Prevalence of Low Vitamin D and Disability Among Egyptian Female Patients with Rheumatoid Arthritis
Abogamal AF1*, Yasein YA2, Mansour AE2, Nassar Y3, Mahmoud E4, Abdalaziz AF5, Mustafa MS5
1 Associate Professor of Rheumatology & Rehabilitation, Faculty of Medicine, Department of Rheumatology & Rehabilitation, Al-Azhar University,Cairo, Egypt.
2 Lecturer of Public Health and Community Medicine, Faculty of Medicine, Department of Public Health and Community Medicine, Al-Azhar University,Cairo, Egypt.
3 Lecturer of Internal Medicine, Faculty of Medicine, Department of Internal Medicine, Al-Azhar University, Cairo, Egypt.
4 Lecturer of Endocrinology, Faculty of Medicine for Girls, Department of Endocrinology, Al-Azhar University, Cairo, Egypt.
5 Associate Professor of Clinical Pathology, Faculty of Medicine, Department of Clinical Pathology, Al-Azhar University, Cairo, Egypt.
*Corresponding Author
Ahmed F. Abogamal,
Associate professor of Rheumatology & Rehabilitation , Department of Rheumatology & Rehabilitation,
Faculty of Medicine, Al-Azhar University, Cairo, Egypt.
Tel: 002 01001972099
Fax: 002 0225102540
E-mail: abogamal15@gmail.com
ahmedfathy15@yahoo.com
Received: March 29, 2016; Accepted: November 04, 2016; Published: November 07, 2016
Citation: Abogamal AF, Yasein YA, Mansour AE, Nassar Y, Mahmoud E, et al., (2016) Prevalence of Low Vitamin D and Disability Among Egyptian Female Patients with Rheumatoid Arthritis. Int J Bone Rheumatol Res. 3(7), 56-61. doi: http://dx.doi.org/10.19070/2470-4520-1600012
Copyright: Abogamal AF© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Vitamin D deficiency was reported to be common in rheumatoid arthritis patients and an association with
female sex, disease severity, higher disease activity and worse quality of life was suggested.
Objectives: To estimate the prevalence of different levels of vitamin D and disability among female patients with rheumatoid
arthritis, and to investigate its possible impact on the degree of disability in rheumatoid arthritis.
Subjects & Methods: A cross sectional hospital-based survey conducted during the year 2015-2016. Total number of
patients included in the study was 160, with a mean age of 44.80 ± 3.69 years. The data was collected through an interview
questionnaire from all participants over a period of one month (November 2015).
Results: The prevalence of low levels of vitamin D and disability among rheumatoid arthritis patients was 54.4% and 63.7% respectively. There was no statistically significant difference between different levels of vitamin D regarding age and duration of rheumatoid arthritis (P > 0.05). Class IV and III of disability was commonly reported among rheumatoid arthritis patients with a disease duration of more than 5 years and represented 27.3% and 24.5% respectively, and there was statistically significant difference (P < 0.05). There was a significant association between different classes of disability and different levels of vitamin D (χ2 = 15.28, P < 0.05).
Conclusion: It appears that low vitamin D is highly prevalent in patients with rheumatoid arthritis and that vitamin D insufficiency and deficiency may be linked to disease impact on functional ability and disability.
2.Introduction
3.Patients and Methods
3.1.Study Design & Setting
3.2.Study Sample
3.3.Data Collection
3.4.Data Analysis
4.Results
5.Discussion
6.Conclusion
7.Acknowledgements
8.References
Keywords
Prevalence; Vitamin D; Disability; Rheumatoid Arthritis; Female Patients; Egypt.
Introduction
Rheumatoid arthritis is a chronic autoimmune disease characterized by loss of self-tolerance leading to immune activation particularly against synovial tissues [1].
The presence of rheumatoid arthritis is associated with chronic long standing synovitis, and juxtaarticular osteoporosis of the synovial joints, with a resultant multiple joint pain, inflammation, erosions and deformities [2-7].
The chronicity of the disease, bone and joint lesions are associated with decreased patient’s functional capacity at the level of daily living, vocational and a vocational activities and a higher disability index [8-16].
