Subungual Nodule of the Great Toe in Female Child
N. Amraoui1*, S. Gallouj1, M. Meziane1, H.Abid2, A.El mrini2, K.Moumna3, T.Harmouch3, F.Mernissi1
1 Department of Dermatology, Hassan II University Hospital, Morocco.
2 Department of Orthopedy traumatology B4, Hassan II University Hospital, Morocco.
3 Department of Pathology, Hassan II University Hospital, Morocco.
*Corresponding Author
Amraoui nissrine,
Department of Dermatology Venereology,
Hassan II University Hospital Fez, Morocco.
Tel: 00212666132727
E-mail: nissrineamraoui@hotmail.com
Article Type: Case Report
Received: April 20, 2015; Accepted: June 10, 2015; Published: June 12, 2015
Citation: N. Amraoui et al., (2015) Subungual Nodule of the Great Toe in Female Child. Int J Bone Rheumatol Res, 2(3), 18-20. doi: dx.doi.org/10.19070/2470-4520-150004
Copyright: N. Amraoui© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Subungual exostoses are bony projections which arise from the dorsal surface of the distal phalanx, most commonly of the hallux, often disturbing the nail plate and causing pain. We report case of subungual exostosis in a female child of 10 years who presented since one year a fixed firm nodule of the great toe. Clinically, radiologic and histological finding were compatible with subungual exostosis. The treatment is surgical. Early diagnosis avoids nail dystrophy.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.References
Key Words
Subungual Exostosis; Nodule; Great Toe; Surgery.
Introduction
Subungual exostoses are bony projections which arise from the dorsal surface of the distal phalanx, most commonly of the hallux [1], often disturbing the nail plate and causing pain. We report case of subungual exostosis in a female child.
Case Report
A 10-year-old female child presented since one year history of a slowly growing mass on the tip of the left great toe. She denied any significant trauma to the great toe. The mass was painful when pressed. Skin examination found a 1cm fixed nodule extending from the distal end of the nail. There was poor adherence between the distal nail plate and underlying nail matrix associated to ungueal dystrophy. The mass was firm and covered with scaly skin (Figure 1). X-ray showed a bony growth protruding from the distal phalanx of the great toe (Figure 2). For the surgical management, after performing a digital block, we removed the nail plate (Figure 3). A strong nail clipper was used to divide the base of the mass at its juncture with the distal phalanx, followed by curettage of the distal phalanx with a bone curette. The nail matrix was repaired with absorbable suture and the nail plate was replaced. The control radiograph showed the disappearance of the mass (Figure 4). Pathologic analysis of the lesion revealed mature trabecular bone with a proliferating fibrocartilaginous consistent with exostosis. There was no evidence of recurrence with a decline of 2 years.
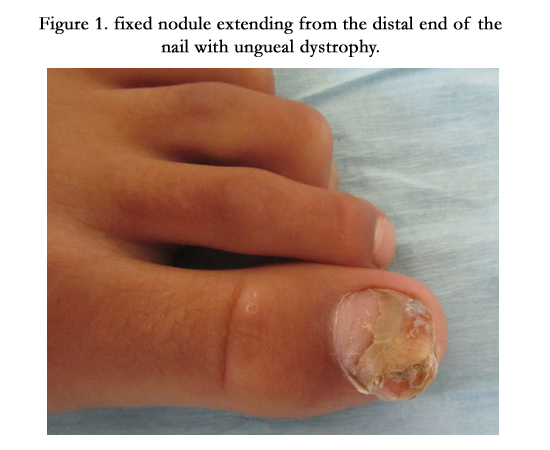

Figure 1. fixed nodule extending from the distal end of the nail with ungueal dystrophy.
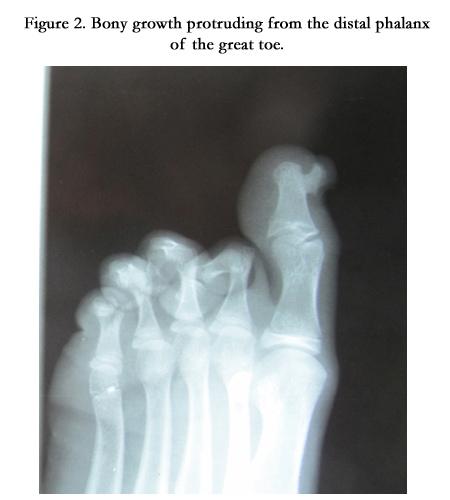

Figure 2. Bony growth protruding from the distal phalanx of the great toe.
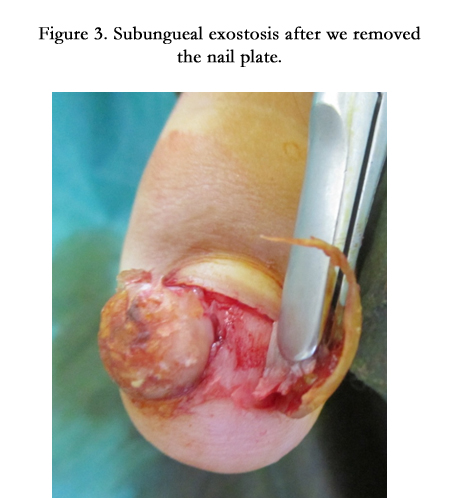

Figure 3. Subungueal exostosis after we removed the nail plate.

