A Possible Association of Sex Hormone-Binding Globulin with Weight Gain in the Valproic Acid-Treated Female Patients with Epilepsy
Saruwatari J1*, Uchiyashiki Y1, Kajiwara A1, Noai M1, Tanamachi Y1, Soraoka H1, Deguchi M1, Oniki K1, Yasui-Furukori N2, Kaneko S2, Ishitsu T3,4, Nakagawa K1,5
1 Division of Pharmacology and Therapeutics, Graduate School of Pharmaceutical Sciences, Kumamoto University, 5-1 Oe-honmachi, Chuo-ku, Kumamoto 862-0973, Japan.
2 Department of Neuropsychiatry, Hirosaki University School of Medicine, 5 Zaifu, Hirosaki 036-8562, Japan.
3 Kumamoto Saishunso National Hospital, 2659 Suya, Koshi, Japan.
4 Kumamoto Ezuko Ryoiku Iryo Center, 575 Shigedomi, Ezumachi, Higashi-ku, Kumamoto 862-0947, Japan.
5 Center for Clinical Pharmaceutical Sciences, Kumamoto University, 5-1 Oe-honmachi, Chuo-ku, Kumamoto 862-0973, Japan.
*Corresponding Author
Junji Saruwatari,
Division of Pharmacology and Therapeutics,
Graduate School of Pharmaceutical Sciences,
Kumamoto University,
5-1 Oe-honmachi, Chuo-ku,Kumamoto 862-0973, Japan.
E-mail: junsaru@gpo.kumamoto-u.ac.jp
Article Type: Research Article
Received: May 28, 2014; Accepted: June 20, 2014; Published: June 23, 2014
Citation: Saruwatari J, et al., (2014) A possible Association of Sex Hormone-Biding Globulin with Weight Gain in the Valproic Acid-Treated Female Patients with Epilepsy. Int J Clin Pharmacol Toxicol. 3(1), 106- 110. doi: dx.doi.org/10.19070/2167-910X-1400020
Copyright: Junji Saruwatari© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Weight gain is a common adverse consequence of treatment with valproic acid. Although a low sex hormone-binding globulin (SHBG) level was shown to be an independent risk factor for the development of metabolic syndrome and type 2 diabetes in the general population, there is presently no data available regarding the association between the SHBG level and valproic acid-induced weight gain. The association between the plasma SHBG level and being overweight was retrospectively investigated in 46 valproic acid-treated and 59 carbamazepine-treated patients with epilepsy. Among the female patients treated with valproic acid, the plasma SHBG levels tended to be negatively correlated with the gap between the body mass index value for each patient and the upper limit of the normal range (adjusted partial regression coefficient = -6.86, P = 0.041), and the SHBG levels were significantly lower in the overweight subjects than in the normal weight subjects (P = 0.001). These associations were not observed among the valproic acid-treated male patients or the carbamazepine-treated male and female patients. The plasma SHBG levels may be therefore associated with being overweight in the valproic acid-treated female patients.
2.Introduction
3.Materials and Methods
4.Results
5.Discussions
6.Acknowledgments
7.References
Keywords
Valproic Acid; Overweight; Sex Hormone-Binding Globulin; Weight Gain.
Introduction
Valproic acid (VPA) is one of the most widely prescribed antiepileptic drugs worldwide [1]. Treatment with VPA has been associated with metabolic and endocrine disorders, such as weight gain and hyperinsulinemia, which may contribute to the cardiovascular risk observed in patients with epilepsy [2-5]. Additionally, VPA can alter the levels of sex hormones in both males and females, and it is associated with reproductive endocrine disorders [1,4,6].
The pathogenic mechanisms underlying the VPA-induced weight gain are still unclear [4,5,7]. Gender may be considered to be one of the risk factors for VPA-induced weight gain [4,5], because the results from clinical studies have suggested that the occurrence of weight gain is more prevalent in VPA-treated female patients with epilepsy, especially in post-pubertal females, compared with the male patients [4,5]. It has also been suggested that VPA-induced weight gain is associated with polycystic ovary syndrome [1,4,6].
