chemotherapy- i.e. C1, C2, C3, C4, (3) After completing the course of chemotherapy - C4 for NACT and C6 for CTRT group, and (4) one months after completing course of chemotherapy- C5 for NACT and C7 for CTRT group with total sample of 36 patients by using EORTC QOL C-30 and H&N C-35 questionnaires.
At the end of study, patients who were not able to come for follow up at one month after full course of chemotherapy were excluded from analysis. Moreover, effect of two different treatments named CTRT vs. NACT on HRQOL score was analyzed by comparison of difference of HRQOL score between NACT vs. CTRT after completing the course of chemotherapy, and comparison of difference of HRQOL score between NACT vs. CTRT one months after completing course of chemotherapy. HRQOL score was grouped into various symptom scales and functional scales as per developer’s instructions.
As shown in flow chart of Figure 1. out of total 67 enrolled patients, only 36 (53.73%) could complete the whole HRQOL study by follow up at one month after the full course of chemotherapy. On overall comparison of all the patients, who completed the study, all demographic characteristics in both the groups were similar and comparable [Table 1].
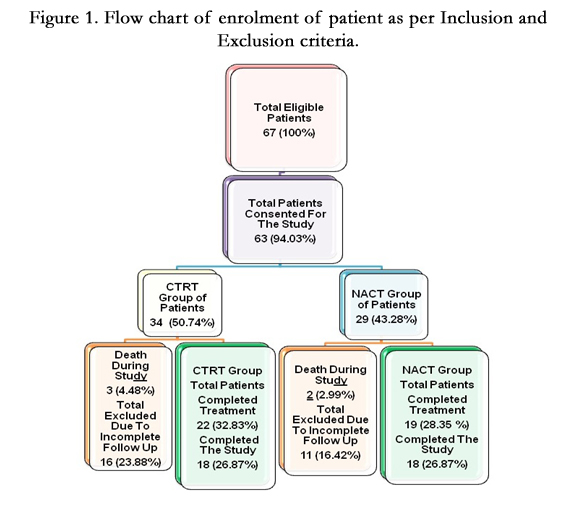
Figure 1. Flow chart of enrolment of patient as per Inclusion and Exclusion criteria.
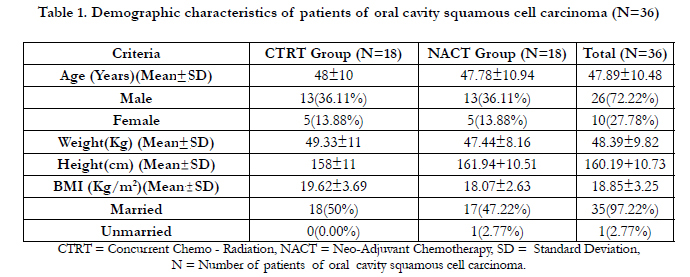

Table 1. Demographic characteristics of patients of oral cavity squamous cell carcinoma (N=36)
On analysis of site of involvement of oral cavity squamous cell carcinoma, the most common site was tongue (38.89%) followed by buccal mucosa (33.33%), palate (13.89%), alveolus (8.33%), retro molar trigone (5.56%) and anterior faucial pillar (2.78%).
In looking towards addiction history of patients, out of 36 patients, the majority of patients (80.56%) had one or more addictions like betel nut chewing, smoking tobacco in the form of bidi (one kind of cigarette) or alcohol consumption.
Majority of patients reported for the chemotherapy during the TNM stage II or III of OCSCC in both CTRT (33.33% or 38.89%) and NACT group (27.78% or 50%) [Table 2].
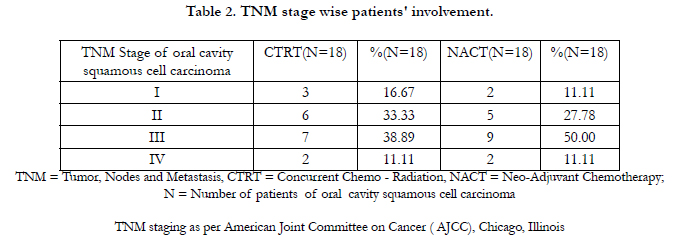
Table 2. TNM stage wise patients' involvement.
