Ecthyma Gangrenosum without Pseudomonas Bacteraemia in an Immunocompetent Healthy Adult
El-Sherif NA1, El-Mangush IM1, El-Dibany SA2*
1 Dermatology Department, Benghazi university, Gamhoria hospital, Benghazi, Libya.
2 Dermatology Department, Omar El-Mukhtar university, Al-Beida, Libya.
*Corresponding Author
Salwa A. El-Dibany,
Dermatology Department,
Omar El-Mukhtar university, Al-Beida, Libya.
Email: salwaeldibani@yahoo.com
Article Type: Case Study
Received: December 23, 2016; Accepted: February 01, 2017; Published: February 02, 2017
Citation: El-Sherif NA, El-Mangush IM, El-Dibany SA (2017) Ecthyma Gangrenosum without Pseudomonas Bacteraemia in an Immunocompetent Healthy Adult. Int J Clin Dermatol Res, S2:001, 1-3. doi: http://dx.doi.org/10.19070/2332-2977-SI02001
Copyright: El-Dibany SA© 2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
2.Introduction
3.Case Presentation
4.Discussion
5.Conclusion
7.References
Keywords
Ecthyma Gangrenosum; Pseudomonas Aeruginosa; Healthy Subjects.
Introduction
Pseudomonas aeruginosa may be presented with mild cutaneous infections in healthy persons like a toe web infections, hot tub folliculitis, however, in persons with lowered resistance, more severe infections such as malignant otitis externa and necrotizing fasciitis are observed [1]. Ecthyma gangrenosum (EG), the characteristic skin symptom of Pseudomonas septicemia, occurs in debilitated or in immunocompromised patients [2, 3]. There are isolated reports of its occurrence in normal healthy individuals with no evidence of bacteremia [4].
Case Presentation
A 62-year-old Libyan female patient was admitted to dermatology department at El-Jamhoria hospital in Benghazi, with a 1-month history of painful ulcer on the skin over her left breast. She was a febrile and in good condition. Local skin examination revealed a single necrotic ulcerated skin lesion covered with central black eschar was present over her left breast skin surrounded by an intense red areola. Two other smaller lesions with the same features were present (Figure 1). The laboratory findings revealed: peripheral WBC count 1600 mm3 of which 69% were neutrophils, 24.5% were lymphocytes, and 6.3% were monocytes; hemoglobin 11.4g/ dL and platelets 243 x 103/L . Test results for both syphilis and HIV were negative . Liver function tests, blood urea nitrogen and serum creatinine levels, and chest radiographs were normal. Pseudomonas aeruginosa was isolated from the necrotic ulcerated skin lesion. whereas the results of repeated blood cultures were negative.


Figure 1. A Necrotic Ulceration of the Breast Skin and Scattered Small Ulcerated Erythematous Papules.
Histopathological examination of skin biopsy from the ulcer showed a necrotic epidermis with dermal infiltrate of a moderate number of lymphocytes, and neutrophiles pronounced in the perivascular area (Figure 2, 3). The diagnosis of EG associated with Pseudomonas infection was made. The patient was treated with intravenous ceftriaxon 1 g IV every 12 hours and three days later gentamicin 100 mg IV every 8 hours has been added according to the result of culture sensitivity, this combination therapy was continues for six weeks. Local application of Silver sulfadiazine cream with surgical debridement were also instituted for better wound healing (Figure 4, 5). Two months later the skin lesion completely healed.
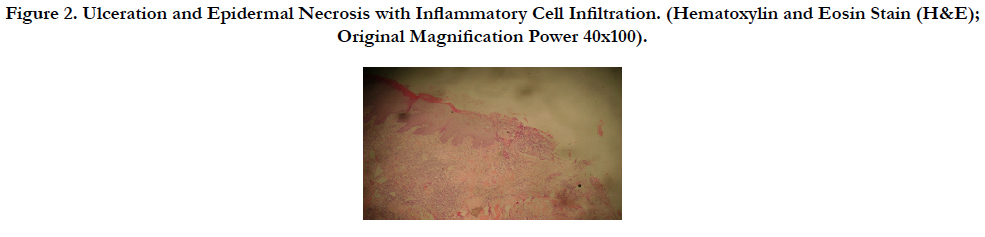
Figure 2. Ulceration and Epidermal Necrosis with Inflammatory Cell Infiltration. (Hematoxylin and Eosin Stain (H&E); Original Magnification Power 40x100).
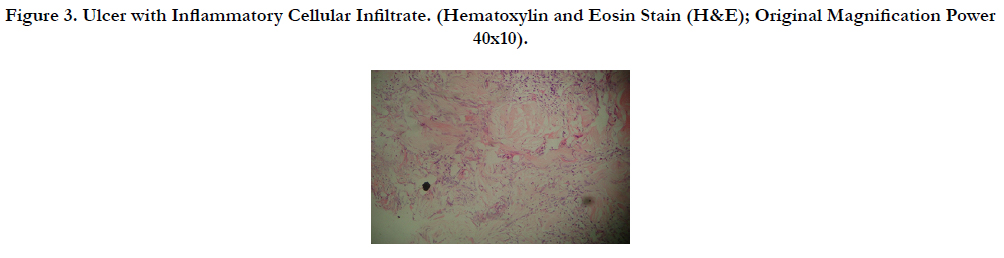
Figure 3. Ulcer with Inflammatory Cellular Infiltrate. (Hematoxylin and Eosin Stain (H&E); Original Magnification Power 40x10).


