Comparison of Reliability and Validity of the Breast Cancer depression anxiety stress scales (DASS- 21) with the Beck Depression Inventory-(BDI-II) and Hospital Anxiety and Depression Scale (HADS)
Bener A1,2*, Alsulaiman R3,4, Doodson L3, El Ayoubi HR4,5
1 Department of Biostatistics & Medical Informatics, Cerrahpaşa Faculty of Medicine, Istanbul University, Istanbul, Turkey.
2 Department of Evidence for Population Health Unit, School of Epidemiology and Health Sciences, University of Manchester, Manchester, UK.
3 Regent's University London, Inner Circle, Regent's Park, London NW1 4NS, UK.
4 Department of Oncology & Hematology, Al Amal Hospital, Hamad Medical Corporation, Qatar.
5 Department clinical hematologist and a stem cell transplantation, Hospital Saint Louis, France.
*Corresponding Author
Abdulbari Bener,
Advisor to WHO, Professor of Public Health,
Department of Biostatistics & Medical Informatics, Cerrahpaşa Faculty of Medicine, Istanbul University, 34098 Cerrahpasa-Istanbul,
Turkey.
Tel: +90-212-414 3041/+90-535 663 9090
Fax: + 90-212-632 0033
E-mail: abdulbari.bener@istanbul.edu.tr
abener99@yahoo.com
Received: July 26, 2016; Accepted: October 21, 2016; Published: October 24, 2016
Citation: Bener A, Alsulaiman R, Doodson L, El Ayoubi HR (2016) Comparison of Reliability and Validity of the Breast Cancer depression anxiety stress scales (DASS-21) with the Beck Depression Inventory-(BDI-II) and Hospital Anxiety and Depression Scale (HADS). Int J Behav Res Psychol. 4(4), 196-202. doi: dx.doi.org/10.19070/2332-3000-1600035
Copyright: Bener A© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: No study has been conducted to determine the reliability and validity of the Depression, Anxiety and Stress Scale (DASS-21), Hospital Anxiety and Depression [HADS] and Beck Depression Inventory (BDI-II) among the Arab Breast Cancer population.
Aim: The aim of this study was to compare the reliability and validity of the Depression, Anxiety, and Stress scale (DASS-21), the Beck Depression Inventory-(BDI-II) and Hospital Anxiety and Depression Scale (HADS) among Breast Cancer women in Qatar.
Design: This is an observational cohort hospital based study.
Subjects: A list of 1,042 eligible breast cancer patients was prepared, from the disease registry from January 2010 to December 2014 who could be contacted. From the available 1,042 list, 730 breast cancer patients information were available (70.0%) and expressed their consent to participate in the study.
Methods: Breast cancer women were screened for depression using DSM-IV criteria, followed by data collection based on 21 items Depression Anxiety Stress Scale (DASS-21), Hospital Anxiety and Depression Scale (HADS) and Beck Depression Inventory (BDI-II) through interviews by trained nurses. Analyses included comparisons between the classifications of women according to the HADS, BDI-II and DASS-21 with classification of breast cancer depression based on DSM IV (Gold standard). Sensitivity, specificity, area under the curve and kappa coefficients was calculated for each scale.
Results: The prevalence of postpartum depression was 20% based on DSM-IV criteria while on the other hand the prevalence was 23% based on DASS-21, 21.8% based on BDI-II and 19.7% based on HADS validated tools. Sensitivity was highest for BDI-II (85%) followed by DASS-21 and HADS (78%) based on standard cut off points of ≥17, ≥10 and ≥13 respectively. On the other hand, specificity was highest for DASS-21 (89%) followed by BDI-II (81%) and HADS (80%). The area under the curve (AUC) was 0.86 (95% CI 0.83-0.89) for DASS-21, 0.84 (95% CI 0.80-0.88) for BDI-II and 0.83 (95% CI 0.80- 0.86) for HADS scales. There was highest agreement between DASS-21 and HADS (Kappa =0.80 p value <0.001), followed by DASS-21 and BDI-II (Kappa 0.75, p value <0.001) and BDI-II and EPDS (Kappa 0.60, p <0.001).
Conclusions: DASS-21, BDI-II and HADS have excellent sensitivity, and specificity to quickly screen for breast cancer women. Agreement is highest among DASS-21 and HADS. Overall, DASS-21 performed better as compared to the other tools based on sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV). The Arab version of the DASS-21 exhibited satisfactory psychometric properties and its use for research and health care practice is warranted. Results indicate and support the cross-cultural validity of the DASS-21 in Arab countries.
