Rapid Recovery from Skin Warts by Explicit Homeopathic Medicines
Swami S*, Pradhan AK
Monk in Charge of Medical Unit at Belur Math, Ramakrishna Mission Charitable Dispensary, Belur Math, Howrah, West Bengal, India.
*Corresponding Author
Swami Shraddhamayananda,
Monk in Charge of Medical Unit at Belur Math,
Ramakrishna Mission Charitable Dispensary,
Belur Math, Howrah, West Bengal,
Pin Code: 711202, India.
Tel: 91-9143415986
E-mail: gopalmj.belurmath@gmail.com
Received: October 10, 2015; Accepted: November 12, 2015; Published: November 13, 2015
Citation: Swami S, Pradhan AK (2015) Rapid Recovery from Skin Warts by Explicit Homeopathic Medicines. Int J Clin Dermatol Res. 3(5), 71-75. doi: dx.doi.org/10.19070/2332-2977-1500019
Copyright: Swami S© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
One hundred patients suffering from warts were treated with homeopathic medicines resulting shortening of the duration of illness, thus a probable diminishing role of the spread of such infections. However, it was found that Dulcammara was effective on verruca vulgaris and plana, Natrum mur was effective on pulmo-planter warts and Thuja was effective on Digitate warts.
2.Materials and Methods
2.1.The patients
2.2.The homeopathic medicines
3.Results
3.1.Results of the pilot study
3.2.Age and sex distribution of the patients
3.3.Outcome of the final study
4.Discussion
5.Conclusion
6.References
Introduction
Human papillomaviruses (HPVs) under the Papillomavirus family are common agents for producing skin warts in adults; as well as in children, throughout the globe. Although the frequency is unknown, warts are estimated to affect approximately 7-12% of the population. In school-aged children, the prevalence is 10-20%. An increased frequency also is seen among immunosuppressed patients and meat handlers. It is now well known that various HPV types are acquired in early infancy [1] and they persist for a pretty long time in the skin as observed by many scientists-even up to more than 60 years [2-4], and parental sharing of these viruses has also been noted [2, 4], although horizontal transmission from other persons is also an important way to spread this disease [4]. There are more than 200 types, of which 100 has been sequenced. Distinct histopathological types are also attributed to different skin HPVs particularly types 1, 2, 3, 4, 27 and 57 [5]. Verruca vulgaris is the commonest wart, although other types like planter and flat warts are not uncommon. Warts are usually highly prevalent in lower age groups and then gradually decrease with age [6], with no sex preponderance [7]. In a Taiwan study hand warts were found in 2.8 per cent of school children [8]. Warts or Verrucae are of different clinical types, depending on the morphology of the warts, the site affected and the mode of transmission. HPVs affect human skin and the moist membranes such as the throat, mouth, feet, fingers, nails, anus and cervix. It is a self limiting disease and in most of the cases spontaneous resolution takes place within 2yrs. The primary clinical manifestations of HPV infection include common warts, genital warts, flat warts, and deep palmoplantar warts. Most known HPV types cause no symptoms to humans but they may cause cosmetic disfigurement or tenderness. Plantar warts can be painful, and extensive involvement on the sole of the foot may impair ambulation. A small number can increase the risk of cancers specially if the lesion persists for a long time in cervix and vagina, penis, anus and oropharynx (HPV 16 and 18 strains). The CDC observed that over 70 percent of infections in young females clear up within 12 months, while 90% do so within 24 months. There are 40 types of HPVs which are transmitted sexually, affecting ano-genital areas, the other types are transmitted by personal contact or indirect transmission from using untreated swimming pool, fomites etc. or by auto-inoculation. Persistent long-term HPV infection raises the risk of developing precancerous lesions of the cervix and other region. However, in the majority of cases, cancer can be prevented. Among different types, types 16, 18, 33, 35, 45, 51, 52, 56, 58, 59, 68, 73, and 82 can cause cancer - they are carcinogenic and are sexually transmitted. The HPV virus enters the human body through a small cut, tear, or abrasion on the epidermis; the primary mode of transmission is through skin-to-skin contact. In our clinic, we first made a pilot study with 45 patients and then planned a master study with 100 such skin HPV infected patients who were treated with homeopathic medicines, along with a control group of 10 cases treated only with placebo containing the vehicle of the original medicine. Details of our findings are given in the following sections.
Materials and Methods
The patients were selected from the general patients attending our dermatology clinic; they were properly counselled as per our institutional ethical committee guidelines, which also had given permission for this study. All demographic records of the patients were maintained, and after final diagnosis by our dermatology consultant, the patients were enrolled for the study. All the patients were instructed to attend the clinic monthly up to 2 yrs as follow ups.
Only three medicines (Thuja oc. 1000, Dulcammara 100 and Nat. Mur 1000) were used in this study and they were given following the results of our pilot study with 45 cases which are given in the results section. Thus in Cauliflower like growth, Thuja was given; in palm and sole variety, Nat. Mur. and in other clinical types Dulcammara was administered. All medicines were used orally without any local application. The medicines were selected and administered in the following groups: Sixty patients with common warts (verruca vulgaris types 1, 2, 4, 7 and verruca plana types 3, 10, 28, 49 which were present in face, extremities and on other parts of the body were treated with dulcammara. Twenty five patients with Palmoplanter warts types 1, 2, 4, 63 were treated with Nat. Mur and fifteen patients with Filiform (digitate) warts were treated with Thuja Oc. The same medicine was given to each group of patients except in the control group where only lactose pills were given which appears similar to the medicines and lactose was the vehicle of these medicines. The medicine was purchased from reputed homeopathic medicine shop (HAPCO) in Kolkata. In the placebo group there were 5 males and 5 females. Random selection was done of both sexes, of different casts and ages. Medicines were given as 4 pills (one dose) weekly for 15 days then one dose in 15 days intervals. Only single oral homeopathic medicine was used for each group of patients without any local application.
Results
All the three different types of warts as described above were separately grouped with 15 patients in each group and for each medicine 5 patients were enrolled with altogether 45 patients studied. Detailed of this pilot study with results are given in Table 1. This study indicates that Dulcammara was effective in verruca vulg. and plana, Nat. Mur. was effective in Palmo planter type and Thuja was effective in Digitate variety.
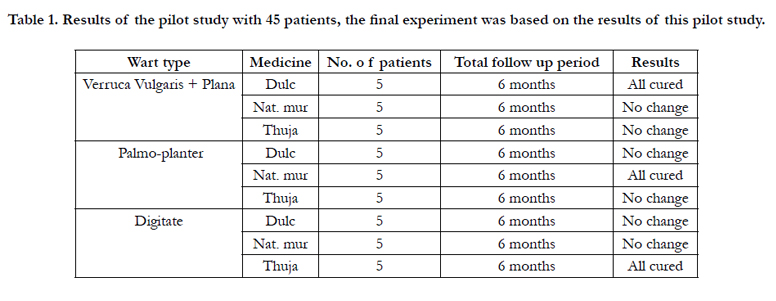