Figure 4. Ulcer After Surgical Debridement of the Necrotic Lesion and Initiation of Systemic Antibiotics.


Figure 5. Healing of the Ulcer after Complete Coarse of Antibiotic.
Discussion
EG was first described in 1897 as a cutaneous manifestation of Pseudomonas aeruginosa bacteremia [5]. This disease had been related to life-threatening septicaemic infections with high mortality [2]. It occurs mostly in immunocompromised patients with leukemia, lymphoma and other malignant diseases, especially in the presence of severe neutropenia, furthermore EG reported in severe burns or organ transplant, or in people receiving immunosuppressive therapy [2, 3, 6]. However, it has been reported also in patients without previously identified medical problems [3-5].
Although EG is now known to be caused by a variety of bacteria and fungi, it still considered to be pathognomonic for P. aeruginosa infection and it continues to be the most common cause [4, 7].
The lesion begins with a painless well-circumscribed edematous papule that subsequently, evolves to a hemorrhagic bulla that ruptures, forming a necrotic ulcer with a gray-black eschar surrounded by an erythematous halo. Certain localizations are particularly affected such as the perineum (57%), the extremities (30%) and trunk (6%), furthermore, fever is noticed in 96% of cases [4].
The pathogenic mechanism for the cutaneous lesion started with bacterial invasion of the arteries in the dermis and subcutaneous tissues occurs by hematogenous seeding in septicemic patients and by direct inoculation in non-bacteremic ones. Subsequently a necrotizing vasculitis caused by obstruction of the dermal vessels and dissolution of the elastic lamina of blood vessels by Pseudomonas elastase and exotoxin A were responsible for the direct tissue destruction and ulcerative lesions [8, 9].
Treatment should begin on the basis of clinical findings without waiting for laboratory confirmation. The recommended treatment is an antipseudomonal beta-lactam antibiotic combined with an aminoglycoside appropriate for both bacteremic and nonbacteremic EG [11]. Moreover, surgical debridement has been also recommend along with skin grafting when needed [2].
The synergistic effect with the combination of beta-lactams and aminoglycosides, with the risk of development of resistant strains with monotherapy have made the combination therapy a preferred mode, furthermore, the reduction of mortality rate among patients with invasive infections received combination therapy compared with monotherapy has been reported [11]. Our patient received combination therapy along with surgical debridement of the necrotic ulcer to promote its healing.
Mortality rates of patients with EG vary between 35% and 90% depending on the severity of the underlying sepsis [3], while in patients without documented bacteremia, mortality rates can be as low as 15% [12]. Furthermore, the mortality rate was 7.5 % in the group of patients with skin lesions considered to be primary and 20 % in the group of patients with skin lesions considered to be secondary to bacteremia [4].
Conclusion
Dermatologist must be aware of these conditions and consider EG as a likely diagnosis when facing a healthy adult with skin lesions such as those described above even with a negative blood cultures. In this situation, prompt debridement, and initiation of antibiotics with appropriate coverage against Pseudomonas species should be initiated.
References
- Agger WA, Mardan A (1995) Pseudomonas aeruginosa infections of intact skin. Clin Infect Dis. 20(2): 302-8.
- Singh N, Devi M, Devi S (2005) Ecthyma gangrenosum: a rare cutaneous manifestation caused by pseudomonas aeruginosa without bacteremia in a leukemic patient. Indian J Dermatol Venereol Leprol. 71(2): 128-129.
- Bodey GP, Jadeja L, Elting L (1985) pseudomonas bacteremia: retrospective analysis of 410 episodes. Arch Intern Med. 145(9): 1621-1629.
- Gençer S, Ozer S, EGe Gül A, Doğan M, Ak OP (2008) Ecthyma gangrenosum without bacteremia in a previously healthy man. Case report. J Med Case Rep. 2: 14.
- Colette CM, Scarfone RJ, Conway D (2000) Ecthyma gangrenosum as a manifestation of pseudomonas sepsis in a previously healthy child. Ann Emerg Med. 36(4): 383-387.
- Tornero C, Ricart C, Arnedo AL, Baeza R (1999) Non-bacteremic Ecthyma gangrenosum in a patient with human immunodeficiency virus infection. Rev Clin Esp. 199(5): 332-333.
- Sen H, Inangil G, Sahin L, Dere K, Ozkan S, et al., (2009) Ecthyma gangrenosum like lesions associated with methicillin resistant staphylococcus aureus infection. Int J Infect Dis. 13(4): e173-5.
- Athappan G, Unnikrishna A, Chandraprakasam S (2008) Ecthyma gangrenosum: presentation in a normal neonate. DOJ. 14(2): 17.
- Sevinsky LD, Viecens C, Ballesteros DO, Stengel F (1993) Ecthyma gangrenosum: a cutaneous manifestation of pseudomonas aeruginosa sepsis. J Am Acad Derm. 29(1): 104–106.
- Song WK, Kim YC, Park HJ, Cinn YW (2001) Ecthyma gangrenosum without bacteraemia in leukaemic patient. Clin Exp Dermatol. 26(5): 395-397.
- Chan YH, Chong CY, Puthucheary J, Loh TF (2006) Ecthyma gangrenosum: a manifestation of pseudomonas sepsis in three paediatric patients. Singapore Med J. 47(12): 1080-1083.
- Varghese GM, Eapen P, Abraham S (2011) Ecthyma gangrenosum of a single limb. Indian J Crit Care Med. 15(3): 188–189.