Sex hormone-binding globulin (SHBG) is a glycated homodimeric plasma transport protein that binds testosterone with a higher affinity than estradiol [8-10]. An emerging understanding of the complexity of SHBG synthesis and physiology has led to renewed interest in the potential role of the protein in a wide range of clinical disorders, including metabolic syndrome and type 2 diabetes [8-10]. However, there is presently no data available regarding the association between the VPA-induced weight gain and the SHBG level.
This study aimed to determine whether the SHBG level is associated with being overweight in the VPA-treated patients with epilepsy.
Materials and Methods
A cross-sectional, case-control analysis was conducted in 46 VPAtreated and 59 age- and sex-matched carbamazepine (CBZ)-treated Japanese patients with epilepsy, who had received VPA or CBZ therapy for over one month at Kumamoto Saishunso National Hospital between May 1989 and July 2011. The demographic and clinical information were obtained retrospectively from the medical records. The institutional ethics committees approved this study. All of the patients provided their written informed consent to participate in the study.
The heights and weights of the subjects were measured, and the body mass index (BMI) was calculated. Overweight was diagnosed as a BMI ≥ 25 kg/m2 in the adult patients. When the patient age was 18 or under, the international BMI cut-offs for child overweight [11] were used for the diagnosis. Since the BMI in childhood changes substantially with age [11], we determined the BMI gap in each patient using the following equation: BMI gap = patient’s BMI value ─ cutoff value for overweight (e.g., BMI of 25 kg/m2 for adults). Blood samples were collected for clinical laboratory tests, which were performed regularly.
The human SHBG Quantikine ELISA kit (R&D Systems, Inc. Minneapolis, USA) was used to measure the plasma concentrations of SHBG with an enzyme-linked immunosorbent assay using 10 μL plasma samples. The measurements were obtained in accordance with the manufacturer’s protocol. The lower limit of quantification was 0.002 nmol/L and the within- and between-day coefficients of variation for determining the SHBG levels were < 5%.
The associations of the plasma SHBG levels with the BMI gaps were determined using a multiple linear regression model, with an adjusted partial regression coefficient (B) and an adjusted coefficient of determination (R2), incorporating the patient age, sex, dose and duration of VPA or CBZ therapy, and the co-administration of antiepileptic drugs that can alter the body weight (i.e. clobazam, gabapentin, topiramate, zonisamide) as covariates, separately in the patients treated with VPA and CBZ (as reference). The interaction between the plasma SHBG levels and sex was also included as a covariate, because the SHBG levels were reported to be affected by the sex of the subject [10,12]. The data on the SHBG levels were converted into log10 values to ensure the normality of distribution before the multiple linear regression model was employed. The other data are presented as the medians (range) or the numbers (%). The continuous and categorical variables were compared by the Mann-Whitney U-test and Fisher’s exact test, respectively. A P-value < 0.05 was considered to be statistically significant. Multiple comparisons were corrected using Bonferroni's method, and P-values < 0.05/n were considered to be statistically significant after correcting for the number of comparisons made. These statistical analyses were performed using the SPSS software package (version 17.0, IBM Japan Ltd, Tokyo, Japan). The statistical power of the associations between the plasma SHBG levels and the BMI gaps was calculated at a significance (alpha) level of 0.05 (two-tailed) based on the sample size of this study and the observed effect size (i.e. R2) using the SPSS SamplePower software program (version 3.0; IBM Japan Ltd).
Results
Among the study population, 12 and 14 patients of the patients treated with VPA and CBZ, respectively, were overweight. In the multiple regression analysis, a significant interactive effect of the SHBG levels and the sex on the BMI gap was observed among the VPA-treated patients (P = 0.008). Therefore, we determined the effects of the SHBG levels separately based on the sex of the subject (Table 1). In the VPA-treated female patients, the SHBG levels tended to be negatively correlated with the BMI gap, whereas this association was not observed in the VPA-treated male patients (Table 1). Table 2 shows the patients’ characteristics and the differences in the SHBG levels between overweight and normal weight patients separately in the VPA-treated male and female patients. Among the VPA-treated female patients, the SHBG levels were significantly lower in the overweight subjects than in the normal weight subjects (Table 2). None of the patient characteristics were significantly different between the overweight and normal weight subjects regardless of sex, except for the body weight, BMI, BMI gap, duration of VPA therapy, γ-glutamyltransferase level and co-administration of gabapentin (Table 2).
