Clinical Evaluation of Deferasirox for Removal of Cr+6 Ions in Rats
Iranmanesh M1, Fatemi SJ2
1* Department of Chemistry, Islamic Azad University, Kerman Branch, Kerman, Iran.
2 Department of Chemistry, Shahid Bahonar University of Kerman, Kerman, Iran.
*Corresponding Author
Marzieh Iranmanesh,
Department of Chemistry,
Islamic Azad University,
Kerman Branch, Kerman, Iran.
E-mail: mzh_iranmanesh@yahoo.com
Article Type: Research Article
Received: September 20, 2013; Accepted: October 5, 2013; Published: October 7, 2013
Citation: Iranmanesh M, Fatemi SJ (2013) Clinical Evaluation of Deferasirox For Removal of Cr+6 Ions In Rats. Int J Clin Pharmacol Toxicol.2(7), 97-101. doi: dx.doi.org/10.19070/2167-910X-1300018
Copyright: Iranmanesh M© 2013. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The present research aimed to characterize the potential efficiency of deferasirox in removing chromium after its administration for 60 days following two doses of 15 and 30 mg/kg Cr+6 to the body weight of the male Wistar rats every day. After chromium administration some abnormal clinical signs such as red staining around the eyes, greenish mottling on the liver, weakness and loss of hair and weight, were observed in rats. Deferasirox was given orally to different groups of rats for a period of one week immediately after chromium administration. After chelation therapy, animals were anesthetized with ether vapors and then chromium and iron concentrations in various tissues were determined by graphite furnace and flame atomic absorption spectrometry methods, respectively. The chelation therapy results showed that deferasirox was able to remove chromium ions from the body and at the same, iron levels in tissues and clinical symptoms were also reduced.
2.Introduction
3.Experimental Section
3.1.Apparatus
3.2.Maintenance of the animals
3.3.Materials
3.4.Methods
4.Results
5.Discussion
6.References
Keywords
Deferasirox; Chromium toxicity; Chelation therapy; Rats; Iron.
Introduction
Chromium is an important metal, which is used in a variety of industrial applications e.g. textile dying, tanneries, metallurgy, metal electroplating, wood preserving and preparation of chromate compounds. It hence, large quantities of chromium have been discharged into the environment due to accidental releases or inadequate precautionary measures (Kimbrough et al., 1999). The chemical and toxicological behaviors of chromium depend on its oxidation state.
The most important concern from the human health point of view is chromium(VI) for both acute and chronic exposures (ATSDR, 1998). Chromium(VI) is known to enter cells readily via non-specific anion channels and it is thereafter reduced by intracellular reductants to the more stable Cr(III) with the concomitant formation of reactive intermediate species of Cr, Cr(V) and (IV), and reactive oxygen species(ROS) (Codd et al., 2001). These reactive species can cause DNA damage and lipid peroxidation (Bagchi et al., 2002; O’Brien et al., 2003). The ROS generated by these reactions are superoxide(O- 2), hydrogen peroxide (H2O2) and hydroxyl radical(OH.). It has been found that Cr(V) is a pulmonary sensitizer that causes bronchoplasm and anphylactoid reactions in sensitized workers (Moller et al., 1986). The acute ingestion of large amounts of Cr(V) results in acute tubular necrosis, marked interstitial changes and renal failure (Ellis et al., 1982). Genotoxicty studies have shown that Cr(V) compounds are the most potent genotoxins (Cohen et al., 1993). Based on sufficient evidence of carcinogenicity of Cr(V) compounds in human and animals, the International Agency for Research on Cancer (IARC) and the Department of Health and Human Services have treated Cr(V) compounds as carcinogenic compounds. Thus, removal of chromium, and especially of chromium(VI), is an essential pollution abatement process that should be applied to all industrial effluents that contain this contaminant. One of the most effective ways to remove toxic elements such as chromium from the biological system is chelation therapy. It involves the use of ligating drugs that binds metal for the treatment of potentially fatal conditions. These ligands promote the excretion and subsequent depletion of this transition metal in biological systems. Deferasirox (4-[3,5-bis(2-hydroxyphenyl)-1,2,4-triazol-1-yl]-benzoic acid, or ICL670, (Figure 1) that was first reported in 1999 is a new drug to remove toxic metal ions from biological systems (Heinz et al., 1999). It is a tridentate chelator with high selectivity for Fe+3(Steinhauser et al., 2004). In vivo, this selectivity is demonstrated by conserved plasma Zn and Cu levels in patients taking