Table 1. Results of the pilot study with 45 patients, the final experiment was based on the results of this pilot study.
Total 100 patients were enrolled in this study. There were also 10 control cases in this study, those were given placebo and followed 2 years to see if there was any change. Most of them aged between 11 to 30 yrs (56%), their mean age was 19 yrs. Beyond 30 yrs of age there were 30 patients ( 25% of total patients ). Frequency distribution of different age groups are given in Graph 1. Most of the patients were in the age groups in between 11-30 years. Sex distribution was equal (1:1). Graph 2. Lesions on different sites in all the patients according their age groups are given in the Table 2. All the cases were diagnosed, categorized and followed up by our Dermatologist of the institution.
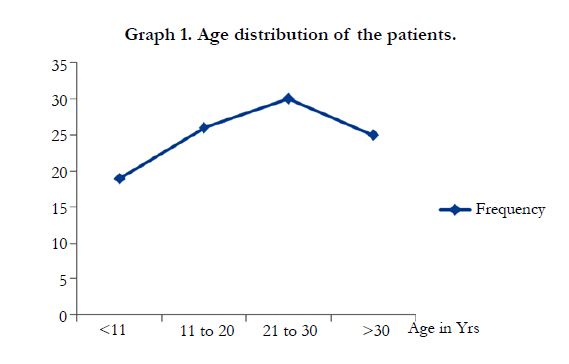
Graph 1. Age distribution of the patients.
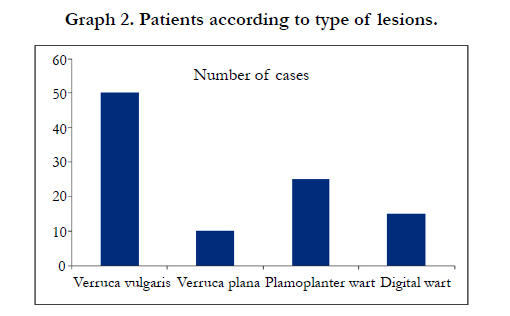
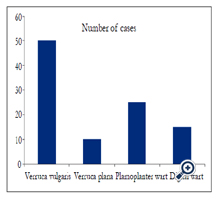
Graph 2. Patients according to type of lesions.
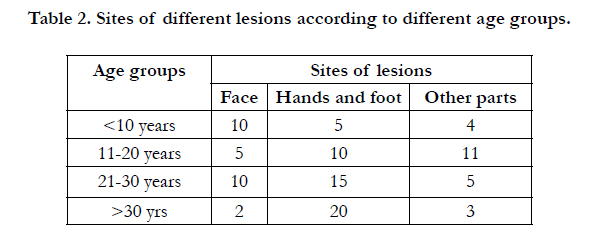
Table 2. Sites of different lesions according to different age groups.
Earliest positive response was seen in majority number cases within a month and 90 patients were cured within 3-4 months. Delayed response was noticed in 10 cases after 6-8 months of treatment. After two years follow up, we have seen relapse in three cases. In placebo cases, after 6 months follow-up, out of 10 patients no change occurred in 6 patients, but in 2 cases few lesions were increased and the remaining 2 patients discontinued treatment after second visit (1 month). Pictures of three such patients treated with homeopathic medicines are given in Figure 1-6. All the patients were followed for 2 years.
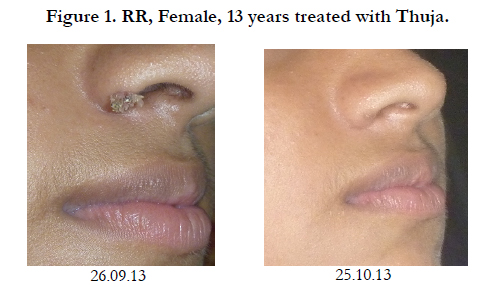