Vitamin D is the main player for the musculoskeletal health, bone, and muscle metabolism. Many observational studies have determined positive clinical relationships between vitamin D serum concentration, physical performance, and muscle fatigue, muscle and bone mass [17-24].
Vitamin D deficiency was reported to be common in rheumatoid arthritis patients and an association with female sex, disease severity, higher disease activity and worse quality of life was suggested [25-27].
On the other hand Several RCTs and meta-analyses have investigated the effect of vitamin D supplementation on musculoskeletal system and reported a patient significant benefit at many levels, including muscle strength, fatigue, bone mass, risk of fall and over all physical performance [28-36].
The current study was conducted to estimate; the prevalence of different levels of vitamin D and disability among female patients with rheumatoid arthritis, and to investigate its possible impact on the degree of disability in rheumatoid arthritis.
The coexistence of long standing RA and vitamin D deficiency suspected to have a significant negative impact on patients function, and that’s why we initiated this study to evaluate the prevalence of vitamin D deficiency in RA patients and, the coexistence impact on patient function.
Patients and Methods
The current study was based on a cross sectional hospital-based survey, conducted among patients presenting at outpatient rheumatology clinics of Al-Azhar University Hospitals, Egypt between 2015-2016.
- Patients with Rheumatoid arthritis according to ACR 2010 criteria for diagnosis of RA [37].
- At least 3 years of disease duration.
- Female.
- Patients receiving stable doses of conventional DMARDs in the form of Methotrexate, Hydroxychloroquin, and NSAIDS.
- Patients taking vitamin D supplement.
- Patients with parathyroid dysfunction.
- Patients with chronic illness affecting vitamin d metabolism, e.g. chronic kidney, renal disease or mal absorption syndromes.
- Patients with active rheumatoid arthritis, Disease Activity Score 28 (DAS28) more than 2.6 [38].
- Pregnancy or breast feeding.
Al-Azhar University Hospital contains 2 outpatient rheumatology clinics (Al-Hussein University hospital clinic and El-Sayed Galal University hospital clinic). The both clinics were included in the study. All female patients attended the both clinics for any purposes during the period of data collection (through November 2015) and met the inclusion criteria were asked to be included in the study and the only 160 patients accepted. Oral consent was obtained from every participant before taking place in the study with nearly 70% response rate.
The data was collected through an interview questionnaire from all participants. Field survey was conducted after obtaining approval from local authority (Hospital administration). The data was collected through one month (November 2015). The field work took 2 days/weeks for every clinic. The average number of women interviewed per day was 10-12 and the time needed to complete the questionnaire was 5-10 minutes.
All patients were subjected to the following:
(A). Full clinical assessment.
(B). Functional according to The American College of Rheumatol ogy 1991 revised criteria for the classification of global functional status in rheumatoid arthritis:
- Class I = able to perform usual activities of daily living (selfcare,vocational, and avocational);
- Class II = able to perform usual self-care and vocational activities, but limited in avocational activities;
- Class III = able to perform usual self-care activities but limited in vocational and avocational activities.
- Class IV = limited in ability to perform usual self-care, vocational, and avocational activities.
Usual self-care activities include dressing, feeding, bathing, grooming, and toileting; vocational and avocational activities are both patient-desired and age-, and sex-specific, patients were questioned about thier ability in the last month [39].
25-Hydroxy Vitamin D concentrations were determined by using a Radio Immunoassay (DiaSorin 25-OH-D assay Stillwater, Minnesota 55082-0285, U.S.A.) This kit was purchased from Gamma Trade Egypt. The instrument used was (Isocom). Principle of the assay: The DiaSorin 25-OH-D assay consists of a two-step procedure. a) The first procedure involves a rapid extraction of 25-OH-D and other hydroxylated metabolites from serum or plasma with acetonitrile. b) Following extraction, the treated sample is then assayed using an equilibrium RIA procedure. The RIA method is based on an antibody with specificity to 25-OH-D. The sample, antibody and tracer are incubated for 90 minutes at 20- 25°C. Phase separation is accomplished after 20 minute incubation at 20-25°C with a second antibody precipitating complex. A NSB/Addition buffer is added after this incubation prior to centrifugation to aid in reducing non-specific binding. The ranges of vitamin D were : 1) sufficiency: equal or more than 30ng/ml, 2) insufficiency: from 10-30ng/ml, and 3) deficiency: less than 10ng/ml [40].