Deferasirox, and while its efficacy is rather low for inducing negative iron balance, it is effective and welltolerated (Nisbet-Brown et al., 2003). In 2005, Deferasirox became the first FDA approved oral alternative for treatment of iron overload and was subsequently approved in the EU in 2006 (Yang et al., 2007). Its relatively long half-life before excretion allows oncedaily dosage and good overall patient compliance, as well as cost-effectiveness. Deferasirox is considered to be superior to desferrioxamine (DFO). Iron chelation therapy (ICT) with (DFO), the current standard for the treatment of iron overload in patients with transfusion dependent disorders such as β-thalassemia, requires regular subcutaneous or intravenous infusions. This can lead to reduced quality of life and poor adherence, resulting in increased morbidity and mortality in iron overloaded patients with β-thalassemia (Scott and Orvig 2009). The aim of the present study was to investigate the chelation potency of Deferasirox given to animals after chromium loading. Testing was performed using an acute experimental model on rats with the chelator given shortly after chromium administration. This study indicates that this procedure might be useful for preliminary testing of the efficiency of the chelating agent to ascertain whether this chelator can mobilize and promote the removal of chromium from rat organs.
Experimental Section
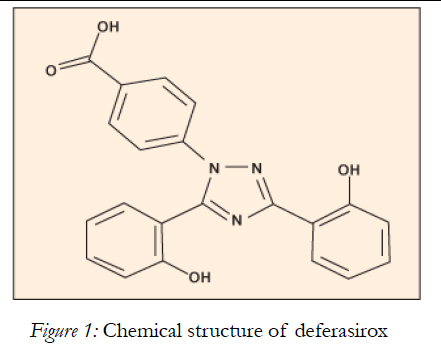
Figure 1: Chemical structure of deferasirox.
A Varian atomic absorption spectrometer (GFAAS, FAAS) was used for measurement of chromium and iron concentrations in various organs, respectively. Also a Mettler analytical balance Model AE 160 was used in this study.
Male Wistar rats were obtained from Razi Institute(Karaj, Iran). They bred in animal house at Kerman Neuroscience Research Center, Iran. The rats were maintained under a controlled light:dark (12:12 h) schedule at 23 ± 1˚C and humidity of 55%. The animals were assigned to control and treated groups and were kept in well cleaned sterilized cages. The rat food was purchased from Razi Institute. This study was approved by the ethics committee of Shahid Bahonar University of Kerman, Iran and Kerman Neuroscience Research Center, Iran.
K2Cr2O7 and other materials were purchased from Merck Chemicals Co. and deferasirox was purchased from Novartis Co.(Basel, Switzerland).
In our model, we used two different doses of chromium followed by an early administration of chelating agent. Experiments were performed on 7-week-old Wistar male rats. There were slight differences between the groups in the initial body weight of the rats (mean 200 g), but at the end of chromium administration experiment, those given chromium in their diet had significant weight loss (Table 1). Comparison of the weights in this experiment shows dietary treatment affected the food intake, whereby animals given normal diet consumed more food than those given chromium. Also because of the slight (but significant) differences in body weight of rats at the start of the study, the results can be influenced by the initial classification and assignment of rats to treated groups. Therefore, the day 1 groups’ body weights are notable and they must be considered. Consequently after acclimatization of animals, we assigned them randomly to control and treated groups. The first group(control group) was given normal food and water to drink. The treated groups were given water containing chromium to the extent of 15 mg Cr+6/kg body weight known as (low dose drinking of chromium) and 30 mg Cr+6/kg body weight known as (high dose drinking of chromium). Chelation therapy was carried out after chromium application. In this part of the research, treated groups were divided into three groups, before chelation therapy, without chelation therapy and chelation therapy with deferasirox(Table 2). Deferasirox was given orally at dose of 140 mg/kg body weight after chromium application during 1 week. Chromium toxicity symptoms observed in rats have been removed in short term (7 days) after drug administration. After chelation therapy, these rats were anesthetized with ether vapors and immobilized by cervical dislocation and their liver, kidneys, intestine, spleen and testicles samples were collected, weighed and dried for determination of their chromium contents. The samples were placed in an oven at 60˚C for 3 days. They were then digested by 1.5 mL of HNO3 per 1 g of dry weight tissues. After digestion, the solutions were evaporated with the addition of 1.0 mL of H2O2 under the hood. Then, the residue was diluted with water to 10 mL volume.
aMean of five determination standard deviation.