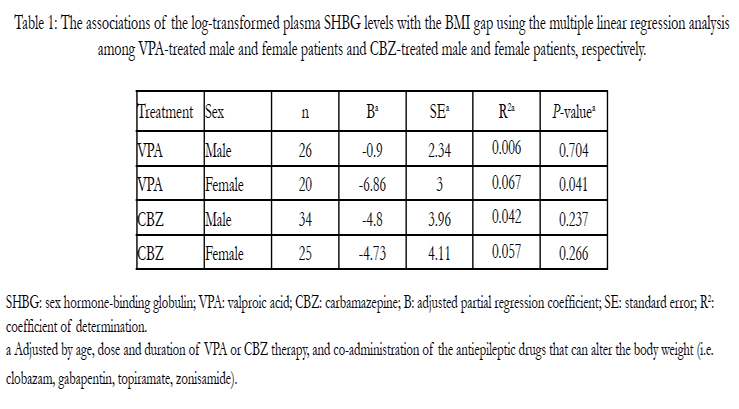

Table 1: The associations of the log-transformed plasma SHBG levels with the BMI gap using the multiple linear regression analysis among VPA-treated male and female patients and CBZ-treated male and female patients, respectively.
SHBG: sex hormone-binding globulin; VPA: valproic acid; CBZ: carbamazepine; B: adjusted partial regression coefficient; SE: standard error; R2:coefficient of determination. a Adjusted by age, dose and duration of VPA or CBZ therapy, and co-administration of the antiepileptic drugs that can alter the body weight (i.e. clobazam, gabapentin, topiramate, zonisamide).
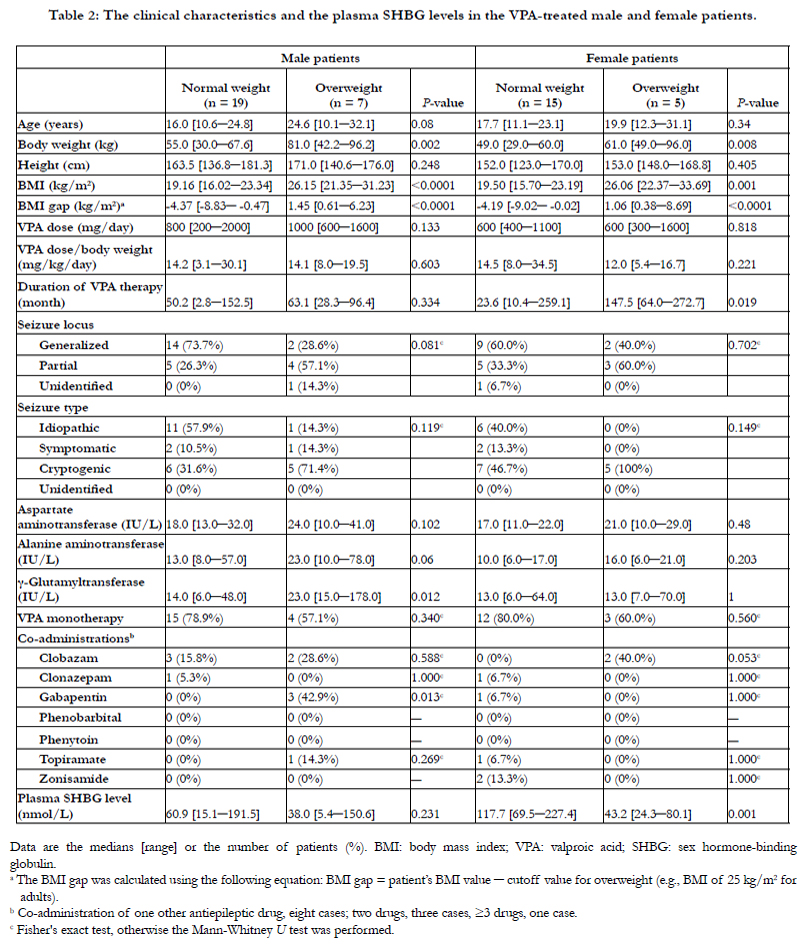
Table 2: The clinical characteristics and the plasma SHBG levels in the VPA-treated male and female patients.
