Linear Pigmented Basal Cell Carcinoma: Exceptional Clinical Entity with Rare Localization
Saadani CH*, Assenhaji I, Gallouj S, Mernissi FZ
Faculty of Medicine, Department of Dermatology, CHU Hassan II, Fes, Morocco.
*Corresponding Author
C.H. Saàdani,
Department of Dermatology, CHU Hassan II, Fes, Morocco.
E-mail: ch.saadani@gmail.com
Received: February 21, 2018; Accepted : March 13, 2018; Published: March 14, 2018
Citation: Saadani CH, Assenhaji I, Gallouj S, Mernissi FZ. Linear Pigmented Basal Cell Carcinoma: Exceptional Clinical Entity with Rare Localization. Int J Clin Dermatol Res. 2018;6(1):160-161. doi: dx.doi.org/10.19070/2332-2977-1800036
Copyright: Saadani CH© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Linear BCC is a distinct clinical entity, first described by Lewis in 1985. The particular region was the most affected. Presence of the tumor along relaxing skin tension lines, increase in subclinical extension. It is suggested that margin controlled excision should be considered for linear BCC. We report a new case of linear pigmented basal cell carcinoma developed in the shoulder.
2.Introduction
3.Observation
4.Discussion
5.Acknowledgement & Declarations
6.Conclusion
7.References
Keywords
Basal Cell Carcinoma; Linear; Pigmented; Shoulder; Rare Localization.
Introduction
Basal cell carcinoma (BCC) is the most common human malignancy, and accounts for nearly 80% of all non melanoma skin cancers [1] Several morphologic and histologic variants of BCC have been reported [2]. Linear pigmented basal cell carcinoma is a distinct and rare morphological variant. The first case was described by Lewis in 1985, and since then only 37 cases have been reported [3]. The most common site is the periorbital region [4], especially the lower eyelid and malar region, and they were followed by cervical and trunk. The main of our case is to report a new case of linear pigmented basal cell carcinoma developed in the shoulder, which is a rare localization.
Observation
A 57-year-old man with no pathologic history had a linear pigmented lesion with onset 1 year earlier, on the right shoulder. The patient reported the notion of manipulation of a papule at the same site before the symptomatology. Clinical examination found a linear pigmented plaque measuring 4 cm, well limited, with erosions and crusts at its center (Figure 1). The differential diagnosis was essentially linear angiokeratomas. Dermoscopy revealed ovoid nests, a peripheral digitiform aspect, telangiectasia and arborizating vascularization and central ulceration, with no pigmented network (Figure 2). The diagnosis of pigmented basal cell carcinoma was confirmed by histology, which showed tumor proliferation of basaloid cells, arranged in palisaded cords, basophilic and sometimes pigmented cytoplasm, and retraction slits. Surgical excision with margins was performed, with histological study concluding a nodular and pigmented basal cell carcinoma, with healthy margins. No recurrence had occurred after 2 years of follow up (Figure 3).


Figure 1. Pigmented plaque with a linear arrangement on the right shoulder.

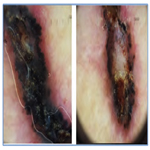
Figure 2. Dermoscopy: ovoid nests, a peripheral digitiform aspect, telangiectasia central ulceration.

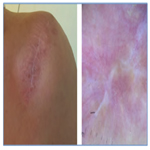
Figure 3. Clinical and dermoscopic control of the exeresis scar.
Discussion
Our case describes a rare form of linear pigmented basal cell carcinoma, with the same features reported in the literature. Nevertheless, the most frequent localization described was the periorbital region [4]. The location at the shoulder is exceptional. The majority of linear CBCs are oriented along the lines of tension of the skin, this linear arrangement can be explained by several mechanisms, including the koebner effect, as the case of our patient [5]. Dermoscopy is used to guide the diagnosis of CBC with ovoid nests, ulceration and telangiectasia. The diagnosis is confirmed by histology and nodular CBC represents the most reported histologic subtype. The orientation along the tension lines allows easy surgical excision with good healing. However, the lateral extension of the tumor requires excision with margins of safety.
Acknowledgement & Declarations
All authors contributed to the writing of this article. The authors also state that they have read and approved the final version. The authors declare no conflict of interest.
Conclusion
Pigmented and linear basal cell carcinoma is a rare morphological variant whose clinical, topographical and therapeutic characteristics must be known. Hence the interest of dermoscopy which has made it possible to correct the diagnosis allowing adequate management.
References
- Margo CE, Waltz K. Basal cell carcinoma of the eyelid and periocular skin. Surv Ophthalmol. 1993 Sep-Oct;38(2):169-92. PubMed PMID: 8235999.
- Sexton M, Jones DB, Maloney ME. Histologic pattern analysis of basal cell carcinoma: study of a series of 1039 consecutive neoplasms. J Am Acad Dermatol. 1990 Dec;23(6 Pt 1):1118-26. PubMed PMID: 2273112.
- Bittencourt F, Weis J, Paschoal F, Machado CD, Barbosa CP. Description and approach to a rare case of linear pigmented basal cell carcinoma. J Am Acad Dermatol. 2016 May 1;74(5):AB195.
- Mavrikakis I, Malhotra R, Barlow R, Huilgol SC, Selva D. Linear basal cell carcinoma: A distinct clinical entity in the periocular region. Ophthalmol. 2006 Feb 1;113(2):338-42. PubMed PMID: 16406534.
- Mavrikakis I, Malhotra R, Selva D, Huilgol SC, Barlow R. Linear basal cell carcinoma: A distinct clinical entity. J Plast Reconstr Aesthet Surg. 2006;59(4):419-23. PubMed PMID: 16756260.
- Pardavila R, Rosón E, De La Torre C, González B, Posada C, Feal C, et al., Linear basal cell carcinoma. Report of two cases. Actas Dermosifiliogr. 2007 Jan 1;98(4):291.





