Primary Cutaneous Large B Cell Lymphoma, Leg Type: Good Evolution of A Particular Location
A Lahlou*, S Elloudi, H Baybay, FZ Mernissi
Department of Dermatology, Hospital Center University Hassan Ii, Fez, Morocco.
*Corresponding Author
Asmae Lahlou,
Department of Dermatology, Hospital Center University Hassan Ii, Fez, Morocco.
Email : lahlouasmae@gmail.com
Received: August 22, 2016; Accepted : October 03, 2016; Published: October 06, 2016
Citation: A Lahlou, S Elloudi, H Baybay, FZ Mernissi (2016) Primary Cutaneous Large B Cell Lymphoma, Leg Type: Good Evolution of A Particular Location. Int J Clin Dermatol Res.4(3), 90-93. doi: dx.doi.org/10.19070/2332-2977-1600024
Copyright: A Lahlou© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Primary cutaneous large B-cell lymphoma, leg type, is a rare and aggressive neoplasm as defined by the recently updated World Health Organization–European Organization for Research and Treatment of Cancer classification of cutaneous lymphomas. We present a case of a 39-year-old men who presented with a cutaneous lesion on her back. Skin biopsy revealed pathology consistent with this entity. The patient was treated with systemic chemotherapy with rituximab combined with doxorubicin, cyclophosphamide, vincristine, and prednisone with a good evolution. Here, we review the available literature and summarize clinical features and management of this uncommon subtype of non-Hodgkin lymphoma.
2.Introduction
3.Case Report
5.Discussion
6.Conclusion
7.References
Keywords
B cell lymphoma; leg type; cutaneous lymphoma
Introduction
Primary cutaneous B-cell lymphomas are a heterogeneous group
of rare clonal B-cell lymphoproliferative disorders with distinct clinicopathological features compared with nodal counterparts [1]. Primary cutaneous diffuse large B-cell lymphoma-leg type (PCLBCL-LT) is a rare subtype which constitutes only 4% [2]. They have a predilection to the leg (72%), advanced age of onset (mean age, 76 years), high Bcl-2 expression (85%) and frequent relapses with extracutaneous dissemination [10-20%]. We report a case we report the case of a young patient of 39 years old who consulted for a hummocky tumor in the back whose histology was in favor of lymphoma B-type leg, , with good response to rituximab combined with doxorubicin, cyclophosphamide, vincristine, and prednison ( R-CHOP).
Case Report
A 39 year old men, presented with asymptomatic erythematous tumors hummocky, with a hard texture to touch, gradually increasing size (figure 1). histopathological examination revealed diffuse atypical, pleomorphic cells, menues hyperchromatic nuclei anisokaryosis and many mitoses (figure 2). Immunohistochemistry (IHC) revealed expression CD20 (figure 3), le Bcl 6 ( figure 4), and foccaly Bcl2 (figure 5), Proliferative index ki67 was very high, anti-CD3 antibody labeled reaction cells, CD10-, CD4-, and CD30- . Based on the clinical, histopathologic and the IHC examination, a diagnosis of primary cutaneous diffuse large B-cell lymphoma, leg type (PCLBLC,LT) was established. Lymph nodes were free, all evolving in a context of apyrexia and conservation condition. Further staging evaluation, including bone marrow biopsy and computed tomographic imaging, was unremarkable. The patient was subsequently started on systemic chemotherapy with rituximab combined with doxorubicin, cyclophosphamide, vincristine, and prednisone (R-CHOP) for eight cycles with a good evolution keeping just a scarred macula pigment in the back. He tolerated therapy well and remains free of disease approximately 1 year after her lymphoma diagnosis (figure 6).