Data was entered, organized, tabulated and analyzed using the standard computer program SPSS version 21. Quantitative data were expressed as Mean ± SD, while Qualitative data were expressed as frequency and percent. Chi square (Χ²) was used to assess the relationship between two qualitative variables, with the significant level set at 0.05.
Results
The study included 160 participants female. All participants suffered from rheumatoid arthritis with a mean age of 44.80 ± 3.69 years.
The findings revealed that, the prevalence of low levels of vitamin D and disability among rheumatoid arthritis patients was 54.4% and 63.7% respectively.
Table (1) Displays the prevalence of different levels of vitamin D among the studied sample. It shows that, the prevalence of vitamin D sufficiency was 45.6%, insufficiency was (33.1%), and deficiency was (21.3%).


Table 1. Prevalence of Different Levels of Vitamin D Among Studied Sample.
Table (2) Clarify the prevalence of different classes of disability among the studied sample. The results revealed that; the prevalence of class I of disability was (36.2%), class II (18.1%), class III (24.4%) and class IV (21.3%).
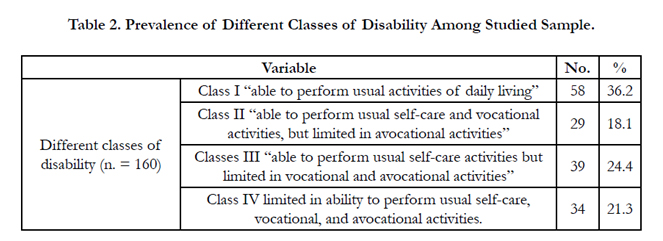
Table 2. Prevalence of Different Classes of Disability Among Studied Sample.
Table (3) Displays the distribution of different levels of vitamin D among the studied sample according to age and duration of rheumatoid arthritis. It shows that, there was no statistically significant difference between different levels of vitamin D among studied sample regarding age and duration of rheumatoid arthritis disease (P > 0.05).
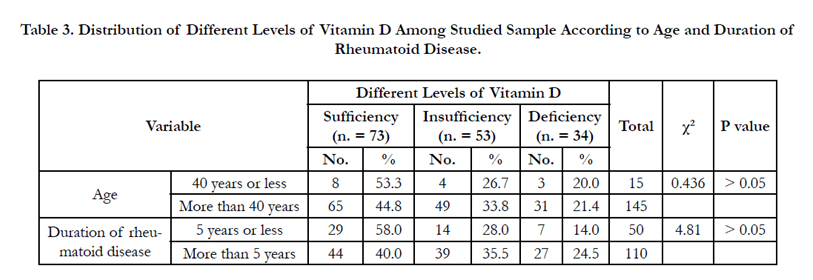
Table 3. Distribution of Different Levels of Vitamin D Among Studied Sample According to Age and Duration of Rheumatoid Disease.
Table (4) Shows the distribution of different classes of disability among the studied sample according to the duration of rheumatoid arthritis. It reveals that, class IV and III of disability was commonly reported among rheumatoid patients with a disease duration of more than 5 years and represented 27.3% and 24.5% respectively, and there was a statistically significant difference (P < 0.05).
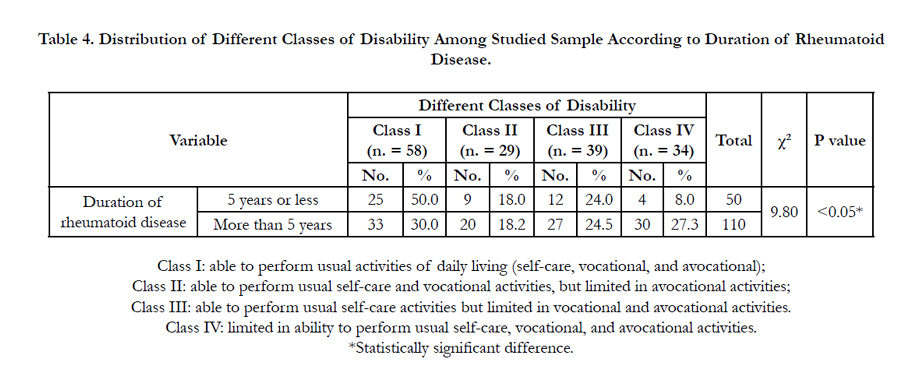
Table 4. Distribution of Different Classes of Disability Among Studied Sample According to Duration of Rheumatoid Disease.
