Vocal Cord Palsy an Induced Complication of Carboplatin and Paclitaxel: A Case Report
Rawish K1*, Munjal SK2, Sharma P3, Panda NK4
1 Junior Speech Therapist, Department of Otolaryngology, PGIMER, Chandigarh, India.
2 Associate Professor, Speech & Hearing Unit, Department of Otolaryngology, PGIMER, Chandigarh, India.
3 BASLP Intern, Speech & Hearing Unit, Department of Otolaryngology, PGIMER, Chandigarh, India.
4 Professor & Head, Department of Otolaryngology, PGIMER, Chandigarh, India.
*Corresponding Author
Rawish Kumar,
Junior Speech Therapist, Department of Otolaryngology, PGIMER, Chandigarh, PIN: 160012, India.
Tel: +91-9780831511
E-mail: rawishkumar@gmail.com
Received: October 24, 2016; Accepted: February 06, 2020; Published: February 07, 2020
Citation: Rawish K, Munjal SK, Sharma P, Panda NK. Vocal Cord Palsy an Induced Complication of Carboplatin and Paclitaxel: A Case Report. Int J Clin Exp Otolaryngol. 2020;6(1):106-107. doi: dx.doi.org/10.19070/2572-732X-2000019
Copyright: Rawish K©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Unilateral vocal cord paralysis is common. Most of time unilateral vocal cord palsy is idiopathic. Other causes include malignancy, secondary to neck or recurrent laryngeal nerve trauma, intubation or secondary to surgery however, taxens induces causes paresis may include larynx.
Case Report: We report a patient who had cancer of cervix (Endometrium) and developed vocal cord paralysis after completion of five cycles of treatment with injections paclitaxel 250mg and carboplatin 450mg. Patient’s stroboscopic examination and voice analysis confirmed vocal cord paralysis with cord lateralized in paramedian position and with breathy quality of voice. The vocal cord paralysis was believed to have occurred due to neurotoxic effect of carboplatin and paclitaxel, as an added complication of these drugs.
Conclusion: Carboplatin and paclitaxel can induce bilateral or unilateral vocal cord paralysis. The concurrent amount of dose used of carboplatin and paclitaxel might have contributed to this illness in patient.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.References
Keywords
Carboplatin; Paclitaxel; Voice Analysis; Breathy Voice.
Introduction
Unilateral vocal cord paralysis is most common than bilateral vocal cord paralysis. In 30~50% of the subjects the unilateral vocal cord paralysis is idiopathic and asymptomatic [1]. Other causes of unilateral vocal cord paralysis may include certain neurologic illness [2], trauma, thyroidectomy [3], and intubation during surgery, malignancy [4]. Sometimes it is the only sign of an otherwise asymptomatic malignancy of larynx [5]. It is believed that the paresis or paralysis may be caused due to the neurotoxic effect of carboplatin and paclitaxel or such neurotoxic drugs.
Case Reportn
A 54 years old female patient reported with complaints of weak and low voice and change in pitch. Patient was receiving platinumbased chemotherapy for adenocarcinoma papillary serous of cervix cancer, stage IIIb without metastases which confined to the uterus only. The patient underwent chemotherapy containing Carboplatin 450mg and Paclitaxel 250mg. Patient reported change of voice prior to completion of 5th cycle of chemotherapy. After 5th cycle of the chemotherapy patient was referred to otolaryngologist for evaluation. In stroboscopic examination one cord was visualized in the paramedian position and other cord was partially approximating the paralyzed one. The perceptual voice analysis on GRBAS scale revealed breathy voice with alteration in pitch as well as loudness in objective assessment on Dr Speech software during sustain phonation of vowel/ae/(as shown in table). Objective voice assessment revealed more jitter (>1%), shimmer (>3%) and F0 tremor. The mean F0 was low and varying from habitual F0 with high variation of Min F0 and Max F0 with high normalized noise energy (NNE). The signal to noise ratio (SNR) and harmonic noise ratio were less. The intensity was also varying during sustain phonation. For management, patient was worked up on the vocal cord approximation techniques to rehabilitate the voice and made the communication better.