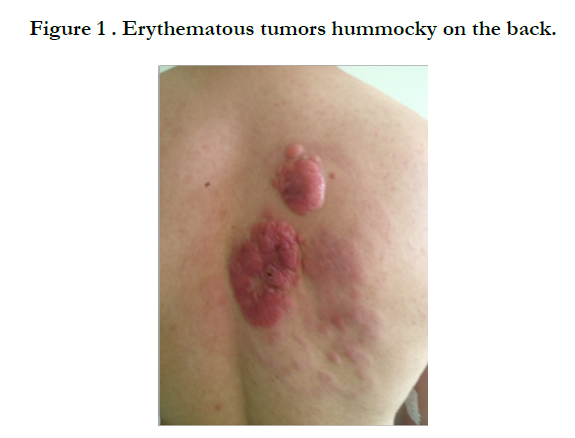

Figure 1 . Erythematous tumors hummocky on the back.
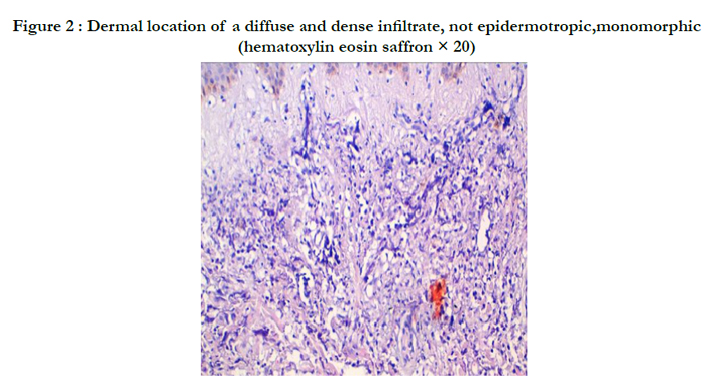
Figure 2 : Dermal location of a diffuse and dense infiltrate, not epidermotropic,monomorphic (hematoxylin eosin saffron × 20)
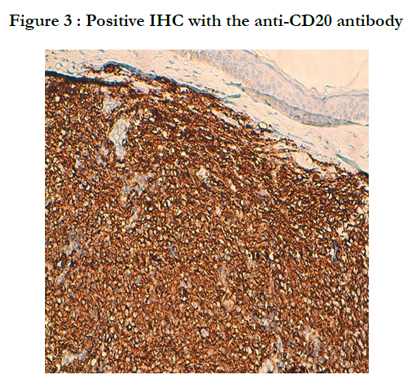
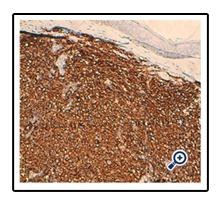
Figure 3 : Positive IHC with the anti-CD20 antibody
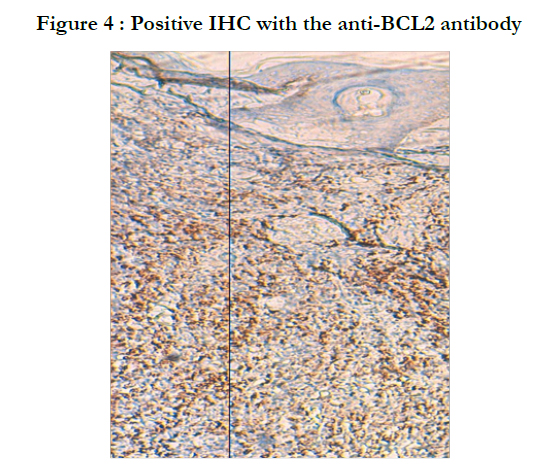
Figure 4 : Positive IHC with the anti-BCL2 antibody
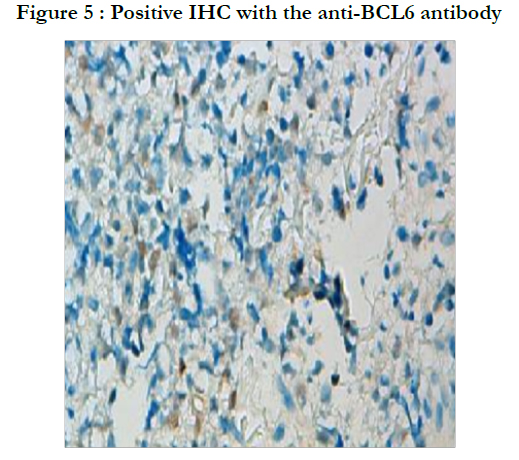
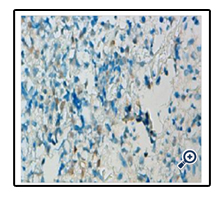
Figure 5 : Positive IHC with the anti-BCL6 antibody


Figure 6 : Clinical improvement after treatment with R-CHOP
Discussion
Primary cutaneous B-cell lymphoma (PCBCL) belongs to a distinct group of B-cell lymphoproliferative disorders defined by its presentation in the skin, without evidence of extracutaneous spread at the time of diagnosis [3]. Extranodal involvement occurs in approximately 25% of non-Hodgkin lymphomas, with the gastrointestinal tract being the most common site of extranodal involvement, followed by the skin [4]. The annual incidence of cutaneous lymphomas is approximately 0.5 to 1 per 100,000 [3]. While B-cell lymphomas account for the majority of nodal lymphomas, PCBCLs represent only 20% to 25% of all primary cutaneous lymphomas [5]. The pathogenesis of PCBCL is unclear. There is some speculation that PCBCL may represent a lymphoproliferative response to antigenic stimuli in the cutis, a skin-associated lymphoid tissue–related B-cell lymphoma [a process similar to mucosa-associated lymphoid tissue lymphomas in the gastrointestinal tract] [6]. In Europe, there is evidence linking Borrelia.
Burgdorferi infection to the development of PCBCL [4]. Jelic and colleagues reported borrelial serology in 12 of 22 (55%) PCBCL cases [7]. Another study evaluating cases of PCBCL in an area with endemic borrelia infections in the Scottish Highlands found B. burgdorferi–specifi c DNA in 35% of cases using polymerase chain reaction, with a statistically significant positive association between B. burgdorferi and PCBCL [8].