Table (5) Presents the relationship between different classes of disability and different levels of Vitamin D among the studied sample. It reveals a significant association between different classes of disability and different levels of vitamin D (Χ² = 15.28, P < 0.05), where class IV of disability was commonly prevalent among rheumatoid arthritis patients with vitamin D deficiency (41.2%) and insufficiency (17.0%), compared with (15.1%) among patients with sufficiency level. A similar finding was observed also with class III, where class III of disability was more reported among patients with vitamin D deficiency (26.5%) and insufficiency (26.4%), compared with (21.9%) among patients with sufficiency level.
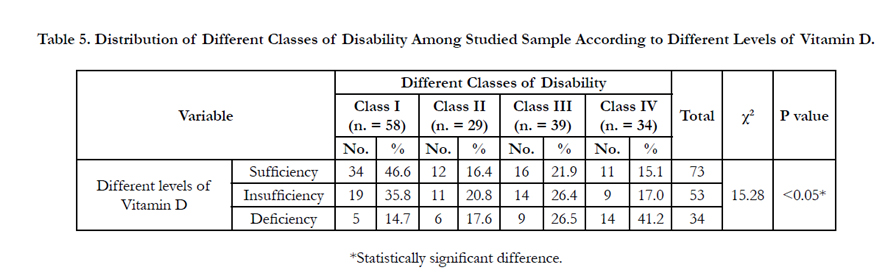
Table 5. Distribution of Different Classes of Disability Among Studied Sample According to Different Levels of Vitamin D.
Discussion
Vitamin D plays an important role in the integrity of the musculoskeletal system, and the coexistence of its deficiency with long standing rheumatoid arthritis could negatively affect patient functional abilities.
In the present study we assessed the level of Vitamin D in longstanding RA patients. Low vitamin D was detected, in 87 (54.4%) patients, insufficiency in 53 (33.1%) patients, deficiency in 34 (21.3) patients, and sufficiency was found in 73 (45.6%) patients. So according to our study results, low Vitamin D is very prevalent in rheumatoid arthritis patients, which came in agreement with Abourazzak and his colleagues as they investigated the vitamin D level in 170 rheumatoid arthritis patients and reported that low vitamin D is very common in rheumatoid arthritis patients [25].
In other similar studies that investigate the level of Vitamin D in rheumatoid arthritis patients, Ranganathan, et al., detected 68% of rheumatoid arthritis patients with low Vitamin D [26]. While Raczkiewicz and his colleagues detect a higher percentage of low Vitamin D 76.3% in rheumatoid arthritis patients which support our results [27].
In our study Rheumatoid arthritis patients were further sub grouped according to their functional ability, by ACR 1991 revised criteria for functional status. Normal functional ability (Class I) were detected in 58 (36.2%) patients, while limited functional status found in 102 (63.7%) patients. The grades of diminished functional ability (class II, III, IV), are 29 (18.1%), 39 (24.4%), 34 (21.3%) patients respectively.
A significantly lower functional ability was found in rheumatoid arthritis patients with disease duration of more than 5 years as P < 0.05, in comparison to patients with less disease duration.
Rheumatoid arthritis and disability has been studied and investigated in many studies with the established concept that rheumatoid arthritis negatively affects patient function and quality of life [40-42]. The current results, efficiently represent the substantial negative impact of rheumatoid arthritis on patient functional performance. This finding supported by the National Institute of Clinical Excellence who recommended that, rheumatoid arthritis patient should be regularly assessed for thier functional ability [43].