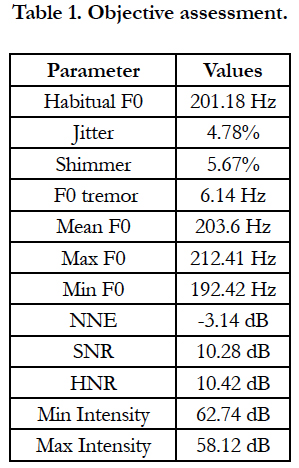

Table 1. Objective assessment.
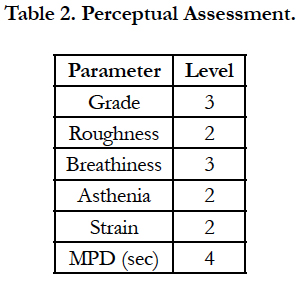
Table 2. Perceptual Assessment.
Discussion
Most common etiologies of vocal cord paralysis have been found to be idiopathic and others etiologies are due to malignancy or carcinoma, iatrogenic, and neck trauma of vocal cord paralysis usually seen with symptoms such as hoarseness, dysphonia, and sometimes aspiration too [6]. Carboplatin and paclitaxel (taxane) are neurotoxic drugs which cause peripheral neuropathy neurological disorder. However, the carboplatin and paclitaxel is less neurotoxic than other like vinka alkaloids. Treatment with carboplatin-taxane regimens exhibit ongoing symptoms such as feeling sick, hair loss, numbness or tingling hands or feet, diarhhoea etc following the completion of treatment in the 25% of the patients [7]. Jeffrey Hsu and Melin Tan-Geller found that paclitaxel induces reversible bilateral vocal cord paralysis [8]. On comparisons with the previously cited case studies, it appears that, this could state indirectly that like other neurotoxic drugs, many other patients might have undiagnosed carboplatin and paclitaxel brought vocal fold paralysis and this complication during chemotherapy is less reported.
Conclusion
Apart from other causes of vocal cord paralysis, the history of use of the neurotoxic chemotherapeutic drugs also should be the part of evaluation. Prior to start chemotherapy usually in old age,patient should be explained that dysphonia, stridor or aspiration may be some additional side effects of these neurotoxic drugs which can be temporary or permanent.
References
- Myssiorek D. Recurrent laryngeal nerve paralysis: anatomy and etiology. Otolaryngol Clin North Am. 2004 Feb; 37(1): 25-44. PMID: 15062685.
- Fairley J, Hughes M. Acute stridor due to bilateral vocal fold paralysis as a presenting sign of myasthenia gravis. J Laryngol Otol. 1992; 106:737–738. PMID: 1402370.
- Holinger LD, Holinger PC, Holinger PH. Etiology of bilateral abductor vocal cord paralysis: a review of 389 cases. Ann Otol Rhinol Laryngol. 1976; 85:428-36. PMID: 949150.
- Takayama H, Sato H, Ota Z, Nishizaki K, Ogawa N. Bilateral vocal cord paralysis due to laryngeal carcinoma in Parkinson’s Disease. J Med. 1987; 18: 251–258. PMID: 3480935.
- Baumann M, Heffner J. Bilateral vocal cord paralysis with respiratory failure, a presenting manifestation of bronchogenic carcinoma. Arch Intern Med. 1989; 149: 1453–1454. PMID: 2730268.
- Benninger MS, Gillen JB, Altaian JS. Changing etiology of vocal fold immobility. The Laryngoscope. 1998 Sep; 108(9): 1346-50.
- Pignata S, De Placido S, Biamonte R, Scambia G, Di Vagno G, Colucci G, et al. Residual neurotoxicity in ovarian cancer patients in clinical remission after first-line chemotherapy with carboplatin and paclitaxel: the Multicenter Italian Trial in Ovarian cancer (MITO-4) retrospective study. BMC Cancer. 2006; 6: 5. PMID: 16398939.
- Hsu J, Tan-Geller M. Reversible Paclitaxel-Induced Bilateral Vocal Fold Paresis. International Journal of Otolaryngology and Head & Neck Surgery. 2015 Apr 17; 4(03): 254.