2.Introduction
3.Subjects and Methods
3.1.Hospital Anxiety and Depression Scale (HADS)
4.Results
5.Discussion
6.Conclusion
7.Acknowledgments
8.References
Keywords
Validity; ROC; Tools; Breast Cancer; Depression; Reliability.
Introduction
Breast cancer depression, anxiety and stress are one of the important public health problems affecting women and family. Breast cancer, one of the most important health problems of women in developed countries, accounts for almost 30% of all cancer types among women [1]. As for Qatar, breast cancer has been the most common cancer type that affects women and in the majority of developed countries (WHO, 2014). Breast cancer was the most common cancer worldwide in women accounting for more than 25% of the total number of new cases diagnosed in 2012 [2, 3]. Cancer is one of the most common causes of death worldwide, accounting for 7.6 million deaths in 2008 [2].
The role of psychological variables, particularly those of anxiety and depression in disease progression and clinical outcome has received attention from the research community. A diagnosis of breast cancer is often accompanied by a significant and profound experience of psychological distress, the most commonly presenting symptoms being those of anxiety and depression [3]. It is worth noting that the prevalence rates of clinically relevant levels of anxiety and depression in cancer patients have been estimated to be up to 45% [4-6]. It has been observed that psychological symptoms often decrease over time, further it has also been observed in the clinical presentation of breast cancer that up to 30% of these patients will continue to experience clinically relevant levels of anxiety and depression at follow-up [7]. Rodgers et al., [8] reported in a study of women with advanced breast cancer that anxiety and depression, as assessed by self-report measure, were significant predictors of the patients' response to chemotherapy in terms of clinical and pathological outcomes and patient who may be anxious and depressed following diagnosis and treatment. The Hospital Anxiety and Depression Scale (HADS) [9] is a widely used self-report instrument designed as a brief assessment tool of the distinct dimensions of anxiety and depression in non-psychiatric populations [10, 11]. The HADS has also been used widely in the clinical oncology setting as a screening and research tool [8, 13-16].
To date, the most commonly used screening tools for breast cancer depression are the Hospital Anxiety and Depression Scale (HADS) [9-15] followed by the Beck Depression Inventory (BDIII) [16-19]. One of the main weaknesses of these screening instruments is that they are not able to screen for the existence of potential anxiety or stress which occurs during the breast cancer treatment period. A number of studies have suggested that the HADS reliably measures anxiety and depression in cancer patients [8, 14, 16] and should be adopted as a routine clinical tool for screening for psychological distress [5, 8, 10]. However, a number of other investigations in this area have suggested that the HADS may not be a suitable instrument to assess patients with cancer [13, 20] or are we using appropriate self-report questionnaires for detecting anxiety and depression in women with early breast cancer [13, 21]. They argue that it is not adequate to subsume anxiety in the breast cancer within diagnoses of depression and stress. Therefore, a new instrument which differentiates between postpartum depression, anxiety and stress (DASS-21) has recently been recommended to be used in clinical groups and a community sample of populations [25-27].
So far, no breast cancer study has been utilized the DASS-21 instrument, although, the DASS-21 has been translated into Arabic and tested for reliability and validity in an Arab population [24-26]. The aim of the current study was to compare the reliability and validity of the Depression, Anxiety, and Stress scale (DASS- 21), the Beck Depression Inventory-(BDI-II) and Hospital Anxiety and Depression Scale (HADS) among Arab breast cancer women in Qatar.
Subjects and Methods
This is an observational cohort hospital study based on the national Cancer Disease Registry of the Al-Amal hospital. This national Cancer Disease Registry registers all the reported cancer cases in Qatar. They record complete information of the patients diagnosed with any type of cancer in Qatar. Al Amal hospital succeeded in offering a multidisciplinary approach to cancer care. The main tertiary care center, Hamad General Hospital, has main Central Laboratory for histopathology and cytological diagnosis of cancer. The computer system in the pathology department is organized such that on reporting any cancer cases, a copy of the histopathology report is sent to the cancer registry. All the positive cases of cancer reports from the Hamad General Hospital Central lab are forwarded to the cancer disease registry, thus ensuring that any cancer patient in Qatar would be accurately documented. All cancer cases were coded using International Classification of diseases 10 (ICD 10). According to ICD-10, malignant neoplasms of breast were coded under C50.