Figure 1. RR, Female, 13 years treated with Thuja.

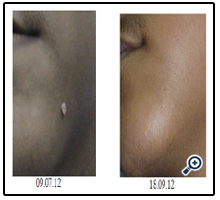
Figure 2. IS, Male, 15 years treated with Thuja.
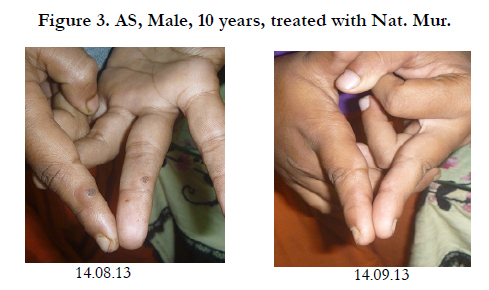

Figure 3. AS, Male, 10 years, treated with Nat. Mur.
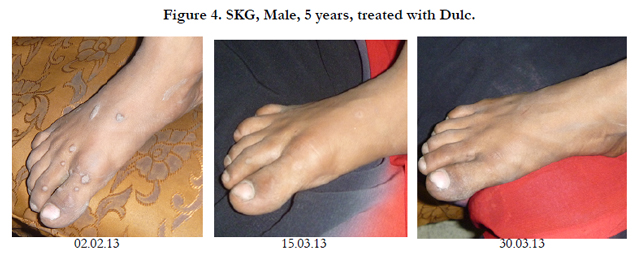

Figure 4. SKG, Male, 5 years, treated with Dulc.