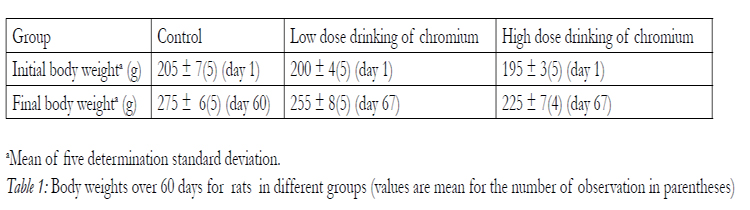

Table 1: Body weights over 60 days for rats in different groups (values are mean for the number of observation in parentheses).
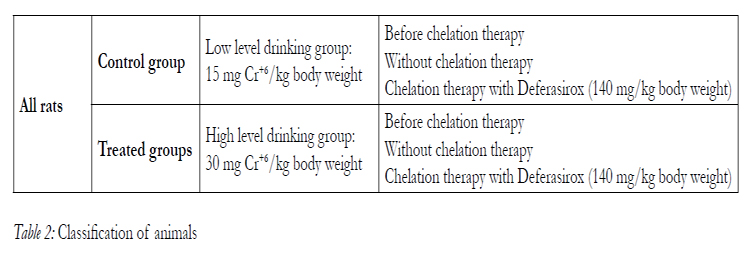
Table 2: Classification of animals.
Results
Results of chromium raising and iron reduction in organs of two chromium doses groups were statistically different. The chromium accumulation in tissues at high level drinking group was more than low level drinking group. A significant difference between control and treated groups was observed. The general symptom of toxicity appeared after 60 days of chromium administration. Abnormal clinical signs in animals were appeared as follows: darkening of the eyes, yellowish discoloration of hair, flaccid and hypotonic muscles, irritability, weakness and loss of hair. Also the body weights of all animals in treated groups were significantly decreased. The highest amount of chromium was found in intestine followed by kidneys. After the chelation therapy, the obtained results showed that chromium levels present in all tissues were significantly reduced whereas, iron concentration returned to the normal level and the symptoms also reduced. Iron level is lowest in the group having the highest chromium concentration, which is probably because of a significant interference that could take place by chromium through iron uptake mechanism. The t-test was applied to the results assuming the certified values are the true values. Deferasirox was more efficient in decreasing chromium concentration from intestine. The results of organ distribution of chromium before and after chelation therapies are shown in (Table 3). Furthermore, iron concentration after chromium administration was significantly decreased. The difference between iron values before and after chelation therapy is notable. These results are summarized in (Table 4). In order to investigate the spontaneous effect of chromium removal from the body in the course of time, one group was treated as without chelation therapy.
Comparison of the results obtained from both (before and without chelation therapy) groups are showing that the passage of time had no significant effect on removal of chromium.
This indicating, Deferasirox is efficient in returning iron concentration to its nearly normal level.