In NACT Group of patients, there were significant differences in majority of QLQ- H&N35 scales compared to baseline on each of the multiple-item scales: difference in scales of pain (HNPA; P > 0.10), nausea-vomiting (NV; P > 0.10), diarrhea (DI; P> 0.10), constipation(CO; P = 0.196), insomnia (SL; P = 0.0794), senses problem (HNSE; P > 0.10), swallowing (HNSW; P > 0.10), speech (HNSP; P = 0.0628), teeth (HNTE; P = 0.0617), social eating (HNSO; P >0.10), social contact (HNSC; P=0.054), and sexuality (HNSX; P>0.10) were not significant.
On analysis of the 11 single-item scales, there were significant differences on the coughing scale (HNCO; P = 0.0002), sticky saliva (HNSS; P = 0.02), feeling of illness (HNFI; P<0.0001), requirement of nutritional supplements (HNNU; P = 0.0002), and painkillers (HNPK; P = 0.0062) [Figure 2. A-F]. On the other hand, difference in score of opening mouth (HNOM; P = 0.752), requirement of feeding tube (HNFE, P > 0.10), dryness of mouth (HNDR; P > 0.10), and weight loss (HNWL; P > 0.10) were not significant. On the other hand, no differences emerged on the single-item scale of weight gain (HNWG).
On evaluation of HRQOL by using the core questionnaire (QLQ-C30), in NACT group of patients, on each of these scales, patients had reported poorer baseline functioning at presentation of disease, which persisted till one month after completion of full course of treatment. Overall, difference in scales on the physical functioning (P > 0.10), role functioning (P > 0.10), emotional functioning scale (P > 0.10), global quality of life (P > 0.10), cognitive functioning (P > 0.10), appetite (P > 0.10), financial difficulty (P > 0.10), and fatigue (P > 0.10) scales were not significant, while there was a statistically significant difference in social functioning (P = 0.0488) at the end of one month after completion of full course of treatment [Figure 2. A-F].
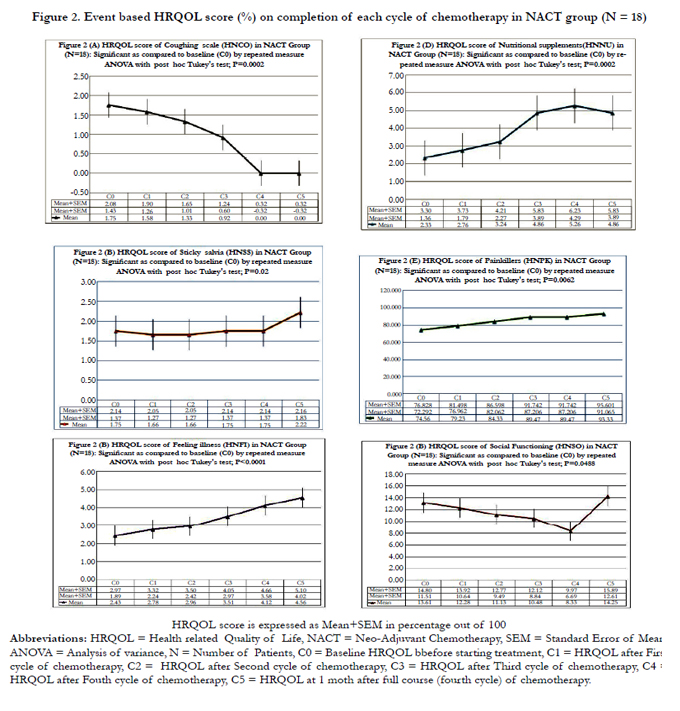
Figure 2. Event based HRQOL score (%) on completion of each cycle of chemotherapy in NACT group (N = 18)
In CTRT group of patients, evaluation of HRQOL by using the core questionnaire (QLQ- H&N35), cancer patients had reported poorer functioning at presentation of disease on each of these scales, which persisted till one month after completion of full course of treatment likewise scales of Pain (HNPA; P > 0.10), senses problem (HNSE; P > 0.10), teeth (HNTE; P > 0.10), insomnia (SL; P > 0.10), swallowing (HNSW; P > 0.10), speech (HNSP; P >0.10), social eating (HNSO; P > 0.10), social contact (HNSC; P > 0.10), and sexual function (HNSX; P>0.10). On the other hand, development of complaints of nausea-vomiting (NV; > 0.10), diarrhea (DI; P= 0.0813) or constipation (CO; P > 0.10) remained persistent during the course of treatment.