The study was approved by the IRB of Research Ethics Committee of Hamad Medical Corporation (HMC-MRC), in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
A list of 1,042 eligible breast cancer patients was prepared, from the disease registry from January 2009 to December 2014 who could be contacted. From the available 1,042 list, 730 breast cancer patients information were available (70.0%) or expressed their consent to participate in the study. Recruited nurses were Arab nationals who speak and write English and Arabic languages well. The nurses were aware of the Arabic culture and thus were able to engage and gain the trust of the study participants if they were not open to discuss their problems and answer the questions. The questionnaire had four parts. The first part included the socio-demographic details of the patients, the second part the medical and family history of the patients, the third part was included the 3 diagnostic screening instruments (DASS-21, HADS, and BDI-II).
The HADS is a 14-item scale designed to detect anxiety and depression, independent of somatic symptoms. The reliability and validity of the Arabic version of the HADS questionnaire has been previously tested. It has two, 7-item subscales measuring depression and anxiety. Each item is assessed on a 4-point response scale (from 0, representing absence of symptoms, to 3, representing maximum symptomatology) with possible scores for each subscale ranging from 0 to 21. Higher scores indicate higher levels of anxiety and depression. The Arabic version of HADS has been develop and validated by previous study Bener et al.,[22]. For the screening sample of 730 breast cancer patients reported here, Cronbach’s alpha coefficient was 0.80.
The Beck Depression Inventory-II (BDI-II) was widely used selfreport to measure the severity of depression [18, 23, 28]. The BDI-II consists of a 21- item self-report inventory where each item describes common symptoms of depression. The respondent was asked to rate each symptom over the preceding week on a four point scale (0-3). Scores of 0-7 reflect minimal depression, 8-15 mild depression; a score of 16-25 was regarded as moderate depression and a score of 26-63 indicated severe depression [18, 23, 28]. The upper interval limit may be adjusted depending on the purpose for the use. To minimize the rate of false negative results the upper interval limit may decrease and to minimize the rate of false positive results the upper limit may be increased. The results support the use of the BDI-II in a community sample. In this study we used a cut-off level of ≥10 to define symptoms of depression. Cronbach’s Alpha was 0.84 for BDI-II scales.
The Depression Anxiety Stress Scales (DASS) [23] is a self-report instrument designed to measure the negative emotional states of depression, anxiety and stress [23-27]. The DASS depression scale has been shown to correlate strongly with the BDI-II, (r = .76), and the DASS anxiety scale with the BDI-II (r = .83) [22, 26]. The 21 item form of the DASS was incorporated into the questionnaire to measure severity of symptoms common to anxiety and depression and the prevalence of co-morbid depression and anxiety. Women were asked to use a 4-point severity/frequency scale to rate the extent to which they had experienced each symptom over the past week from ‘never’ to ‘most of the time’.
Scores for the DASS-21 sub-scales of depression and anxiety were derived by totaling the scores for each sub-scale and multiplying by two to ensure consistent interpretation with the longer 42 item version [23, 28]. We classified women according to the recommended scoring system using cut-off values to classify participants into the following categories: normal (0-9 for depression and 0-7 for anxiety), mild (10-13 for depression and 8-9 for anxiety), moderate (14-20 for depression and 10-14 for anxiety), severe (21-27 for depression and 15-19 for anxiety), and extremely severe (≥28 for depression and ≥20 for anxiety). We have referred to women within the ‘normal’ range on the DASS-21 for depressive or anxiety symptoms as non-depressed or non-anxious respectively. Women, who scored in the ‘mild’ to ‘extremely severe’ ranges, were referred to as depressed or anxious. Analysis is based on this dichotomy (i.e. ‘normal range’ versus ‘mild to extremely severe’ symptoms). Internal consistency in the present study was explored for each scale of the DASS-21, and Cronbach’s alpha coefficients were adequate: Depression (.84), Anxiety (.80) and Stress (.87).
