Oxidative Stress in Paediatric Patients With Diabe-tes Mellitus Type 1 and Relationship With Glucemic Levels
Dalyla Alonso Rodríguez1*,Ela Moreno Tellez2,Yanet Alarcon Martinez3, Frank Medina Ali4.
1*Specialist in pharmaceutical sciences, Pediatric Provincial Hospital Dr. Euardo Agramonte Pina.
Camagüey - Poly-Clinician of Pediatric Specialties. Camagüey, Cuba.
2 Specialist of second degree in clinical laboratory.
3 First-degree specialist in clinical laboratory.
4 Specialist of second degree in endocrinology.
*Corresponding Author
Dalyla Alonso Rodriguez,
Specialist in pharmaceutical sciences,
Pediatric Provincial Hospital Dr. Euardo Agramonte Pina,
Camagey - Poly-Clinician of Pediatric Specialties,
Camaguey, Cuba.
E-mail: dalyla@finlay.cmw.sld.cu
Article Type: Review Article
Received: January 12, 2013; Accepted: January 27, 2013; Published: January 31, 2013
Citation: Dalyla Alonso Rodríguez, Dr Ela Moreno Téllez , Dr Yanet Alarcón Martínez, Dr Frank Medina Alí (2013) Oxidative Stress in Paediatric Patients With Diabetes Mellitus Type 1 and Relationship With Glucemic Levels. Int J Clin Pharmacol Toxicol. 2(1), 45-46. doi: dx.doi.org/10.19070/2167-910X-130009
Copyright: Dalyla Alonso Rodríguez© 2012. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
This study was made in paediatric patients affected by diabetes mellitus type 1. Fasting blood samples were obtained to determine glucose, bilirrubin, uric acid, ascorbic acid, ceruloplasmin , albúmin and LDLox lev-els. We found high levels of LDL ox and glycemia, and low levels of the rest of the antioxidants. We conclude that oxidative stress was present in these patients
2.Introduction
3.Case Description
4.Method
4.1 Criteria of inclusion
4.2 Criteria of exclusion
5.Results
6.Discussion
7.Conclusions
8.Recommendations
9.References
Keywords
Oxidative Stress; Antioxidants; Diabetes Mellitus Type 1; Glycemia; Paediatric.
Introduction
The oxidative stress has total success in a rut through the measurement of the damages caused on important macromolecules at our or-ganism of the stress, and no for these free radi -cals’ direct measurement than for your fleeting nature they are approximately imposible [1].
The measurement of the damage to lipids would be able to evaluate her by means of the calculation of the damage to lipoproteínas for the increment of the sensibility of the LDL to oxidation. This LDLox has a potential aterogénic height and contributes to of direct mode the endothelial damage and formation of ateroma’s plate. The LDL’s glicosilation can be one of the factors that contribute to the increase of this sensibility like may happen in diabetes mellitus [2].
You can try on the damage to proteins determining seric concentrations our organism’s of important proteins and that definitively provide us information about the system of antioxidant defense like they are: Albumin, ceruloplasmin and total bilirrubin.
The consideration of the levels of seric uric acid ( Au ) like measure of the antioxidant activity of the human serves to be a part of an innovative instruc -tion about the antioxidant power of this substance considered until very recently of reject, his capabil -ity to receive free present radicals’ electrons in the cell like hidroxil ( HO.), Lipoperoxil (LOO.) And hy-pochlorite ( ClO.), You give him the possibility of de -fending us of the whole damage that they involve. The vitamin C, for your part, not only has important antioxidant shows at our organism’s watery zone, but also tocoferil is able to regenerate the radicle and the Au, forming radial ascorbilo that is totally innocuous. The possibility of guaranteeing seric levels made suitable through the diet you make her form priority part in the antioxidant humans.
In diabetic patients, the oxidative stress can result from an excessive production of reactive species of oxygen (ROS), especially the super-oxide anion; Or for decrease of the antioxidant stock, fundalmental albumin, ceruloplasmin and uric acid [1,2]. For it before exposed we intended to diagnose the oxida -tive stress in diabetic children type 1 at our clinical laboratory.
Case Description
An 18 year old Caucasian female presented to the emergency room (ER) during the morning with a one day history of nau-sea, vomiting, chills, and vague abdominal pain. She reported her vomit as greenish in color and non-bloody. There was no evidence of fever, recent travel, contact with sick persons, or diet changes. She had been hospitalized approximately six weeks pror for acute gastroenteritis but was otherwise healthy. The only medication she took as an outpatient was minocycline of acne. The patient denied using illicit drugs, but admitted alcohol in-take as recently as two nights prior to admission.
