Brown Tumors or Bone Metastases in Context of Parathyroid Carcinoma: A Diagnostic Challenge
Blasco LG*, Cozar-Santiago MD, Ferrer-García JC, Sánchez Juan C
Hospital General Universitario de Valencia, Valencia, Spain.
*Corresponding Author
Lourdes Garcia Blasco,
Hospital General Universitario de Valencia,
Valencia, Spain.
Tel: 0034617685459
E-mail: lourdesgb88@hotmail.com
Received: May 14, 2016; Accepted: August 06, 2016; Published: August 11, 2016
Citation: Blasco LG, Cozar-Santiago MD, Ferrer-García JC, Sánchez Juan C (2016) Brown Tumors Or Bone Metastases In Context Of Parathyroid Carcinoma: A Diagnostic Challenge. Int J Bone Rheumatol Res. 3(5), 46-49.DOI : dx.doi.org/10.19070/2470-4520-160010
Copyright: Blasco LG© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Parathyroid carcinoma is a rare cause of primary hyperparathyroidism. When this malignancy is diagnosed, often there are distant metastases (usually liver and/or bone). Brown tumor is a localized form of osteitis fibrosa cystica; classic manifestation in bone of excess parathyroid hormone and this is a bening pathology. We encountered an unusual case of parathyroid carcinoma with images that mimicked metastatic bone tumors, whose differential diagnosis with brown tumor may be complicated. Positron emission tomography/computed tomography (PET/CT) scan was requested for the evaluation of fluorodeoxyglucosa uptake of these lesions. PET/CT images showed multiple hypermetabolic images that mimicked multiple skeletal metastasis but brown tumors could not be dismissed.
2.Abbreviations
3.Introduction
4.Case Report
5.Conclusion
6.References
Keywords
Hyperparathyroidism; BrownTumor; Parathyroid Carcinoma; Parathyroidectomy, Positron Emission Tomography / Computed Tomography.
Abbreviations
PET/CT: Positron Emission Tomography/Computed Tomography; PHPT: Primary Hyperparathyroidism; PTH: Parathyroid Hormone; US: Ultrasonography; MIBI: Methoxyisobutylisonitrile; CT: Computed Tomography; HDP: Hydroxymethane Diphosphonate; 18F-FDG PET/CT: Fluorine-18 Fluorodeoxyglucosa Positron Emission Tomography / Computed Tomography; SUV: Standardized Uptake Value.
Introduction
Primary hyperparathyroidism (PHPT) is usually caused by a parathyroid adenoma, occasionally by primary parathyroid hyperplasia, and rarely by a parathyroid carcinoma. Parathyroid malignancy is a rare cause of hyperparathyroidism, the incidence is around 1%. Whereas benign hyperparathyroidism is more common in women (3:1), the incidence of parathyroid cancer is equal between the two genders. The main clinical manifestations of parathyroid carcinoma are neck mass, bone and kidney disease, marked hypercalcaemia, and very high serum parathyroid hormone (PTH) concentrations. Up to one-third of subjects have lymph node metastases at initial presentation, and one-third have distant metastases, usually in liver and bone. Less than 10 percent of parathyroid carcinomas are hormonally non-functional, and such tumors usually are presented at a more advanced stage.
The classic manifestation of PHPT bone disease is osteitis fibrosa cystica, which is characterized clinically by bone pain and radiographically by subperiosteal bone resorption. Brown tumors result from excess of osteoclast activity and present of collections of osteoclasts intermixed with fibrous tissue and poorly mineralized woven bone. The brown coloration is due to hemosiderin deposition.
We report a case of a male with a parathyroid carcinoma and bone lesions that pose differential diagnosis between metastases and brown tumor.
Case Report
A 39 years old man was evaluated because of left gluteal pain. He had been in good health until five months before presentation, when he began to experience pain without trauma. Weakness, anorexia, weight loss and urinary frequency were also noted. On physical examination, a firm mass, 2 cm in diameter, was palpated in the left lobe of the thyroid gland. The X-ray study showed enhanced reabsortion in left ischiopubic ramus. Calcium levels were 13.9 mg/dL.