On evaluation of the 11 single-item scales, there was a significant difference on the opening mouth (HNOM; P= 0.004), sticky saliva (HNSS; P = 0.02), dry mouth (HNDR; P<0.0001), coughing (HNCO; P = 0.0002), feeling of illness (HNFI; P<0.0001), requirement of nutritional supplements (HNNU; P <0.0001) and painkillers (HNPK; P<0.0001), while score of and weight loss (HNWL; P >0.10) was not significant. On the other hand, no differences emerged on the single-item scale of requirement of feeding tube (HNFE) and weight gain (HNWG) [Figure 3. A-H].
On analysis of HRQOL by using the core questionnaire (QLQC30) in CTRT group of patients, on each of these scales, cancer patients had reported poorer functioning at presentation of disease, which persisted till one month after completion of full course of treatment. Overall, difference in scales on the pain (PA; P > 0.10), physical functioning (PF2; P > 0.10), social functioning (SF; P > 0.10), role functioning (RF2; P = 0.0901), emotional functioning scale (EF; P > 0.10), global quality of life (QL2; P>0.10), cognitive functioning (CF; P > 0.10), appetite loss (AP; P >0.10), financial difficulty (FI; P > 0.10), and fatigue (P = 0.0663) scales, were non significant, while there was a significant improvement in the dyspnoea score (DY; P= 0.0044) at the end of one month after completion of full course of treatment [Figure 3. A-H].
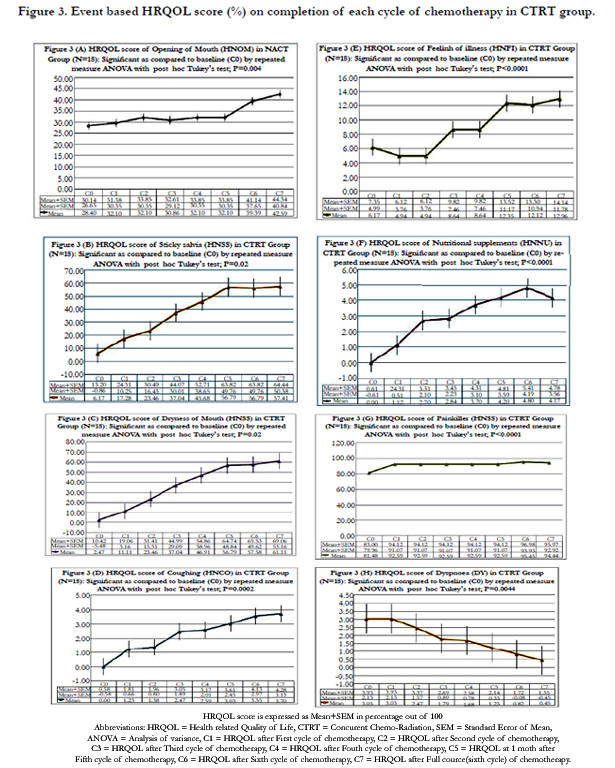
Figure 3. Event based HRQOL score (%) on completion of each cycle of chemotherapy in CTRT group.