Figure 5. MDG, Male, 10 years, treated with Dulc.


Figure 6. SS, Female, 35 years, treated with Dulc.
Discussion
In a recent study, it was found that HPV lesions usually completely resolved in about 70% cases within 12 months and in 90% cases within 24 months and it was observed that conventional treatments could not shorten the time to resolution [4]. There is no specific conventional treatment today for HPV infection.However, some medications and/or surgical interventions are sometimes prescribed/used for patients with HPV infections: (a) Salicylic acid may gradually remove the warts, one layer at a time. They can be bought without a prescription; they are OTC (overthe- counter) medications. They should not be used for genital warts as they may irritate. (b) Trichloroacetic acid burns off the warts in the genital area. (c) Podofilox (Condylox) may be used for the treatment of genital warts. (d) Cryotherapy where the warts are frozen with liquid nitrogen. They freeze and fall off. (e) Laser surgery in which the warts are removed by burning. (f) Surgical removal of the wart. (g) Electrocautery in which an electrical current is used to "zap" (burn off) warts or lesions. In most cases, however, the majority of infections clear up by themselves. Some experts believe total elimination by the immune system does not occur, it just becomes undetectable. Whether or not the individual is still infectious in such cases, is hard to know for certain. This study indicated a definite role of homeopathic medicines in the early resolution of HPV lesions. The real mechanism of action of these homeopathic medicines is very difficult to explain and there is no definite explanation of the mechanism of action of these medicines so far. Thus possible attempts should be made in future studies to find out the real mechanism of these medicines.
Conclusion
The result of this study was encouraging. It is not only helpful to control the spread of the disease within short time but also indicating a definite role of homeopathic medicine in HPV infection and the risk of pre cancerous stage can be prevented.
References
- Antonsson A, Karanfilovska S, Lindqvist PG, Hansson BG (2003) General acquisition of human papillomavirus infections of skin occurs in early infancy. J Clin Microbiol 41(6): 2509-2514.
- Hsu JY, Chen AC, Keleher A, McMillan NA, Antonsson A (2009) Shared and persistent asymptomatic cutaneous human papillomavirus infections in healthy skin. J Med Virol 81(8): 1444–1449.
- Hazard K, Karlsson A, Andersson K, Ekberg H, Dillner J, et al. (2007) Cutaneous human papillomaviruses persist on healthy skin. J Invest Dermatol 127(1): 116-119.
- Gottschling M, Göker M, Köhler A, Lehmann MD, Stockfleth E, et al. (2009) Cutaneotropic human beta-⁄ gamma-papillomaviruses are rarely shared between family members. J Invest Dermatol 129(10): 2427-2434.
- Gross G, Pfister H, Hagedorn M, Gissmann L (1982) Correlation between human papillomavirus (HPV) type and histology of warts. J Invest Dermatol 78(2): 160-164.
- Steele K, Irwin WG, Merrett JD (1989) Warts in general practice. Ir Med J 82(3): 122-124.
- Tamer E, Ilhan MN, Polat M, Lenk N, Alli N (2008) Prevalence of skin diseases among pediatric patients in Turkey. J Dermatol 35(7): 413-418.
- Chen GY, Cheng YW, Wang CY, Hsu TJ, Hsu MM, et al. (2008) Prevalence of skin diseases among schoolchildren in Magong, Penghu, Taiwan: a community-based clinical survey. J Formos Med Assoc 107(1): 21-29.