Data are the medians [range] or the number of patients (%). BMI: body mass index; VPA: valproic acid; SHBG: sex hormone-binding globulin.
a The BMI gap was calculated using the following equation: BMI gap = patient’s BMI value ─ cutoff value for overweight (e.g., BMI of 25 kg/m2 for adults).
b Co-administration of one other antiepileptic drug, eight cases; two drugs, three cases, ≥3 drugs, one case.
c Fisher's exact test, otherwise the Mann-Whitney U test was performed.
To compare the results in VPA-treated patients, we assessed the presence of any associations between the SHBG levels and the BMI gap separately in CBZ-treated male and female patients, but there were no associations among these patient groups (Table 1 and Table 3).
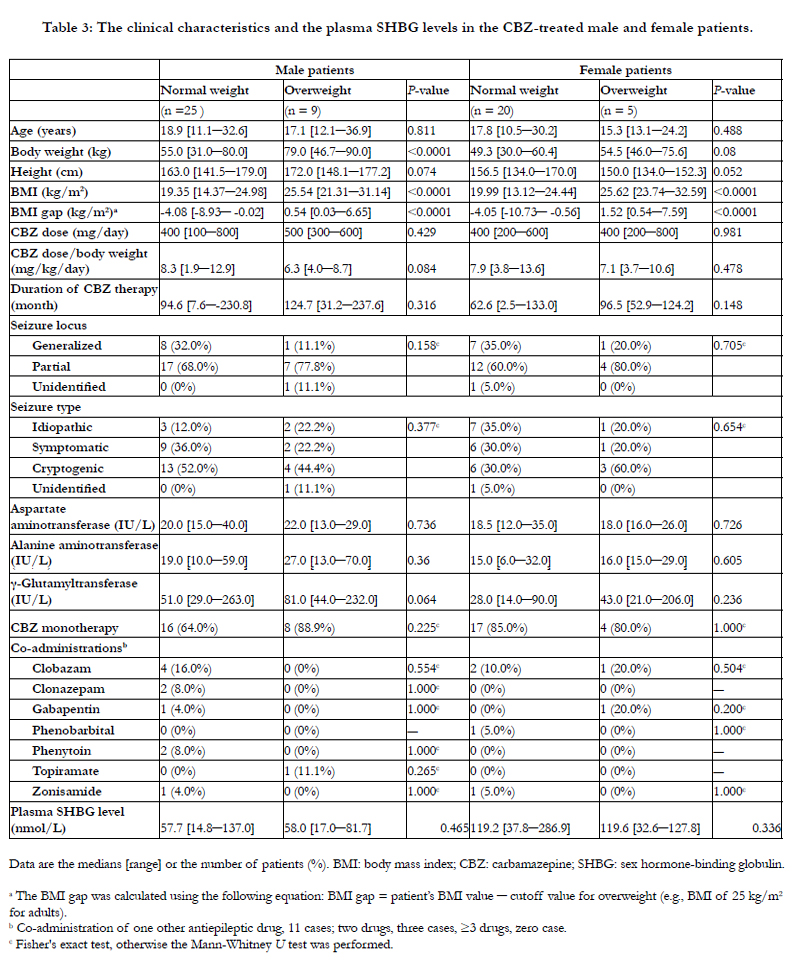
Table 3: The clinical characteristics and the plasma SHBG levels in the CBZ-treated male and female patients.
Data are the medians [range] or the number of patients (%). BMI: body mass index; CBZ: carbamazepine; SHBG: sex hormone-binding globulin.
a The BMI gap was calculated using the following equation: BMI gap = patient’s BMI value ─ cutoff value for overweight (e.g., BMI of 25 kg/m2 for adults).
b Co-administration of one other antiepileptic drug, 11 cases; two drugs, three cases, ≥3 drugs, zero case.
c Fisher's exact test, otherwise the Mann-Whitney U test was performed.