The patient was admitted in Endocrinology department to be studied of hypercalcaemia. Initial laboratory data are shown in Table 1. Neck ultrasonography (US) disclosed a 41 mm solid nodule that was heterogeneous in the low left lobe of the thyroid gland. Color Doppler US demonstrated plentiful pulsating blood flow. The X-ray study demonstrated a “salt and pepper” (Figure 1) appearance in the cranium and generalized bone demineralization of bone. Abdominal X-ray showed a stone in left kidney. Cervical 99mTc-MIBI (methoxyisobutylisonitrile) scintigraphy performed 2 hours after injection revealed a focus of high uptake in the left lower portion of the cervical region concordant with US lesion. During surgery left lower parathyroid gland was observed enlarged; it invadied thyroid and esophagus and they were removed successfully. Inmunohistogical study revealed parathyroid carcinoma with essophagus invasion. Soon after the operation, his serum calcium levels were restored to the normal range. After that, because of “hungry bone” syndrome, his serum calcium levels decreased to 7.7 mg/dL.
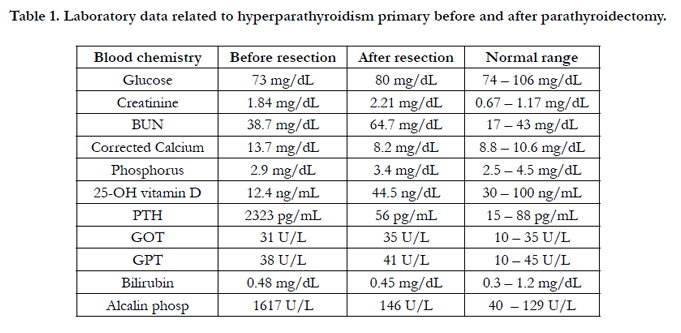

Table 1. Laboratory data related to hyperparathyroidism primary before and after parathyroidectomy.
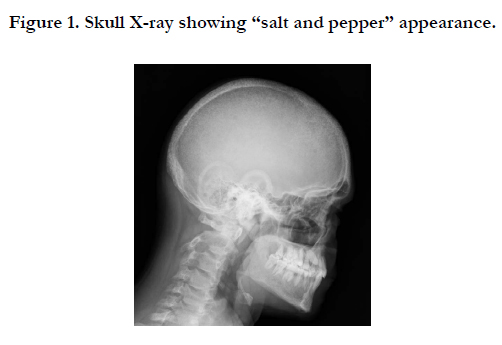

Figure 1. Skull X-ray showing “salt and pepper” appearance.
Computed tomography (CT) images showed multiple stones in kidneys and lytic and osteoblastic lesions in the axial skeleton and pelvis. These bone lesions mimicked multiple skeletal metastatic lesions but brown tumors could not be dismissed. Whole body bone imaging with 99mTc-HDP (hydroxymethane diphosphonate) (Figure 2), revealed diffusely increased uptake in the calvarium, in cortex of the long bones and also a focal increased uptake in the left pubis and other in the middle right ulna. The orthopedic surgeon performed a bone biopsy that wasn’t diagnostic. Fluorine- 18 fluorodeoxyglucosa positron emission tomography/computed tomography (18F-FDG PET/CT) imaging was requested for the evaluation of FDG uptake of these lesions, three months after surgery. 18F-FDG PET/CT whole body imaging was performed after intrevenously injection of 6.5 mCi 18F-FDG. PET/ CT images showed increased FDG uptake in left iliac bone with a maximum standardized uptake value (SUV) of 2.4 without SUV modification in the late acquisition. A year after parathyroidectomy, a new PET/CT was performed which showed structural lesion without uptake in this region (Figure 3).