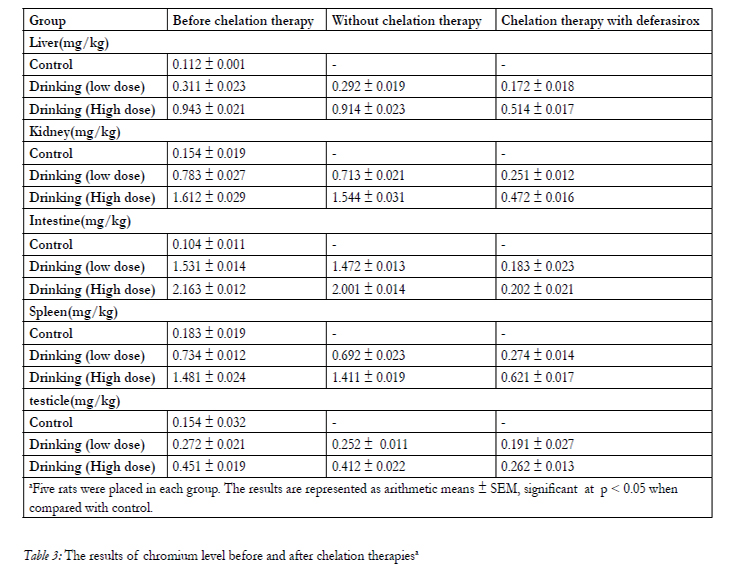
Table 3: The results of chromium level before and after chelation therapiesa
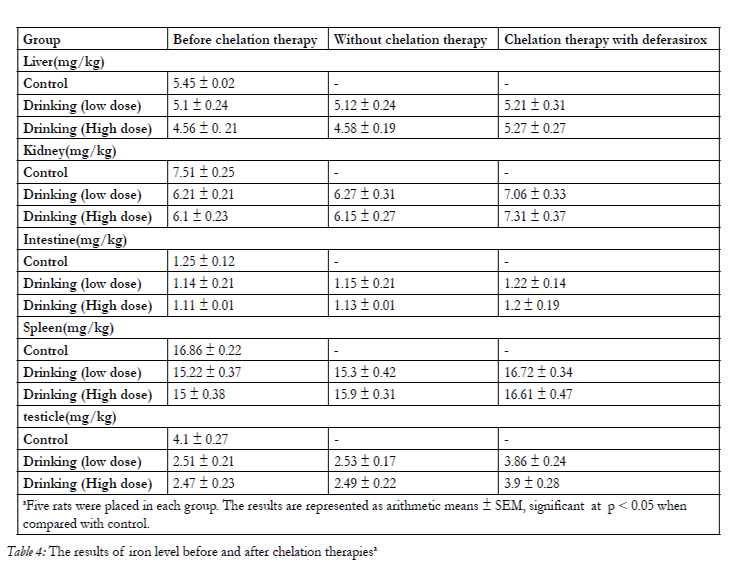
Table 4: The results of iron level before and after chelation therapiesa
Discussion
The aim of the present work was to evaluate the ability of deferasirox in removing chromium from the body. Many studies have now reported, the high absorption, distribution, long-term efficacy and safety of deferasirox in removing some toxic metal ions and treating iron overload in patients with β-thalassaemia major (Cappellini, 2008; Neufeld, 2006; Wood et al., 2006). In this investigation, a short-term experimental model was used in order to speed up the preliminary testing procedure. The effects of chelator on chromium and iron levels were remarkable. It has been reported that the chelating agents having higher stability constants with a metal in aqueous solution may also prove successful in reducing the body burden of the metal (Kaur et al., 1984). Gastrointestinal absorption and uptake of chromium after oral exposure shows the accumulation of chromium in different organs as well as decrease of iron concentration in different tissues. After administration of chelating agents, the chromium content returned to nearly normal level of control group, which indicates that deferasirox effectively increases the elimination of chromium in rat organs. The symptoms were also disappeared. A comparison of the results obtained from before and without chelation therapies indicate that removal of chromium is not time dependent at all. Toxicity and side effects of deferasirox are reported to be very low (Cappellini, 2008), therefore after basic preclinical research, they could be recommended for human administration. With considering, our obtained results and previous researchers (Fatemi et al., 2007; Amiri et al., 2007; Tubafard and Fatemi, 2008; Fatemi et al., 2009) it can be also concluded that deferasirox is efficient enough to remove chromium from all tissues and treat its side effects and general symptoms of toxicity. Thus deferasirox represent a promising drug of Cr-mobilizing agent. Our results showed that this procedure might be useful for preliminary testing of the efficiency of chelating agent in removing of chromium.
References
- Agency for Toxic Substances and Diseases Registry (ATSDR), (1998) Toxicological Profile for Chromium. Public Health Service. US Department of Health and Human Services, Atlanta, GA.
- Amiri A, Fatemi SJ and Fatemi SN (2007) Removal of Thallium by combining desferrioxamine and deferiprone chelators in rats. Biometals 20: 159–163.