The subtype identified in our patient, PCLBCL, LT, represents approximately 20% of all PCBCLs and 4% of all cutaneous lymphomas [9, 10]. It is more common in the elderly, with a median age in the mid 70s [11, 12]. But our patient was young. The male to female ratio ranges from 1:3 to 1:4 [10, 12, 13]. Patients with PCLBCL, LT present with red to bluish nodules or tumors on one or both lower legs. Only about 10% to 15% of these patients are noted to develop lesions outside of the lower extremities, as was the case with our patient, who presented with a tumor on the back [10]. Compared with other subtypes of PCBCLs [primary cutaneous marginal zone lymphoma and primary cutaneous follicular center lymphoma], these tumors are more aggressive with worse outcomes, as they frequently disseminate to lymph nodes and visceral organs [1]. PCLBCL-LT typically realize tumors rapidly increasing in size, often multiple at diagnosis may be unilateral or bilateral in the lower limbs. Other areas may be affected, including the cephalic extremity and trunk as our patient, The extra leg location and uniqueness of the tumor are factors of good prognosis. [13,14], other factors such as young age in our patient may be involved. In fact studies have shown a survival rate at 3 years of 77% for other anatomical localization interesting seats against 43% for forms affecting lower limbs 4 and 87% in patients treated with rituximab and chemotherapy against 50% who received other types of treatment such as radiotherapy and chemotherapy [16-17].
Conclusion
Lymphomas primitive leg skin types B have a poor prognosis, with a rapidly unfavorable evolution,we think that young age and topography outside the leg remains good prognosis if treated with R-CHOP chemotherapy as like our patient.
References
- Hristov AC. (2012) Primary cutaneous diffuse large B-cell lymphoma, leg type: Diagnostic considerations. Arch Pathol Lab Med 136(8):876-81.
