Paraneoplastic Dermatomyositis: About 9 Patients
A Lahlou*, S Elloudi, H Baybay, FZ Mernissi
Departement of dermatology, hospital university, Hassan II, FEZ, Morocco.
*Corresponding Author
Asmae Lahlou,
Departement of dermatology, hospital university, Hassan II, FEZ, Morocco.
Email: lahlouasmae@gmail.com
Received: August 22, 2016; Accepted : September 29, 2016; Published: September 30, 2016
Citation: A Lahlou, S Elloudi, H Baybay, FZ Mernissi (2016) Paraneoplastic Dermatomyositis: About 9 Patients. Int J Clin Dermatol Res. 4(2), 87-89. doi: http://dx.doi.org/10.19070/2332-2977-1600023
Copyright: A Lahlou© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Dermatomyositis, a rare inflammatory disease possibly of autoimmune origin, produces a characteristic skin rash and symmetrical proximal myopathy. Patients with Dermatomyositis have a higher incidence rate of cancer, compared with the general population, since DM usually presents as a paraneoplastic syndrome. through the study of 9 cases of paraneoplastic dermatomyositis we will discuss the clinical feature, paraclinical, etiological, therapeutic and outcomes of paraneoplastic dermatomyositis (PDM) relative to the literature.
2.Introduction
3.Material and methods
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Dermatomyositis; Paranéoplastic; Autoimmune; Carcinoma.
Introduction
Dermatomyosis (DM) is a rare autoimmune myopathy involving a violation of the skeletal muscles and skin. It may be associated with cancer in adults. We report a serie of 9 cases to discuss the clinical feature, paraclinical, therapeutic and evolving our case paraneoplastic DM (PDM) from the literature.
Material and Methods
We retrospectively reviewed the clinical records of all patients hospitalized for DM in dermatology department at university hospital HASSAN II Fez during the period 2007-2015, including the case of DMP were selected.
Results
9 patients were included for this study among 25 patients with DM usually 36% of DM paraneoplastic (Figure 1), with 3 cases of nasopharyngeal carcinoma, 3 cases of breast cancer and one case of multiple myeloma, a case of gastric lymphoma, and one case of cancer rectum (Figure 2). Le sex ratio F / H was 3.5, the mean age was 48.6 years (38-65 years). The DM was indicative of neoplasia in all cases after a mean period of 7 months with an average time to diagnosis of DM 11.8 months (4-27 months).
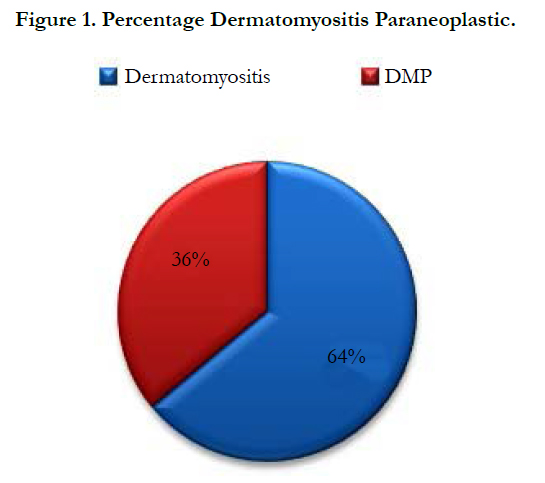
Figure 1. Percentage Dermatomyositis Paraneoplastic.
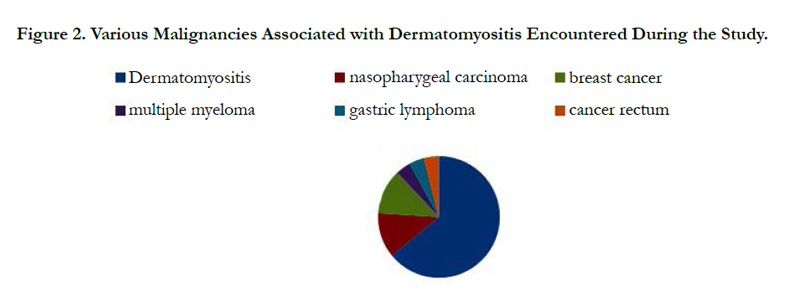
Figure 2. Various Malignancies Associated with Dermatomyositis Encountered During the Study.
Skin involvement was present in all patients. The mode of revelation was muscular in 14 cases. The demonstrations were extramuscular type of lung disease (3 cases), articular (3 cases) and gastrointestinal (5 cases). Muscle enzymes were elevated in all patients, and the inflammation was present in 4 cases. In all cases no noted vasculitis dermal in histology. The treatment was based on prolonged corticosteroid therapy and synthetic antimalarials drugs in all cases and the management of associated cancer. The evolution was marked by clinical and laboratory remission in 1 case after 2 years of decline, death in one patient, 4 patients are being monitored and 3 patients were lost to follow (Figure 3, 4).