On comparison of HRQOL score between CTRT and NACT group, by looking towards overall treatment outcome analysis as compared to baseline (C0), at the end of a full course of therapy, deterioration of global health status and development of dryness of mouth, sticky saliva, sense problem and trouble with social eating were more significant in CTRT group compared to NACT group (P<0.05) [Figure 4].
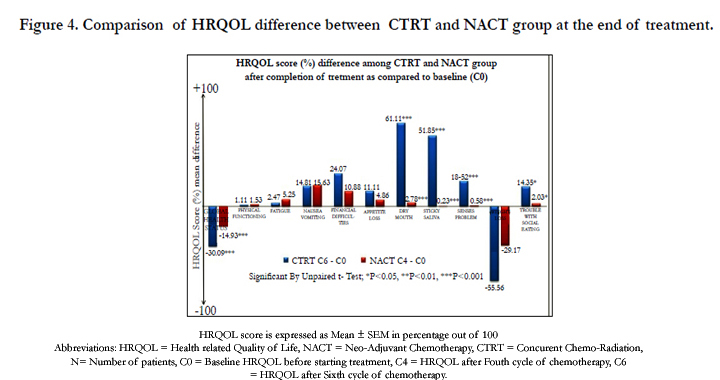
Figure 4. Comparison of HRQOL difference between CTRT and NACT group at the end of treatment
Discussion
On the whole, many studies dealing with QoL in head and neck cancer have been based on heterogeneous groups of patients with respect to different site and stage of tumour. Only a few prospective studies have focused on a specific anatomic site and type like oral cavity squamous cell carcinoma [17].
This study is one of the first to examine the HRQOL by using the new EORTC QLQ-H&N35 module in Indian patients with Oral cavity squamous cell carcinoma. As instruments of EORTC questionnaires showed good internal consistency compared to existing alternative tools, their instrument is preferred and selected over other available tools [18]. Moreover, reliability in the form of external and internal validity has already been established by various previous studies, so it gives consistent result on follow up [19].
In this observational study, all enrolled patients were inhabitant of western India. And the majority of patients of OCSCC presented during the fourth or fifth decade of life, which is similar to the findings that observed by Shenoi P et al. and Sankaranarayana et al [7, 20].
Out of all patients of the OCSCC, majority of the patients were male and they were farmer by occupation, which is aligned with Indian demographic data suggestive of male predominance for development of oral cancer [21]. In addition to that, more than half of the patients with OCSCC presented during advanced TNM stage of the disease, which is similar to Indian patients’presentation at outpatient department [22].
According to previous Indian study, oral or mouth cancer most commonly involves the tongue, which may also occur on the floor of the mouth, cheek lining, gingiva (gums), lips, palate (roof of the mouth), maxilla or mandible. Similar findings were observed in this study as majority of patients presented with OCSCC of anterior 2/3rd of tongue, followed by buccal mucosa, palate, alveolus, retro molar trigone and anterior faucial pillar [23].
On event based follow up for analysis of HRQOL, development of complaints of nausea, vomiting, feeling of illness, weight loss, fatigue, impaired socialization (decrease in involvement of social activity or eating in the presence of relatives), requirement of nutritional supplements and painkillers were progressive compared to baseline in both the treatment groups, which were related to disease itself or adverse reaction due to chemotherapy or radiotherapy in both the CTRT and NACT groups.
As compared to NACT group, patients of CTRT group had developed more deterioration in global health status, dryness of mouth, sticky saliva, persistent coughing, and sensory problems after complete course of chemotherapy treatment, which persisted even at one month follow up. These findings were similar to Brazilian study, which showed that worsening of HRQOL after diagnosis and treatment was more among patients treated with radiotherapy [24].