Sufficient vitamin D, is essential for muscle performance, bone mass, fitness, fall prevention, and normal physical activity [17, 19, 20, 23]. Its insufficiency is associated with poor quality of life, and poor functional ability especially in patients with rheumatoid arthritis [27].
In-depth analysis of the current study, shows a statistically significant positive association between the disability class and vitamin D deficiency (P < 0.05), higher vitamin D level is associated with better functional performance and a lower disability class. Which may represents a significant value for vitamin D, on functional ability of rheumatoid arthritis patients. This negative impact furthermore is expressed by the presence of higher disability classes among the groups having low Vitamin D, as class IV functional ability was 41.2% in patients with the vitamin D deficiency group, and insufficiency 17.0%, compared with 15.1% among patients with normal vitamin D level.
Our results are supported by Raczkiewicz and his colleagues, where they studied 97 consecutive rheumatoid arthritis patients for vitamin D level and functional ability, and stated that "vitamin D deficiency is highly prevalent in rheumatoid arthritis patients and is associated with worse quality of life indices, and higher vitamin D levels is associated with better functional ability" [27].
Grazio et al., in their assessment to the same relation found an association between low vitamin D and disability in rheumatoid arthritis patients, which supports our results [44]. Similar findings are also reported by Furuya et al., who found that, high disability indices were more common among rheumatoid arthritis patients with low vitamin D [45].
According to our results we recommend assessment of vitamin D status in patients with rheumatoid arthritis to detect and correct hypovitaminosis D, which may help to improve patient’s functional ability.
A further follow up study to evaluate the effect of correction of hypovitaminosis D, on RA patient’s functional ability is recommended to express more the impact of low vitamin D in such patients.
Conclusion
It appears that low vitamin D is highly prevalent in female patients with rheumatoid arthritis and that vitamin D insufficiency and deficiency may be linked to disease impact on functional ability and disability in female patients with rheumatoid arthritis.
Acknowledgements
We would like to thank all participants who collaborated in the study, the health authorities, and everyone who helped us to accomplish this work.
References
- Lee DM, Weinblatt ME (2001) Rheumatoid arthritis. Lancet. 358 (9285): 903-911.
- Richard D Brasington (2015) Clinical features of rheumatoid arthritis. Rheumatology. 6th (Edn), 85: 704-711.
- Harre U, Georgess D, Bang H, Bozec A, Axmann R, et al., (2012) Induction of osteoclastogenesis and bone loss by human autoantibodies against citrullinated vimentin. J Clin Invest. 122(5): 1791–1802.
- Jimenez-Boj E, Nobauer-Huhmann I, Hanslik-Schnabel B, Dorotka R, Schett G, et al., (2007) Bone erosions and bone marrow edema as defined by magnetic resonance imaging reflect true bone marrow inflammation inrheumatoid arthritis. Arthritis Rheum. 56: 1118–1124.
- Schett G, Firestein GS (2010) Mr Outside and Mr Inside: Classic and alternative views on the pathogenesis of rheumatoid arthritis. Ann Rheum Dis. 69(5): 787–789.
- McInnes I, Schett G (2011) The pathogenesis of rheumatoid arthritis. N Engl J Med. 365(23): 2205–2219.
- Choy E (2012) Understanding the dynamics: pathways involved in the pathogenesis of rheumatoid arthritis. Rheumatology (Oxford). 51: v3–11.
- Klarlund M, Ostergaard M, Jensen KE, Madsen JL, Skodt H, et al., (2000) Magnetic resonance imaging, radiography, and scintigraphy of the finger joints: one year follow up of patients with early arthritis. The TIRA Group. Ann Rheum Dis. 59(7): 521–528.
- Schett G, Gravallese E (2012) Bone erosion in rheumatoid arthritis: mechanisms, diagnosis and treatment. Nat Rev Rheumatol. 8(11): 656–664.
- Escalante A, Del Rincon I (1999) How much disability in rheumatoid arthritis is explained by rheumatoid arthritis? Arthritis Rheum. 42(8): 1712e- 1721.
- Escalante A, Haas RW, Del Rincon I (2005) A model of impairment and functional limitation in rheumatoid arthritis. BMC Musculoskelet Disord. 6: 16.