The patient’s physical exam in the ER was normal except for some abdominal tenderness and right sided guarding. A com-plete metabolic panel (CMP) and complete blood count (CBC) were ordered on admission to the ER. The laboratory values were within normal limits with the exception of hypokalemia (3.1 mEq/L), hyperglycemia (164 mg/dL) and an elevated white blood cell (WBC) count (12,400 cells/mL). Both the pregnancy test and urine drug screen conducted were negative. A urinalysis was also performed and did not indicate any abnormalities or infection. While in the ER, she received an injection of prometh-azine 25 mg. Approximately one hour after the promethazine ad-ministration she was noted to be thrashing and moving around in her bed. The movements subsided and on the next assessment two hours later, the patient was observed to be resting quietly.
The patient was admitted to the hospital that evening for further evaluation and orders for intravenous fluid replacement (Dex-trose 5% and normal saline with 20 mEq potassium chloride) and promethazine 25 mg intravenously as needed for nausea and vomiting were written. Through the course of the first night, the patient continued experiencing emesis despite two additional promethazine 25 mg injections. She was noted to be consider-ably anxious and periodically would thrash around erratically in the bed. The patient was given a one-time intravenous dose of lorazepam 1mg which was successful in sedating the patient who rested comfortably for the remainder of the night.
After awakening the following morning, the patient once again experienced continuous vomiting. She was given ondansetron which appeared to elevate her symptoms. The patient continued to complain of abdominal pain and display left sided guard-ing. Though not febrile at admission, a temperature of 100.8º F (38.2°C) prompted a urinalysis, blood and urine cultures, and a computerized topography (CT) of the abdomen, none of which indicated infection or other abnormalities. A CMP was also con-ducted that morning and all laboratory values were normal with the exception of resolving hypokalemia (3.3 mEq/mL) for which she received potassium chloride 40 mEq by mouth.
The patient received two additional doses of promethazine for her continued nausea and vomiting. Her anxious and erratic be-havior and abdominal pain also continued throughout the day. Her nausea and vomiting was eventually controlled with the ad-dition of scheduled intravenous ondansetron 4 mg. Due to ongo-ing abdominal pain and nausea the evening of the second night of her hospital stay, the patient received an intravenous dose of ketorolac 60 mg with her promethazine 25 mg injection. After the administration of both agents, the patient’s behavior became even more increasingly erratic. She began thrashing around in her bed with more force than previously seen and attempted to disrobe and expose herself to the nursing and medical staff pre-sent. The patient did not respond to nor elicit any verbal com-munication. This behavior continued until the early morning when the patient eventually fell asleep. The following morning, the patient stated that she had no recol-lection of this behaviour and appeared calm. The order for as need promethazine was discontinued, but the patient continued to receive the ondansetron which was successful in controlling her nausea and vomiting. After consultations from surgery and gastroenterology, the patient was diagnosed with mild gastritis and duodenitis.Because the patient did not have any known psychiatric history, her behaviour was suspected to be a result of promethazine, ke-torolac, or a combination of both medications. We did not sus-pect ondansetron or any drug-interaction involving ondansetron because the erratic behavior appeared before the administration of ondansetron, did not increase when ondansetron alone was added to promethazine, but did increase markedly when ketorol-ac was added to the promethazine regimen. Both promethazine and ketorolac were discontinued and no additional doses were administered. The patient did continue to receive the scheduled ondansetron which alleviated her symptoms. She did not exhibit any additional abnormal behavior throughout the remainder of her hospitalization and was discharged on day four of her hospital stay.
Methods
Type accomplished a study in 30 diabetic patients itself 1 taken in Endocrinology’s consultation of Especialidades’s Poly-Clinician Pediatric. Camaguey in the period once February 2012 was understood between October 2011.
Diabetic children type 1, ambulatory, with over 5 elderly years and with a minimum of 3 years of evolu -tion of the disease.
• Children that take treatment with vitaminic supplements or another drug that you interfere in any one of the complementary to accomplish.
• Patients hospitalized by decompensation of the disease.
• Patients with associated to diseases the Dia -betes Mellitus type 1.
• One considered like children with bad meta -bolic control ( MCM ) all those that they not do their job with the following criteria proposed by Diabetes’s Latin American Association ( ALAD ): [3]
• Average of glucemias inside the following límit- under 5 elderly years: 5.5-11 mmol L and older of 5 elderly years: 4.4-10 mmol /L
Total seric bilirrubin took signs of blood without eat-ing to determine levels ( Gendrasik Grof ) ( CN: Less de17 μmol/L ), albumin (colorimetric method with verde bromocresol, CN: : ≥ 33 g/L), ceruloplasmin ( modified Ravin, CN:22-42 mg % ), uric acid ( Henrry Sabel Kin, CN: 143-339 μmol/L), ascorbic acid ( meth -od of analysis with 2,4 dinitrofenilhidrazina, CN:11.6-113.6 μmol/L) and LDLox ( enzymatic method with suddenness with PEG 6000 ) CN; 5-15 μg/ml Excell accomplished the statistical analysis of the data himself by means of the program.