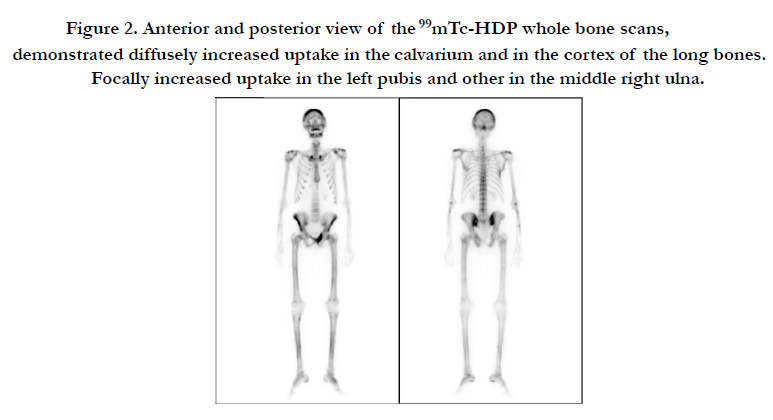
Figure 2. Anterior and posterior view of the 99mTc-HDP whole bone scans, demonstrated diffusely increased uptake in the calvarium and in the cortex of the long bones. Focally increased uptake in the left pubis and other in the middle right ulna.
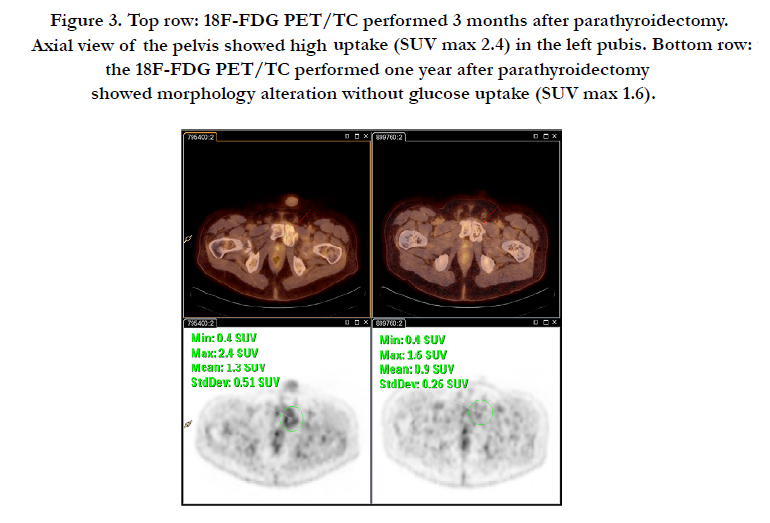
Figure 3. Top row: 18F-FDG PET/TC performed 3 months after parathyroidectomy. Axial view of the pelvis showed high uptake (SUV max 2.4) in the left pubis. Bottom row: the 18F-FDG PET/TC performed one year after parathyroidectomy showed morphology alteration without glucose uptake (SUV max 1.6).
Parathyroid carcinoma is an unusual cause of PTH-dependent hypercalcaemia, counting for less than 1% of all cases of hyperparathyroidism [1]. The diagnosis of parathyroid carcinoma is often made during surgery or histopatholgy examination. The tumor often invades surrounding structures, spreads to regional lymph nodes and disseminates haematogenously to lungs, liver and bones. The prognosis depends on the completeness of tumor resection. Mortality rates for parathyroid carcinomas, particularly for those patients with recurrence within the first 2 years postoperatively are high and are reported to be between 46% and 65%.
Brown tumors are not true tumors but they are the final stage of hyperparathyroidism. Clinically, brown tumors are often manifested as slowly growing, painful masses producing bone pain and arthralgia which are the most common symptoms. Brown tumor is caused by increased circulating levels of parathyroid hormone, which results in increased osteoclastic bone resorption primarily in the cortical bone. Brown tumors can be detected in different imaging techniques.
Since 1994, when Joyce et al. first reported that multiple brown tumors in primary hyperparathyroidism due to adenoma can mimic metastatic disease on MIBI scan [9], there have been many similar reports [10, 11].
Discrepant uptake among radiotracers of 99Tc-MIBI and 99mTc- HDP in brown tumors has been reported in the literature [7]. FDG PET/CT imaging has been commonly used to distinguish malign lesions from benign lesions. High FDG uptake may be seen in benign conditions such as inflammation and infections [3]. High FDG uptake mechanism has been suggested to be the presence of giant cells in brown tumors which can be visualized with PET/CT. Another mechanism is that intracellular glucose metabolism of the macrophages may play a role for the elevated FDG uptake [4, 8].