Data were analyzed using SPSS Version 21. Student-t test was used to ascertain the significance of differences between mean values of two continuous variables and confirmed by non-parametric Mann-Whitney test. The Chi-square and the Fisher’s exact test (two-tailed) analysis were performed to test for differences in proportions of categorical variables between two or more groups. Relationships between the DASS-21, BDI-II and HADS results were measured using Pearson correlations. Internal reliability was assessed with Cronbach’s alpha. To evaluate the comparative utility of the assessment instruments, sensitivities, specificities, positive predictive values (PPV), and negative predictive values (NPV) were calculated. Receiver operating characteristic (ROC) curves were employed to derive areas under the curves (AUC). AUC’s greater than >0.5 are interpreted to perform at better than chance levels, with values of >0.8 recommended to conclude a given test is accurate. Chi-square analyses were subsequently used to compare the AUC’s of the DASS-21, BDI-II and HADS with summary scoring to assess for the differences. Statistical contrasts between the DASS-21, BDI-II and HADS diagnostic algorithm were performed and using the Fisher Exact test.
Results
A total of 1,042 breast cancer patients was approached and investigated based on the cancer disease registry 730 breast cancer patients who could be accessed and information were available (70.0%) for study. In the study sample, the prevalence of depression was 20% based on DSM-IV criteria while on the other hand the prevalence was 24.4% based on DASS-21, 25.1 % based on BDI-II and 16.5% based on HADS validated questionnaires. Table 1 shows selected demographic, maternal and obstetric characteristics of the sample according to depressed and non-depressed using the DASS-21 instrument.
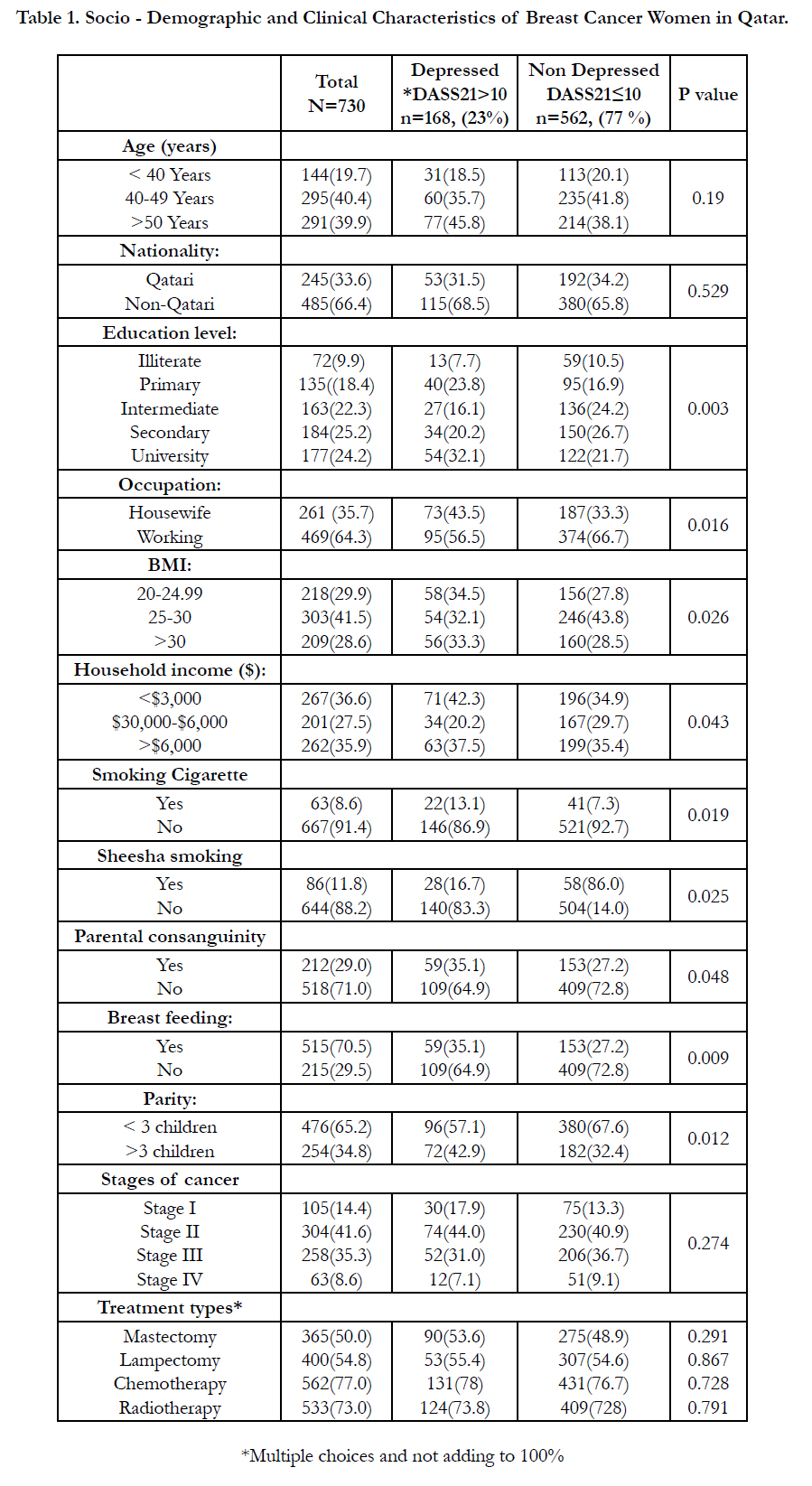

Table 1. Socio - Demographic and Clinical Characteristics of Breast Cancer Women in Qatar.