Results
You observe the incidence of decreased levels in the board of antioxidant such as: Albumin, uric acid and vitamin C and increased levels of LDLox which evidences oxidative stress for unbalance. The elevated levels of gluycemia evidence the bad metabolic control of the disease.
As it is appreciated, the system of antirust defense was decreased (low moral values of albumin in 43 % of patients, of uric acid in a 27 % and of vitamin C in a 50 %), for your part the LDLox showed up incre -mented in 76.6 % of the patients, being this one defi -nite marker for the diagnosis of oxidative stress, in 7 patients the LDLox showed up with numbers within the doubtful range ( 15-40 µg/mL).
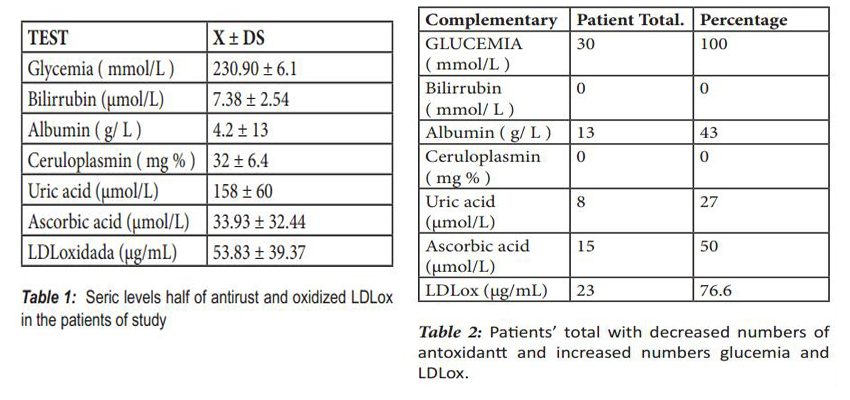

Tables:
Discussion
I raise objections of study in all the children demonstrated him a bad metabolic control of diabe -tes mellitus type 1 according to criteria of Diabetes’s Latin American Association (ALAD).[3].
You are demonstrated the hyperglycemia produces glicosilation not enzymatic of proteins, which causes endothelial damage and this in turn induces free radicals’ production. The decrease of the antioxidant stock, such I eat: Uric acid, ascorbic acid and albumin triggers also free radicals’ accumulation, especially super-oxide anion.( 1.2 ).
You perform on theuric acid like antirust together with the vitamin C, the first one possesses a couple of electrons shared in that you perceive the reactive sorts of oxygen and it gives them up to the second one, creating for oneself an innocuous complex that is debugged easily at the organism; The unbalance becomes established when you find any of them decreasedly [4]
Conclusion
• Exists a stress oxidativo in over 50 % of the infantile studied population.Type demonstrated the bad metabolic control in dia -betic children itself 1.
• LDLox’s levels found lifted I raise objections of study in 76,6 % of the children.
Recommendation
• Having an effect on the Diabetes Mellitus’s metabolic control type 1
References
- Medaoui AE., Champlain J. : Prevención de la hiperten-sion, resistensia a la insulina, y estres oxidativo por el acido lipoico. Hipertensión 2002; 39: 303-07
- Asayama K., Uchida N., Nakane T., Hayashibe H., Doboshi K., Amemiya S., et al. : Antioxidantsin the serum af chil-dren whith insulindependent diabetes mellitus. Free Radic. Biol. Med. 1993; 15(6) : 597-602.
- Ramos V., Güell R., Vera M., Dávalos A., Ferraro M., et al. Consenso latinoamericano sobre diabetes en el nino y el adolescente. Cartagena de Indias. Colombia: Novo care., 1998:p. 7-21.
- Andrieva-Gateva P.: Insulin resistance and oxidative stress. Vutr Boles 1999; 31(4):9-19.
- Williams D., Dorchy H., Dufrasne D.: Serum antioxidant status and oxidized LDL in well-controlled young type 1 diabetic patients with and without subclinical complications. Athero-sclerosis 1998; 137suppl: S61-4.
- Delmas-Bauvieux MC., Peuchant E., Thomas MJ., Du -bourg L., Pinto AP et al.: The place of electron spin resonancemethods in the detection of oxidative stress in type 2 diabetes with poor glicemic control. Clin. Biochem. 1998.; 31(4):221-8.