In our case, neither bone scan, 18F-FDG PET/CT nor bone biopsy allowed a definitive diagnosis of bone metastases or brown tumors. However, withdrawing stimulus PTH, brown tumors often regress, which is detected in PET / CT in earlier stage than other conventional imaging techniques (metabolic changes occur before morphological ones). In the case of the coexistence of brown tumors with bone metastases, when PTH stimulus is removed, brown tumors regress but metastatic lesions would continue uptaking 18F-FDG [12].
Brown tumor treatment consists of correcting the cause of hyperparathyroidism. Most authors believe that the bone lesions regress after some time after parathyroidectomy. The length of time for bone regeneration varies from several months in young patients to several years in elder patients. In our case, bone lesion had regressed a year after parathyroidectomy. Any lesions do not regress but extend beyond the normal anatomy and calcify [5, 6].
Conclusion
Differential diagnosis between brown tumors and bone metastases can be a challenge in the parathyroid carcinoma context. After correction of hyperparathyroidism, FDG PET/CT imaging can be useful to see the response to treatment and osteoblastic changes in brown tumors and this imaging technique allows definitive diagnosis between bone metastases and brown tumors.
References
- Wynne AG, Van Heerden JON, Carney JA, Fitzpatrick LA (1992) Parathyroid carcinoma: clinical and pathologic features in 43 patients. Medicine 71(4): 197-205.
- Treglia G, Dambra DP, Bruno I, Mulè, A, Giordano A (2008) Costal brown tumor detected by dual-phase parathyroid imaging and SPECT-CT in primary hyperparathyroidism. Clinical nuclear medicine, 33(3): 193-195.
- Aoki J, Watanabe H, Shinozaki T, Takagishi K, Ishijima H, et al., (2001) FDG PET of Primary Benign and Malignant Bone Tumors: Standardized Uptake Value in 52 Lesions 1. Radiology. 219(3): 774-777.
- Gamelli RL, Liu H, He LK, Hofmann CA (1996) Augmentations of glucose uptake and glucose transporter-1 in macrophages following thermal injury and sepsis in mice. Journal of leukocyte biology, 59(5): 639-647.
- Knezevic G, Uglesic V, Kobler P, Svajhler T, Bagatin M (1991) Primary hyperparathyroidism: evaluation of different treatments of jaw lesions based on case reports. Brit I Oral Max Surg. 29(3): 185-188.
- Daniels JSM (2004) Primary hyperparathyroidism presenting as a palatal brown tumor. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 98(4): 409-413.
- Gonca Kara Gedik GK, Ata O, Karabagli P, Sari O (2013) Differential diagnosis between secondary and tertiary hyperparathyroidism in a case of a giant-cell and brown tumor containing mass. Findings by (99m) Tc-MDP,(18) F-FDG PET/CT and (99m) Tc-MIBI scans. Hellenic journal of nuclear medicine, 17(3): 214-217.
- Sager S, Aliyev A, Halac M, Oztürk T (2012) Positron emission tomography/ computed tomography imaging of brown tumors mimicking multiple skeletal metastases in patient with primary hyperparathyroidism. Indian journal of endocrinology and metabolism. 16(5): 850.
- Joyce JM, Idea RJ, Grossman SJ, Liss RG, Lyons JB (1994) Multiple brown tumors in unsuspected primary hyperparathyroidism mimicking metastatic disease on radiograph and bone scan. Clinical nuclear medicine. 19(7): 630-635.
- Pai M, Park CH, Kim BS, Chung YS, Park HB (1997) Multiple brown tumors in parathyroid carcinoma mimicking metastatic bone disease. Clinical nuclear medicine, 22(10): 691-694.
- Rubin, MR, LiVolsi VA, Bandeira F, Caldas G, Bilezikian JP (2001) Tc99msestamibi uptake in osteitis fibrosa cystica simulating metastatic bone disease. The Journal of Clinical Endocrinology & Metabolism, 86(11): 5138-5141.
- Santiago Chinchilla A, Ramos Font C, Muros de Fuentes MA, Navarro- Pelayo Láinez M, Palacios Gerona H, et al., (2011) False negative of the scintigraphy with 99mTc-sestamibi in parathyroid carcinoma with associated Brown tumors. Contributions of the 18F-FDG PET/CT. Rev. Esp Med Nucl 30(3): 174-9.