Table 2 shows mean scores with standard deviation for breast cancer women with and without depression based on DASS- 21, BDI-II, and HADS scales. The scores were higher on all the three scales for the depressed group as compared to nondepressed group with a means and standard deviations for DASS- 21 (24.4±5.7) , for BDI-II (25.1±7.6) and for HADS (16.5.4±7.1) (p<0.001.
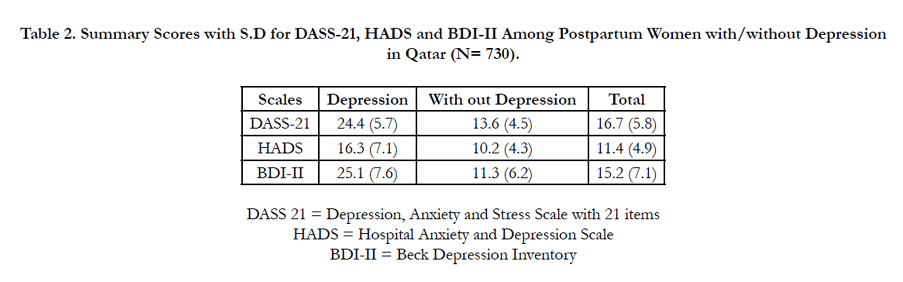
Table 2. Summary Scores with S.D for DASS-21, HADS and BDI-II Among Postpartum Women with/without Depression in Qatar (N= 730).
Table 3 shows comparative performance of DASS-21, HADS, and BDI-II using commonly used cutoff points. Sensitivity was highest for BDI-II (85%) followed by DASS-21 (0.83) and HADS (78%) based on standard cut off points of ≥17, ≥10 and ≥13 respectively. On the other hand, specificity was highest for DASS-21 (89%) followed by BDI-II (81%) and HADS (80%). Positive predictive and negative predictive values were highest for DASS-21 (0.66 and 0.96 respectively) as compared to the other two scales.
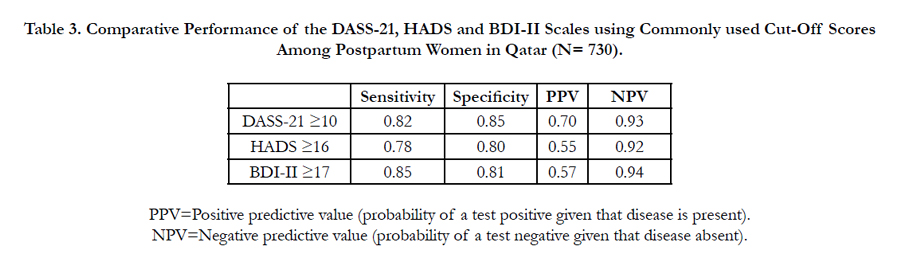
Table 3. Comparative Performance of the DASS-21, HADS and BDI-II Scales using Commonly used Cut-Off Scores Among Postpartum Women in Qatar (N= 730).
Table 4 shows the degree of agreement among DASS-21, HADS and BDI-II. Agreement was highest between DASS-21 and HADS (kappa =80%, p <0.001), followed by agreement between DASS-21 and BDI-II (kappa =75%, p <0.001) and BDI-II with HADS (kappa=60%, p<0.001).
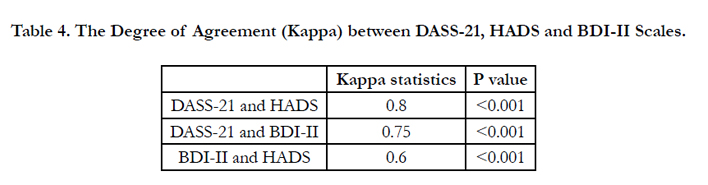
Table 4. The Degree of Agreement (Kappa) between DASS-21, HADS and BDI-II Scales.