In CTRT group, the opening of mouth and chewing function was compromised at presentation and further deteriorated during follow up study. Likewise, many authors previously stressed that opening of mouth was compromised due to submucous fibrosis, mandibular reconstruction by bony free flaps, and osteo-integrated dental rehabilitation. In fact, dental status and prosthetic rehabilitation before radiation treatment play only a partial role in chewing ability. Moreover, in advanced cancers of the retromolar trigone extending to the tonsillar region, resection of the pterygoidmuscles always leads to heavy trismus that, in many cases, is irreversible and extremely invalidating [25].
On sequential evaluation of HRQOL score, there was deterioration in most of the HRQOL score, while in CTRT group; there was improvement of dyspnoea on overall analysis. HRQOL score of development of dyspnoea had decreased compared to baseline, which may be attributed to shrinkage of tumour, decreased secretions and clearance of blockage of upper respiratory tract by Concurrent Chemoradiation.
Overall, more deterioration of Global Quality of Life in CTRT group as compared to NACT group can be due to development of mucositis which is characterised by dryness of mouth, sticky saliva, sense problem and trouble with social eating in CTRT group. In this perspective, few authors of previous studies have focused on residual tongue mobility, a factor which in terms of functional outcome of eating disability is much more crucial than the amount of preserved tongue [25].
In short, statistical significant score of HRQOL need to be correlated with clinical scenario. However, many previous studies failed to identify a statistically significant relationship between clinical parameters and functional outcomes, probably on account of the cross-sectional design and grouping of different head and neck sites and treatment modalities [25].
This study was focused on oral cavity, so a study on a single region can give more robust result compared to generalised study including more number of sites of head and neck cancer. Moreover, evaluation of HRQOL in vernacular language was able to make patients aware about early signs of progression of cancer and adverse drug reactions which can help them to approach healthcare facility on early basis.
On the other hand, patients with advanced stage of cancer could not survive longer or lost to follow up due to multiple reasons, so their HRQOL could not be evaluated. Consequently, this study was limited by the small sample of patients completing questionnaires at one month after full course of chemotherapy, which can be extended for more duration with involvement of multiple centres.
Conclusion
This study demonstrated that in patients of oral cavity squamous cell carcinoma, overall baseline HRQOL remained poor, which further deteriorated more in patients receiving CTRT as compared to that of NACT group.
Overall, more deterioration of Global Quality of Life in Concurrent Chemo-Radiation (CTRT) group as compared to Neo-Adjuvant Chemotherapy (NACT) group was detected due to significant development of dryness of mouth, sticky saliva, sense problem and trouble with social eating in CTRT group of patients.
Acknowledgement
We are very much grateful to the European Organization for Research and Treatment of Cancer Group of Brussels, Belgium and for giving permission to carry out study by using HRQOL study questionnaires. Moreover, I would also like to extend my acknowledgement to Dr. N. A. Trivedi, Dr. J. D. Bhatt, Dr.Vikas Doshi and team of clinical staff for assistance during initial phases of this study. In the same way, I express my sincere and deepest gratitude towards study participants.
References
- Warnakulasuriya S (2009) Global epidemiology of oral and oropharyngeal cancer. Oral Oncology 45(4): 309-316.
- Dietz A, Meyer A, Singer S (2009) Quality of life measures in patients with head and neck malignancies. Current status and future requirements. HNO 57(9): 857-865.
- WHO (1993) Rehabilitation after cardiovascular diseases, with special emphasis on developing countries. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser 831: 1–122.
- Rogers SN, Ahad SA, Murphy AP (2007) A structured review and theme analysis of papers published on ‘quality of life’ in head and neck cancer: 2000-2005. Oral Oncol 43(9): 843-868.
- Shenoi R, Devrukhkar V, Chaudhuri, Sharma BK, Sapre SB, et al. (2012) Demographic and clinical profile of oral squamous cell carcinoma patients: A retrospective study. Indian J Cancer 49(1): 21-26.
- Sharma P, Saxena S, Aggarwal P (2010) Trends in the epidemiology of oral squamous cell carcinoma in Western UP: An institutional study. Indian J Dent Res 21(3): 316-319.