- Shaikh AJ, Masood N, Ahsan A, Memon W. (2008) Primary cutaneous B cell lymphoma – Leg type (NEW EORTC – WHO classification), with nasal sinuses involvement. J Pak Med Assoc 58(5):274-6.
- Siegel RS, Pandolfino T, Guitart J, Rosen S, Kuzel TM. (2000) Primary cutaneous B-cell lymphoma: review and current concepts. J Clin Oncol. 18(15):2908-25.
- Santucci M, Pimpinelli N. (2004) Primary cutaneous B-cell lymphomas.Current concepts. I. Haematologica 89(11):1360–1371.
- Senff NJ , Noordijk EM, Kim YH, Bagot M, Berti E, et al., (2008) European Organization for Research and Treatment of Cancer and International Society for Cutaneous Lymphoma consensus recommendations for the management of cutaneous B-cell lymphomas. Blood. 112(5):1600–1609.
- Slater DN. (1994) MALT and SALT: the clue to cutaneous B-cell lymphoproliferative disease. Br J Dermatol.131(4):557–561.
- Jelić S, Filipović-Ljesković I. (1999) Positive serology for Lyme disease borrelias in primary cutaneous B-cell lymphoma: a study in 22 patients; is it a fortuitous finding? Hematol Oncol 17(3):107–116.
- Goodlad JR, Davidson MM, Hollowood K, Ling C, MacKenzie C,et al.,(2000) Primary cutaneous B-cell lymphoma and Borrelia burgdorferi infection in patients from the Highlands of Scotland. Am J Surg Pathol.24(9):1279–1285.
- Huang CT, Yang WC, Liu YC, Lin SF. (2011) Primary cutaneous diff use large B-cell lymphoma, leg type, with unusual clinical presentation of bluishreddish multicolored rainbow pattern. J Clin Oncol. 29(17):497–498.
- Swerdlow SH, Campo E, Harris NL, Jaff e ES, Pileri SA, et al., (2008) WHO Classifi cation of Tumours of Haematopoietic and Lymphoid Tissues. 4th edn. Vol :2. Lyon, France: IARC Press,
- Grange F , Beylot-Barry M, Courville P, Maubec E, Bagot M, et al., (2007)Primary cutaneous diff use large B-cell lymphoma, leg type:clinicopathologic features and prognostic analysis in 60 cases. Arch Dermatol 143(9):1144–1150.
- Willemze R, Jaffe ES, Burg G, Cerroni L, Berti E, et al.,(2005) WHO-EORTC classification for cutaneous lymphomas. Blood 105(10):3768–3785.
- Senff NJ, Hoefnagel JJ, Jansen PM, Vermeer MH, van Baarlen J et al., (2007)R. Reclassification of 300 primary cutaneous B-cell lymphomas according to the new WHO-EORTC classifi cation for cutaneous lymphomas: comparison with previous classifi cations and identification of prognostic markers. J Clin Oncol. 25(12):1581–1587
- Grange F , Beylot-Barry M, Courville P, Maubec E, Bagot M et al.,(2007) Primary cutaneous diffuse large B-cell lymphoma, leg type: clinicopathologicfearures and prognostic analysis in 60 cases. Arch Dermatol.143(9): 1144-50
- Senff NJ , Hoefnagel JJ, Jansen PM, Vermeer MH, van Baarlen J (2007) Reclassification of 300 primary cutaneous B-Celilymphomas according to the new WHO-EORTe classification for cutaneous lymphomas: comparison with previous classifications and Identification of prognostic markers. J Clin Onco.125(12):1581-7
- Bekkenk MW, Postma TJ, Meijer CJ, Willemze R (2000) Frequency of central nervous system involvemenr in primary cutaneous B-celilymphoma. Cancer. 89(4):913-9
- Gimeno E, Gimenez MT, Alvarez-Larrán A, Gallardo F, Ferrer A, et al., (2009) Central nervous system invol¬vernent from primary cutaneous large B-celilymphoma of the leg. LeukRes 33(7):59-60