- Katz PP, Morris A, Yelin EH (2006) Prevalence and predictors of disability in valued life activities among individuals with rheumatoid arthritis. Ann Rheum Dis. 65(6): 763-769.
- Lillegraven S, Kvien TK (2007) Measuring disability and quality of life in established rheumatoid arthritis. Best Pract Res Clin Rheumatol. 21(5): 827–840.
- Bombardier C, Barbieri M, Parthan A, Zack DJ, Walker V, et al., (2012) The relationship between joint damage and functional disability in rheumatoid arthritis: a systematic review. Ann Rheum Dis. 71(6): 836–844.
- Young A, Dixey J, Kulinskaya E, Cox N, Davies P, et al., (2002) Which patients stop working because of rheumatoid arthritis? Results of five years ׳ follow up in 732 patients from the Early RA Study (ERAS). Ann Rheum Dis. 61(4): 335–340.
- Young A, Dixey J, Cox N, Davies P, Devlin J, et al., (2000) How does functional disability in early rheumatoid arthritis (RA) affect patients and their lives? Results of 5 years of follow-up in 732 patients from the Early RA Study (ERAS). Rheumatology (Oxford). 39(6): 603–611.
- Al-Said Y, Al-Rached H, Al-Qahtani H, Jan M (2009) Severe proximal myopathy with remarkable recovery after vitamin D treatment. Can J Neurol Sci. 36(3): 336–339.
- Girgis C, Clifton-Bligh R, Turner N, Lau S, Gunton J (2014) Effects of vitamin D in skeletal muscle: falls, strength, athletic performance and insulin sensitivity. Clin Endocrinol. 80(2): 169–181.
- Ding C, Cicuttini F, Parameswaran V, Burgess J, Quinn S, et al., (2009) Serum levels of vitamin D, sunlight exposure, and knee cartilage loss in older adults: the Tasmanian older adult cohort study. Arthritis Rheum. 60(5): 1381–1389.
- Glowacki J, Hurwitz S, Thornhill TS, Kelly M, LeBoff MS (2003) Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am. 85(12):2,371–2,377.
- Tauber C, Noff M, Noff D, Pitaru S, Malkin C (1991) Blood levels of vitamin D metabolites in gonarthrosis. Arch Orthop Trauma Surg. 110(2): 109–111.
- Felson DT, Niu J, Clancy M, Sack B, Amin S, et al., (2007) Low levels of vitamin D and worsening of knee osteoarthritis: results of two longitudinal studies. Arthritis Rheum. 56(1): 129–136.
- Bergink AP, Uitterlinden AG, JP Van Leeuwen, Pols HA, Hofman A, et al., (2009) Vitamin D status, bone mineral density, and the development of radiographic osteoarthritis of the knee: the Rotterdam study. J Clin Rheumatol. 15(5): 230–237.
- Chapuy MC, Arlot ME, Duboeuf F, Brun J, Crouzet B, et al., (1992) Vitamin D3 and calcium to prevent hip fractures in the elderly women. N Engl J Med. 327(23): 1637–1642.
- Abourazzak FE, Talbi S, Aradoini N, Berrada K, Keita S, et al., (2015) 25-hydroxy vitamin D and its relationship with clinical and laboratory parameters in patients with rheumatoid arthritis. Clin Rheumatol. 34(2): 353–357.
- Ranganathan P, Khalatbari S, Yalavarthi S, Marder W, Brook R, et al., (2013) Vitamin D deficiency, interleukin 17, and vascular function in rheumatoid arthritis. J Rheumatol. 40(9): 1529–1534.
- Raczkiewicz A, Kisiel B, Kulig M, Tłustochowicz W (2015) Vitamin D status and its association with quality of life, physical activity, and disease activity in rheumatoid arthritis patients. J Clin Rheumatol. 21(3): 126–130.
- Patel R, Collins D, Bullock S, Swaminathan R, Blake GM, et al., (2001) The effect of season and vitamin D supplementation on bone mineral density in healthy women: A double-masked crossover study. Osteoporos Int. 12(4): 319–325.