When the magnitude of the effect size was fixed at the observed R2 values (Table 1), the predicted statistical power of the associations between the plasma SHBG levels and the BMI gaps was 6.7%, 58%, 23% and 20% in 26 VPA-treated males, 20 VPA-treated females, 34 CBZ-treated males and 25 CBZ-treated females with epilepsy, respectively.
Discussions
To the best of our knowledge, this is the first report to show that low plasma SHBG levels may be associated with overweight status in VPA-treated female patients with epilepsy.
The mechanism underlying the VPA-induced weight gain is matter of discussion, and various hypotheses have been proposed to explain the effects of VPA on the weight increase. There have included dysregulation of the hypothalamic system and effects on insulin resistance [4,5]. It is known that the treatment with VPA disrupts the hypothalamo-hypophyseal-gonadal axis in female rats [13], and it has also been reported that VPA-treated epileptic patients who reported weight gain developed increased appetite and frequently consumed calorie-rich beverages [4,5,14,15]. On the other hand, it has been suggested that hyperinsulinemia in obese patients taking VPA is not only a consequence of the insulin resistance induced by weight gain, but that the development of insulin resistance may be one of the factors leading to weight gain in some patients [4,5]. It has been reported that weight gain during VPA treatment is related to increase in insulin concurrent with a decrease in the glucose level, which can stimulate appetite and may cause weight gain [4,5,16]. Additionally, VPA is reported to have effects on the adipokines released by adipose tissue, such as leptin [4,5]. The VPA-related obesity was also previously reported to be associated with elevated serum leptin levels in female patients with epilepsy [4-6][15,17].
Recently, a low SHBG level was shown to be an independent risk factor for the development of metabolic syndrome and type 2 diabetes in the general population [8,9]. A previous study of healthy midlife females reported that lower blood SHBG levels were associated with higher leptin levels, independent of the fat mass and insulin resistance, suggesting that SHBG may regulate the adipose tissue hormones [18]. It has also been reported that the association between SHBG and insulin resistance was stronger in aging females than in the males [9,19]. Therefore, we speculate that the low plasma SHBG levels may be associated with the hyperleptinemia and/or insulin resistance in the VPA-treated female patients, thus resulting in the associations with the VPA-induced weight gain
This investigation has some potential limitations. First, because we separated the subjects by sex due to the observation of interactive effects of the SHBG level and the sex on the BMI gap, the sample size of each group was small. When we calculated the statistical power of the associations between the plasma SHBG levels and the BMI gaps based on the sample size of this study and the observed effect size (i.e. R2), the values of the predicted power were small, because the magnitude of the observed effect size was extremely small, especially for the negative findings. Therefore, the presence of a type 2 error might not be excluded. Second, the influence of the duration and dose of VPA or CBZ therapy, the age, sex, seizure locus, seizure type, seizure control and concomitant use of antiepileptic drugs, including the previous antiepileptic drugs that the patients had used, on the BMI gap may not have been fully excluded, even though we adjusted for several potential confounding factors in the analyses. Regarding age, it has been reported that pre-pubertal males had significantly higher SHBG levels compared with similar-aged pre-pubertal females, and the SHBG levels declined with age in both sexes [10,12]. Third, because we could not obtain any data about the SHBG level before VPA therapy in the present study, we could not clarify whether the association between being overweight and a low SHBG level existed prior to the use of VPA. Finally, since we did not include healthy controls, we could not compare the findings of this study with the relationships between the SHBG level and the weight status in non-epileptic subjects. Despite these limitations, we herein provided the first evidence that low plasma SHBG levels may be associated with being overweight in VPA-treated female patients with epilepsy. Further longitudinal investigations in larger populations, and studies showing pathophysiological evidence are needed to verify this finding.