- Bjordal K, de Graeff A, Fayers PM, Hammerlid E, van Pottelsberghe C, et al. (2000) A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group. Eur J Cancer 36(14): 1796-1807.
- Grégoire V, Lefebvre JL, Licitra L, Felip E (2010) Squamous cell carcinoma of the head and neck: EHNS-ESMO-ESTRO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 21(suppl 5): 184-186.
- Baxi S, Fury M, Ganly I, Rao S, Pfister DG (2012) Ten years of progress in head and neck cancers. J Natl Compr Canc Netw 10(7): 806-810.
- Paccagnella A, Orlando A, Marchiori C, Zorat PL, Cavaniglia G, et al. (1994) Phase III trial of initial chemotherapy in stage III or IV head and neck cancers: A study by the gruppo di studio sui tumori della testa e del collo. J Natl Cancer Inst 86(4): 265-272.
- Posner MR, Hershock DM, Blajman CR, Mickiewicz E, Winquist E, et al. (2007) Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N Engl J Med 357(17): 1705-1715.
- Vermorken JB, Remenar E, van Herpen C, Gorlia T, Mesia R, et al. (2007) Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N Engl J Med 357(17): 1695-1704.
- Haddad R, O′Neill A, Rabinowits G, Tishler R, Khuri F, et al. (2013) Induction chemotherapy followed by concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): A randomised phase 3 trial. Lancet Oncol 14(3): 257-264.
- Seiwert TY, Salama JK, Vokes EE (2007) The chemoradiation paradigm in head and neck cancer. Nat Clin Pract Oncol 4(3): 156-171.
- Agarwal JP, Chaturvedi P, Chaukar D, Joshi P, Patil V, et al. (2013) Neoadjuvant chemotherapy in advanced hypopharyngeal carcinoma. Indian J Cancer 50(1): 25-30.
- The European Organisation For Research And Treatment Of Cancer (2012) Available from: http://www.eortc.org.
- Deleyiannis FW, Weymuller EA, Coltrera MD (1997) Quality of life in disease-free survivors of advanced (stage III or IV) oropharyngeal cancer. Head Neck 19(6): 466-473.
- Silveira AP, Goncalves J, Sequeira T, Ribeiro C, Lopes C, et al. (2010) Patient reported outcomes in head and neck cancer: selecting instruments for quality of life integration in clinical protocols. Head Neck Oncol 31: 2-32.
- Sherman AC, Simonton S, Adams DC, Vural E, Owens B, et al. (2000) Assessing quality of life in patients with head and neck cancer: cross-validation of the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Head and Neck module (QLQ-H&N35). Arch Otolaryngol Head Neck Surg 126(4): 459-467.
- Sankaranarayanan R, Mohideen MN, Nair MK (1989) Aetiology of oral cancer in patients less than or equal to 30 years of age. Br J Cancer 59(3): 439-440.
- Almodovar J, Perez SI, Arruza M, Morell CA, Baez A (1996) Descriptive epidemiology of head and neck squamous cell carcinoma in Puerto Ricans. P R Health Sci J 15(4): 251-255.
- Kerdpon D, Sriplung H (2001) Factors related to delay in diagnosis of oral squamous cell carcinoma in southern Thailand. Oral Oncol 37(2): 127-131.
- Khan Z (2012) An Overview of Oral Cancer in Indian Subcontinent and Recommendations to Decrease its Incidence. WebmedCentral CANCER 3:6.
- Prasad A, Datta PP, Bhattacharya J, Pattanayak C, Chauhan AS, et al. (2013) Pattern of Adverse Drug Reactions Due to Cancer Chemotherapy in a Tertiary Care Teaching Hospital in Eastern India. J Pharmacovigilance 1(2): 107.
- Villaret AB, Cappiello J, Piazza C, Pedruzzi B, Nicolai P (2008) Quality of life in patients treated for cancer of the oral cavity requiring reconstruction: a prospective study. ACTA Otorhinolaryngol Ital 28(3): 120-125.