Table 5 shows comparison area under the curve (AUC) of DASS- 21, HADS and BDI-II score. AUC was highest for DASS-21 , the area under the curve (AUC) was 0.86 (95% CI 0.83-0.89) for DASS-21, 0.84 (95% CI 0.80-0.88) for BDI-II and 0.83 (95% CI 0.80-0.86) for HADS scales.

Table 5. Comparison of Area Under the Curve (AUC) of DASS 21, HADS and BDI-II Score among Postpartum Women.
Figure 1 demonstrates ROC curve contrast of DASS-21, HADS, and BDI-II scores among postpartum women in Qatar. Reliability of DASS-21, HADS, and BDI-II was excellent with Cronbach’s alpha score of more than 0.80.
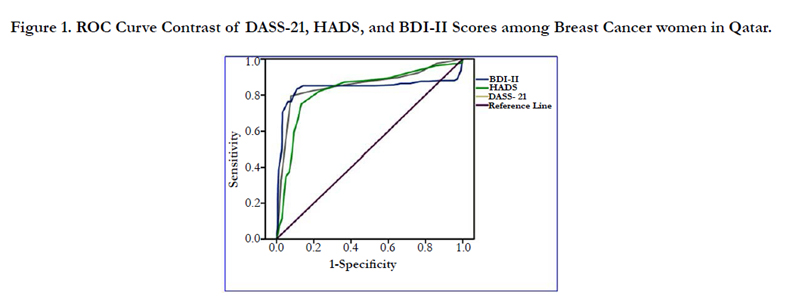
Figure 1. ROC Curve Contrast of DASS-21, HADS, and BDI-II Scores among Breast Cancer women in Qatar.
Discussion
Breast cancer is the most common cancer and the second principal cause of cancer deaths in women [1, 2]. Meanwhile, in the Arab world, breast cancer is ranked as the most frequent tumor in young women below 50 years of age and the current study is confirmative with the earlier reported study [2]. The current study assessed depression, anxiety and stress and risk factors in breast cancer patients from the State of Qatar during the treatment period. The prevalence rate of psychiatric morbidity was 23% by the DASS21 and with the mean score and standard deviation of 24.4 ± 5.7. Breast cancer diagnosis and treatment are often associated with psychological distress and reduced quality of life [6-9, 28, 29]. Studies of the quality of life of cancer patients can identify subgroups of patients at the greatest risk of psychological morbidity, who could benefit from interventions designed to assist them in coping with the disease and its treatment [15, 16, 29].
An individual’s perception and evaluation of psychological symptoms, well-being, and social functioning are likely to be affected by socio-economic status, culture, beliefs, and values. Although, the perceptions of breast cancer illness in Western Countries tend to be organized around dimensions of severity and conception of disease. In Eastern and far-eastern cultures, such as India, Philippines and China, illness perception also includes spiritual and psychological dimensions. In fact, Middle-East and Arab women share a unique set of cultural norms, beliefs and values. Therefore, assessment of psychological depression, anxiety, stress and in breast cancer patients after treatment may reveal findings that will ultimately require different approaches for assistance in coping with their psychological and medical condition.
Our study is the first to compare the psychometric performance of three depression screening instruments among postpartum women. Moreover it is the first to determine the validity and reliability of the DASS-21 instrument in Arab postpartum women. It demonstrates that the DASS-21 is the most accurate in detecting postpartum depression among Arab women. The DASS-21 had satisfactory concurrent validity compared to the BDI and HADS scores. We found that the 10 cut-off points are substantially better in detecting depression. The internal validity as measured by Cronbach's alpha coefficient was excellent and over 80%. Moreover, the DASS-21 was sensitive to the severity of depression. The mean DASS-21 score of women with major depression was higher than that of those with depressive disorder not otherwise specified, which in turn was higher than the mean score of the non-depressed women. The Arab women DASS-21 had satisfactory sensitivity and specificity in identifying depression in early stages. This is consistent with the previous reported DASS21 studies [1, 12, 18, 25-30]. The DASS21 proved to be a valid and reliable psychometric instrument in terms of screening for depressive disorders in Breast Cancer women. In the oncology setting, DASS21 maintains adequate sensitivity, acceptable specificity, and high NPV but low PPV for diagnosing Breast Cancer with an optimum cutoff score ≥10.