- Bagchi D, Stohs SJ, Downs BW, Bagchi M, Preuss HG (2002) Cytotoxicity and oxidative mechanisms of different forms of chromium. Toxicology 180: 5–22.
- Cappellini MD (2008) Long-term efficacy and safety of deferasirox. Blood Review 2: 35–41.
- Codd R, Dillon CT, Levina A, Lay PA (2001) Studies on the genotoxicity of chromium: from the test tube to the cell. Coordination Chemistry Reviews 216–217: 537–582.
- Cohen, MD, Kargacin B, Klein CB, Costa M (1993) Mechanisms of chromium carcinogenicity and toxicity. Critical Reviews in Toxicology 23: 255–281.
- Ellis EN, Brouhard BH, Lynch RE, Dawson EB, Tisdell R, Nichols MM, Ramirez F (1982) Effects of hemodialysis and dimercaprol in acute dichromate poisoning. Journal of Toxicology-Clinical Toxicology 19: 249–258.
- Fatemi SJ, Amiri A, Bazargan MH, Tubafard S and Fatemi SN (2007)Clinical evaluation of desferrioxamine (DFO) for removal of thallium ions in rat. International Journal of Artificial Organs 30: 902–905.
- Fatemi SJ, Tubafard S, and Nadi B (2009) Evaluation of the effect of cadmium on rat organs and investigation of diethyl carbamate as an oral drug in treatment of cadmium toxicity. Medicinal Chemistry Research 18:179–186.
- Heinz U, Hegetschweiler K, Acklin P, Faller B, Lattmann R and Schnebli HP (1999) 4-[3,5-Bis (2-hydroxyphenyl)-1,2,4-triazol-1-yl]- benzoic acid: a novel, efficient and selective iron (iii) complexing agent. Angewandte Chemie International Edition 38: 2568–2571.
- Kaur G, Srivastava UC, Dwivedi RS and Srivastava RC (1984) Influence of polyaminocarboxylic acids on the removal of manganese- 54 from the body organs of sham-operated and partially hepatectomized rats. Toxicology Letters 22: 1–6.
- Kimbrough DE, Cohen Y, Winer AM (1999) A critical assessment of chromium in the environment. Critical Reviews in Environmental Science and Technology 29: 1–46.
- Moller DR, Brooks SM, Bernstein DI, Cassedy K, Enrione M, Bernstein IL (1986) Delayed anaphylactoid reaction in worker exposed to chromium. Journal of Allergy and Clinical Immunology 77: 451–456.
- Neufeld EJ (2006) Oral chelators deferasirox and deferiprone for transfusional iron overload in thalassemia major: new data, new questions. Blood 107(9): 3436–3441.
- Nisbet-Brown E, Olivieri NF, Giardina PJ, Grady RW, Neufeld EJ, Sechaud R (2003) Effectiveness and safety of ICL670 in iron-loaded patients with thalassaemia: a placebo-controlled, dose-escalation trial. Lancet 361: 1597–1602.
- O’Brien TJ, Ceryak S, Patierno SR (2003) Complexities of chromium carcinogenesis: role of cellular response, repair and recovery mechanisms. Mutation Research 533: 3–36.
- Scott LE, Orvig C (2009) Medicinal inorganic chemistry approaches to passivation and removal of aberrant metal ions in disease. Chemical Reviews 109:4885–4910.
- Steinhauser S, Heinz U, Bartholoma¨M, Weyhermu¨ller T, Nick H and Hegetschweiler K (2004) Complex formation of ICL670 and related ligands with Fe(III) and Fe(II). Europian Journal of Inorgorganic Chemistry 21: 4177–4192.
- Tubafard S and Fatemi SJ (2008) Chelation of bismuth by combining desferrioxamine and deferiprone in rats. Toxicology and Industrial Health 24: 235–240.
- Wood JC, Otto-Duessel M, Gonzalez I, Aguilar MI, Shimada H, Nick H (2006) Deferasirox and deferiprone remove cardiac iron in the iron-overloaded gerbil. Translational Research 148(5):272–280.
- Yang LPH, Keam SJ, and Keating GM (2007) Deferasirox: a review of its use in the management of transfusional chronic iron overload. Drugs 67: 2211–2230.