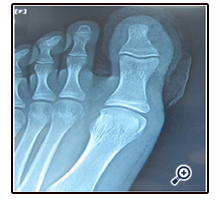
Figure 4. disappearance of the mass after surgery.
Discussion
Subungual exostosis is an uncommon, slow growing, benign osteocartilaginous tumour arising from the distal phalanx of a digit, beneath or adjacent to the nail bed. Dupuytren first described the condition in 1817 [2, 3] clinically it appears as painful red-pink expanding nodule under the great toenail. The majority of the lesions occur in the second or third decade of life which is the case of our patient [4]. Fikri reported 28 observations in 14 years [5]. Landon reported 44 observations in 65 years [6]. Subungual exostosis more commonly affects women than men in a ratio of 2:1 [7]. Differential diagnoses include subungual verruca, squamous cell carcinoma, onychocryptosis, inclusion cysts, glomus tumor, malignant melanoma [8], Ingrown toenail, Pyogenic granuloma, and Osteochondroma.
Radiologic imaging of Subungual exostosis reveals an osteocartilaginous exophytic mass extending from the distal tuft of the phalanx. Histology showed mature trabecular bone with a proliferating fibrocartilaginous [4].
Various surgical techniques are performed, depending on the extent of nail bed involvement. A fish mouth incision is made where the lesion does not destroy the nail bed. This type of incision raises the nail to excise the tumor, leaving the nail bed intact. Where the lesion is large and the nail bed is destroyed, the nail is removed and the tumor approached directly from above. In this case, the nail bed is preserved as much as possible [9]. The most common complications associated with the excision of a subungual exostosis are recurrence, infection, nail plate growth disturbances, and subungual hematoma.
The etiology of subungual exostosis is unknown. The presence of a subungual exostosis is usually interpreted as a reactive process rather than as a neoplasic one. It has been described as an acquired deformity in which trauma and microtrauma seem to be the most important etiologic factors [10]. Others authors have hypothesized their growth is related to chronic infection. Starnes reported a genetic correlation in a small number of patients [11]. In an analysis of the histology of subungual exostosis, Ippolito reported that growth could occur via two different mechanisms: enchondral ossification, or more commonly, intramembranous/ mixed ossification [12].
Conclusion
The diagnosis of subungual exostosis is easy, it may be suspected from the clinical presentation and confirmed with radiographic examination. Subungual exostosis should be considered in the differential diagnosis of any digital mass.
References
- Rapini RP, Bolognia JL, Jorizzo JL (2007) Dermatology. (2nd edtn) Set. St. Louis: Mosby.
- Dave S, Carounanidy U, Thappa DM, Jayanthi S (2004) Subungual exostosis of the thumb. Dermatol Online J 10(1): 15.
- Singh R, Jain M, Goel R, Siwach R, Kalra R et.al., (2011) Subungual exostosis of the great toe: a case report and tumor overview. Foot Ankle Spec 4(6): 376–378.
- Letts M, Davidson D, Nizalik E (1998) Subungual exostosis: diagnosis and treatment in children. J Trauma 44(2): 346-349.
- Fikry T, Dkhissi M, Harfaoui A, Adil A, Haddoun A et al., (1998) Subungual exostoses. A retrospective study of a series of 28 cases. Acta Orthop Belg 64(1): 35-40.
- Landon G, Johnson KÀ, Dahlin D (1979) Subungual exostosis. J Bone Joint Surg 61: 256-259.
- Davis DA, Cohen PR (1996) Subungual exostosis: case report and review of the literature Pediatr Dermatol 13(3): 212-218.
- Carroll RE, Chance JT, Inan Y (1992) Subungual exostosis in the hand. J Hand Surg Br 17: 569–574.
- Lokiec F, Ezra E, Krasin E, Keret D,Wientrob S (2001) A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 21(1):76-79.
- GrisafI PJ, Lombardi CM, Sciarrino AL, Rainer GF, Buffone WF (1989) Three select subungual pathologies: subungual exostosis, subungual osteochondroma and subungual hematoma. Clin Podiatr Med Surg 6(2): 355- 364.
- Starnes A, Kara Crosby DO, Rowe DJ, Jeremy S (2012) Subungual exostosis: A simple surgical technique. Dermatol Surg 38(2):258–260.
- Ippolito E, Falez F, Tudisco C, Balus L, Fazio M et al., (1987) Subungual exostosis. Histological and clinical considerations on 30 cases. Ital J Orthop Traumatol 13(1): 81–87.