Overall depression and quality of life of Arab women who underwent mastectomy was not different from those who received lumpectomy. These findings are in agreement with those reported among Australian patients with breast cancer [31]. Nonetheless, high levels of depression were, as expected, The observed depression rate in this study was higher than in many industrialized countries [8, 9, 11-16]; however, in our study, breast cancer depression, anxiety and stress was an important public health problem in a high income per-capita and rapidly developing country. In a previous study reported by Bener et al.(yr?) the family history of breast cancer was significantly more often in breast cancer patients (14.4%) than in controls (6.2%) (p=0.002), but, the study revealed the lack of association between breast cancer and the parental consanguinity in Arab women residing in Qatar. In recent years, the genetic predisposition to breast cancer has advanced significantly, approximately 10 – 15% of all breast cancers are thought to have a hereditary component [32, 33]. One of the most important risk factors contributing to the preponderance of genetic disorders in Arab population is the deep-rooted norm of consanguineous marriages. Marriages between relatives are common worldwide and lead to human consanguinity. The present study revealed that there were statistically significant differences between consanguineous marriage compared to the non-consanguineous marriages.
The State of Qatar during last decade has been undergoing a social and cultural transformation [4, 19]. Traditional eastern values and social structures are becoming less important, but a western social infrastructure has not yet been established to support women. In other words, the household responsibilities of women have not decreased but they have been also carrying outside responsibilities, there were statistically significant differences between working and not working women. Beside these, there are various other chronic social problems impacting women’s health including, high birth rate, low education level, poverty, insufficient health care delivery, and an inadequate social security system in the country. Although, depression is under-diagnosed in breast cancer population since depression can have heavy impact on quality of life in breast cancer patients [18]. Many authors suggested that depression and stress symptoms may affect compliance with cancer therapy, reduce survival and quality of life [6, 18, 28]. However, without such a valid screening device, breast cancer depression might be under-recognized in Qatar because of somatic presentation of depression, inadequate liaison with psychiatric services and insufficient community health care services. Thus, this scale would also be applicable for the Arab women populations in other parts of Arabian Gulf countries, particularly states near Qatar which share a common dialect.
Our study suggests that the Arab version of the DASS-21 appears to be a satisfactory instrument for screening for breast cancer depression, anxiety and stressed women and DASS-21 has satisfactory concurrent validity compared with the BDI and HADS scores. The internal validity as measured by Cronbach's was excellent at over 80%. Moreover, the DASS21 was sensitive to the severity of depression. The mean DASS-21 score of the women with major depression was higher than that of those with depressive disorder not otherwise specified, which in turn was higher than the mean score of the non-depressed women. The Arab women DASS-21 has satisfactory sensitivity and specificity in identifying depression in early postpartum. Women who scored above a threshold of 10 are likely to be suffering from depression of significant severity, and should therefore be further assessed to confirm whether clinical depression is present or in development. We found that the 10 cut-off point is substantially better in detecting depression. This illustrates the importance of proper validation in the cross-cultural application of a psychiatric rating instrument. Furthermore, the DASS-21 was used in preference to the HADS used in previous surveys as it includes a scale for anxiety symptoms. The DASS-21 has good psychometric properties and the depression scale correlates well with the HADS.
Conclusion
The Arab version of the DASS-21 exhibited the most satisfactory psychometric properties and its use for research and health care practice is warranted. The DASS-21, BDI-II and HADS have excellent sensitivity, and specificity to quickly screen for breast cancer depression among women. Agreement is highest among DASS-21 and HADS in the Arab population. Overall, the DASS-21 performed better than the other tools based on sensitivity, specificity, and positive predictive value (PPV) and negative predictive value (NPV). Moreover, it is very practical to use the DASS-21 instrument as it is a brief, easy to administer inventory that may assist GP practitioners, psychiatrists and psychologists to more effectively assess and treat new breast cancer women who may be depressed, anxious and/or stressed in the chemotherapy period.
Acknowledgments
This study was generously supported and funded by the Hamad Medical Corporation. The authors would like to thank the Hamad Medical Corporation for their support and ethical approval (HMC RP # 12215/12 and HMC RP # 12061/12).
References
- World Health Orgniztion (2014): The Global Burden of Disease. Geneva, Switzerland: WHO press; 2016.