- Latham NK, Anderson CS, Reid IR (2003) Effects of vitamin D supplementation on strength, physical performance, and falls in older persons: a systematic review. J Am Geriatr Soc. 51(9): 1219–1226.
- Ceglia L (2008) Vitamin D and skeletal muscle tissue and function. Mol Aspects Med. 29(6): 407–414.
- American Geriatrics Society Workgroup on Vitamin D Supplementation for Older Adults (2014) Recommendations abstracted from the American GeriatricsSociety Consensus Statement on vitamin D for prevention of falls and their consequences. J Am Geriatr Soc. 62(1): 147–152.
- Brunner RL, Cochrane B, Jackson RD, Larson J, Lewis C, et al., (2008) Calcium, vitamin D supplementation, and physical function in the Women’s Health Initiative. J Am Diet Assoc. 108(9): 1472–1479.
- Bunout D, Barrera G, Leiva L, Gattas V, de la Maza MP, et al., (2006) Effects of vitamin D supplementation and exercise training on physical performance in Chilean vitamin D deficient elderly subjects. Exp Gerontol. 41(8): 746-752.
- Gupta R, Sharma U, Gupta N, Kalaivani M, Singh U, et al., (2010) Effect of cholecalciferol and calcium supplementation on muscle strength and energy metabolism in vitamin D-deficient Asian Indians: a randomized, controlled trial. Clin Endocrinol (Oxf ). 73(4): 445–451.
- Moreira-Pfrimer LDF, Pedrosa MAC, Teixeira L, Lazaretti-Castro M (2009) Treatment of vitamin D deficiency increases lower limb muscle strength in institutionalized older people independently of regular physical activity: a randomized double-blind controlled trial. Ann Nutr Metab. 54(4): 291–300. https://www.ncbi.nlm.nih.gov/pubmed/19729890
- Beaudart C, Buckinx F, Rabenda V, Gillain S, Cavalier E, et al., (2014) The effects of vitamin D on skeletal muscle strength, muscle mass, and muscle power: a systematic review and meta-analysis of randomized controlled trials. J Clin Endocrinol Metab. 99: 4336–4345.
- Aletaha D, Neogi T, Silman AJ, Felson DT, Cohen MD, et al., (2010) Rheumatoid arthritis classification criteria: an American College of Rheumatology/ European League Against Rheumatism collaborative initiative. Arthritis Rheum. 62(9): 2569–2581.
- Prevoo ML, van 't Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, et al., (1995) Modified disease activity scores that include twenty-eight-joint counts, development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 38(1): 44-48.
- Marc C Hochberg, Rowland W Chang, Isaac Dwosh, Theodore Pincus, Wolfe F, et al., (1992) The american college of rheumatology 1991 revised criteria for the classification of global functional status in rheumatoid arthritis. Arthritis Rheum. 35(5): 498–502.
- Holik mf (2009) Vitamin d status: measurement, interpretation, and, clinical application. Ann epidemiology. 19(2): 73-78.
- Uhlig T, Loge JH, Kristiansen IS, Kvien TK (2007) Quantification of reduced health-related quality of life in patients with rheumatoid arthritis compared to the general population. J Rheumatol. 34(6): 1241–1247.
- Matcham F, Scott IC, Rayner L, Hotopf M, Kingsley GH, et al., (2014) The impact of rheumatoid arthritis on quality-of-life assessed using the SF-36: A systematic review and meta-analysis. Semin Arthritis Rheum. 44(2): 23-130.
- National Institute of Clinical Excellence (NICE) (2009) Rheumatoid arthritis: the management of rheumatoid arthritis in adults 2009.
- Grazio S1, Naglić ĐB, Anić B, Grubišić F, Bobek D, et al., (2015) Vitamin D serum level, disease activity and functional ability in different rheumatic patients. Am J Med Sci. 349(1): 46-49.
- Furuya T1, Hosoi T, Tanaka E, Nakajima A, Taniguchi A, et al., (2013) Prevalence of and factors associated with vitamin D deficiency in 4,793 Japanese patients with rheumatoid arthritis. Clin Rheumatol. 32(7): 1081-7.