Acknowledgments
This work was supported by grants from the Japan Research Foundation for Clinical Pharmacology and KAKENHI (23510348,24590652, 25860117), and in part by a grant from the Smoking Research Foundation.References
- Nanau RM, Neuman MG (2013) Adverse drug reactions induced by valproic acid. Clin Biochem 46:1323-1338.
- Verrotti A, Manco R, Agostinelli S, Coppola G, Chiarelli F (2010) The metabolic syndrome in overweight epileptic patients treated with valproic acid. Epilepsia 51:268-273.
- Verrotti A, Agostinelli S, Parisi P, Chiarelli F, Coppola G (2011) Nonalcoholic fatty liver disease in adolescents receiving valproic acid. Epilepsy & Behavior 20:382-385.
- Verrotti A, D'Egidio C, Mohn A, Coppola G, Chiarelli F (2011) Weight gain following treatment with valproic acid: pathogenetic mechanisms and clinical implications. Obes Rev 12:e32-43.
- Belcastro V, D'Egidio C, Striano P, Verrotti A (2013) Metabolic and endocrine effects of valproic acid chronic treatment. Epilepsy Research 107:1-8.
- Verrotti A, D'Egidio C, Mohn A, Coppola G, Parisi P, et al. (2011) Antiepileptic drugs, sex hormones, and PCOS. Epilepsia 52:199-211.
- Rauchenzauner M, Laimer M, Wiedmann M, Tschoner A, Salzmann K, et al. (2013) The novel insulin resistance parameters RBP4 and GLP-1 in patients treated with valproic acid: just a sidestep? Epilepsy Research 104:285-288.
- Le TN, Nestler JE, Strauss JF 3rd, Wickham EP 3rd (2012) Sex hormonebinding globulin and type 2 diabetes mellitus. Trends in Endocrinology & Metabolism 23:32-40.
- Wallace IR, McKinley MC, Bell PM, Hunter SJ (2013) Sex hormone binding globulin and insulin resistance. Clin Endocrinol (Oxf ) 78:321-329.
- Hammond GL, Wu TS, Simard M (2012) Evolving utility of sex hormonebinding globulin measurements in clinical medicine. Curr Opin Endocrinol Diabetes Obes 19:183-189.
- Cole TJ, Bellizzi MC, Flegal KM, Dietz WH (2000) Establishing a standard definition for child overweight and obesity worldwide: international survey. British Medical Journal 320:1240-1243.
- Sorensen K, Andersson AM, Skakkebaek NE, Juul A (2007) Serum sex hormone- binding globulin levels in healthy children and girls with precocious puberty before and during gonadotropin-releasing hormone agonist treatment. J Clin Endocrinol Metab 92:3189-3196.
- Lakhanpal D, Kaur G (2007) Valproic acid alters GnRH-GABA interactions in cycling female rats. Cellular and molecular neurobiology 27:1069-1083.
- Isojarvi JI, Rattya J, Myllyla VV, Knip M, Koivunen R, et al. (1998) Valproate, lamotrigine, and insulin-mediated risks in women with epilepsy. Ann Neurol 43:446-451.
- Verrotti A, Basciani F, Morresi S, de Martino M, Morgese G, et al. (1999) Serum leptin changes in epileptic patients who gain weight after therapy with valproic acid. Neurology 53:230-232.
- Demir E, Aysun S (2000) Weight gain associated with valproate in childhood. Pediatr Neurol 22:361-364.
- Rauchenzauner M, Haberlandt E, Scholl-Burgi S, Karall D, Schoenherr E, et al. (2008) Effect of valproic acid treatment on body composition, leptin and the soluble leptin receptor in epileptic children. Epilepsy Research 80:142-149.
- Wildman RP, Wang D, Fernandez I, Mancuso P, Santoro N, et al. (2013) Associations of testosterone and sex hormone binding globulin with adipose tissue hormones in midlife women. Obesity (Silver Spring) 21:629-636.
- Yasui T, Tomita J, Miyatani Y, Yamada M, Uemura H, et al. (2007) Associations of adiponectin with sex hormone-binding globulin levels in aging male and female populations. Clinica Chimica Acta 386:69-75.