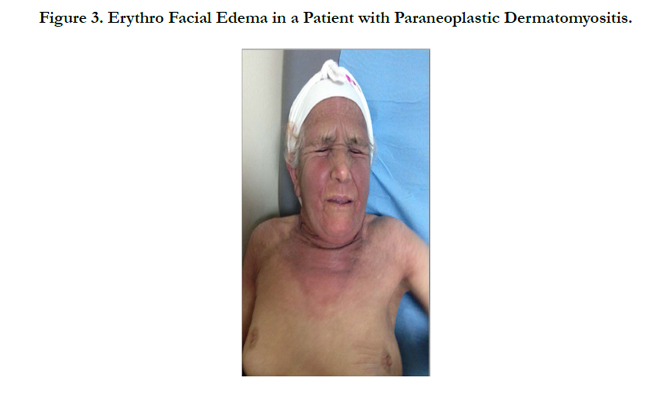

Figure 3. Erythro Facial Edema in a Patient with Paraneoplastic Dermatomyositis.
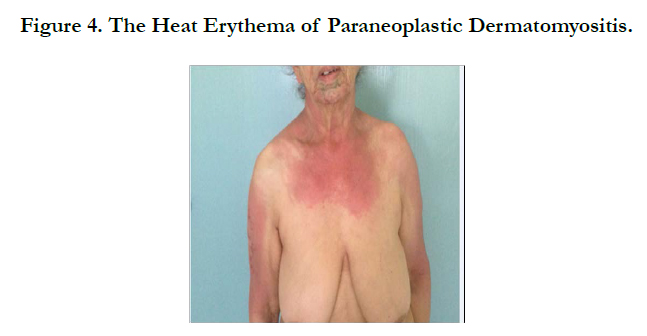

Figure 4. The Heat Erythema of Paraneoplastic Dermatomyositis.
Discussion
Dermatomyositis (DM) is a rare, autoimmune disease of the connective, which is associated with immune complex deposi¬tion and subsequent inflammatory cell accumulation [1]. The incidence rate of tumors in patients with DM has been reported to display a variable frequency of 0.6-1.0 per 100,000 individuals [2]. Diagnosis of dermatomyositis is associated with a higher risk of malignances, including the ovary, lung, pancreas, stomach, colorectal cancer and non-Hodgkin lymphoma particularly for patients aged >40 years [3]. Approximately 30% of the patients are left with mild to severe disability though the prognosis has been obviously improved. Age and association with tumor are risk factors associated with poor prognosis. DM often presents as a paraneoplastic syndrome, thus implying the presence of a tumor [4]. A probable hypothesis for the development of DM is that shared immunological processes link malignancy with myopathy [5].
A diagnosis of adult dermatomyositis compels us to exclude a possible paraneoplastic etiology. According to the largest series, 15% to 25% of cases of adult dermatomyositis are associated with cancer however our series is characterized by the high frequency of malignancy (36%) [3, 6]. This risk is present even in cases of amyopathic dermatomyositis [7, 8].
The DM can precede, coincide with, or develop after the diagnosis of cancer [9]. In our case the DM was revealing where the breast and nasopharyngeal were the most frequent. This neoplastic association with poor prognosis hence the importance of early diagnosis. The pathogenesis is multifactorial and some clinical or laboratory criteria are suggestive. We discovered cases of DMP advanced stage in our series despite the absence of neoplasia criteria. No consensus exists regarding the extent or frequency of the balance sheet to achieve in a subject with DM. The agents including corticosteroids and immunosuppressive drugs are always used in the treatment of dermatomyositis. The purposes of treatment are to improve the ability of daily living by increasing muscle strength and to alleviate extramuscular manifestations, including rash,dysphagia, dyspnoea, arthralgia and fever. But The treatment of DMP is based on the treatment of tumor underlying and immunosuppressants, however, the development of targeted therapies could change this therapeutic approach in the near future.
Conclusion
TThe PDM is frequent hence the interest to recall the need for a full investigation before each case DM even outside predictive of neoplasia signs.
References
- Mastaglia FL, Phillips BA (2002) Idiopathic inflammatory myopathies: Epidemiology, classification, and diagnostic criteria. Rheum Dis Clin North Am. 28(4): 723-741.
- Dalakas MC, Hohlfeld R (2003) Polymyositis and dermatomyositis. Lancet. 362: 971-982.
- Hill CL, Zhang Y, Sigurgeirsson B, Pukkala E, Mellemkjaer L, et al., (2001) Frequency of specific cancer types in dermatomyositis and polymyositis: A popu¬lation based study. Lancet. 357: 96-100.
- Callen JP (2001) Relation between dermatomyositis and polymyositis and cancer. Lancet. 357: 85-86.
- Buchbinder R, Hill CL (2002) Malignancy in patients with inflammatory myopathy. Curr Rheumatol Rep. 4: 415-426.
- Ungpraset P, Leeaphorn N, Hosiriluck N, Chaiwatcharayut W, Ammannagari N, et al., (2013) Clinical features of inflamma-tory myopathies and their association with malignancy: A systematic review in Asian population. ISRN Rheumatol. 509354.
- El-Azhary RA, Pakzad SY (2002) Amyopathic dermatomyositis: Ret-rospective review of 37 cases. J Am Acad Dermatol. 46(4): 560-565.
- Cao H, Parikh TN, Zheng J (2009) Amyopathic dermatomyositis ordermatomyositis- like skin disease: Retrospective review of 16 cases with amyopathic dermatomyositis. Clin Rheumatol. 28(8): 979-984.
- Callen JP, Wortmann RL (2006) Dermatomyositis. Clin Dermatol. 24(5): 363-373.