- Globocan cancer fact sheet. Breast Cancer Incidence and Mortality Worldwide, 2012.
- Glanz K, Lerman C (1992) Psychosocial impact of breast cancer: a critical review. Behav Med. 14: 204-212.
- Bener A, El Ayoubi H, Kakil R, Ibrahim W (2007) Patterns of Cancer Incidence among the Population of Qatar: A Worldwide Comparative Study. Asian Pac J Cancer Prev. 9(1): 19-24.
- Walker LG, Walker MB, Heys SD, Lolley J, Wesnes K, et al., (1997) The psychological and psychiatric effects of rIL-2 therapy: a controlled clinicaltrial. Psycho-oncol. 6(4): 290–301.
- Ollonen P, Lehtonen J, Eskelinen M (2005) Anxiety, depression and the history of psychiatric symptoms in patients with breast disease: a prospective case-control study in Kuopio, Finland. Anticancer Res. 2527-2534.
- Howard R, Harvey (1998) P: A longitudinal study of psychological distress in women with breast symptoms. J Health Psychol. 3(2): 215–226.
- Rodgers J, Martin CR, Morse RC, Kendell K, Verrill M (2005) An investigation into the psychometric properties of the Hospital Anxiety and Depression Scale in patients with breast cancer. Health Qual Life Outcomes. 3: 41.
- Nordin K, Berglund G, Glimelius B, Sjoden PO (2001) Predicting anxiety and depression among cancer patients: a clinical model. Euro J Cancer. 37(3): 376–384.
- Zigmond, AS, RP Snaith (1983) The hospital anxiety and depression scale. Acta Psychiatr. Scand. 67(6): 361–370.
- Bjelland I, Dahl AA, Haug TT, Neckelmann D (2002) The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosomatic Res. 52: 69–77.
- Herrmann C (1997) International experiences with the Hospital Anxiety and Depression Scale – a review of validation data and clinical results. J Psychosomatic Res. 42: 17–41.
- Hall A, A'Hern R, Fallowfield L (1999) Are we using appropriate self-report questionnaires for detecting anxiety and depression in women with early breast cancer? Euro J Cancer. 35(1): 79–85.
- Saboonchi F, Wennman-Larsen A, Alexanderson K, Petersson LM (2013) Examination of the construct validity of the Swedish version of Hospital Anxiety and Depression Scale in breast cancer patients. Qual Life Res. 22(10): 2849-2856.
- Osborne RH, Elsworth GR, Sprangers MA, Oort FJ, Hopper JL (2004) The value of the Hospital Anxiety and Depression Scale (HADS) for comparing women with early onset breast cancer with population-based reference women. Qual Life Res. 13(1): 191-206.
- Kamińska M, Kubiatowski T, Ciszewski T, Czarnocki KJ, Makara-Studzińska M, et al., (2015) Evaluation of symptoms of anxiety and depression in women with breast cancer after breast amputation or conservation treated with adjuvant chemotherapy. Ann Agric Environ Med. 22(1): 185-189.
- Alcalar N, Ozkan S, Kucucuk S, Aslay I, Ozkan M (2012) Association of coping style, cognitive errors and cancer-related variables with depression in women treated for breast cancer. Jpn J Clin Oncol. 42(10): 940-947.
- Eskelinen M, Ollonen P (2011) Beck Depression Inventory (BDI) in patients with breast disease and breast cancer: a prospective case-control study. In Vivo. 25(1): 111-116.
- Bener A, El-Ayoubi HR, Moore MA, Basha B, Joseph S, et al., (2009) Do We Need to Maximise The Breast Cancer Screening Awareness? Experience with an Endogamous Society With High Fertility. Asian Pac J Cancer Prev. 10(4): 599-604.
- Beck AT, Epstein N, Brown G, Steer RA (1988) An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 56(6): 893-897.
- Lloyd-Williams M, Friedman T, Rudd N (2001) An analysis of the validity of the Hospital Anxiety and Depression scale as a screening tool in patients with advanced metastatic cancer. J Pain Symptom Manage 22(6): 990–996.
- Bener A, Al-Hamaq AOAA, Dafeeah E (2011) High Prevalence of Depression, Anxiety and Stress Symptoms among Diabetes Mellitus Patients. Open Psychiatr J. 5: 5-12.
- Lovibond PF, Lovibond SH (1995) The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 33: 335-343.
- Bener A, Gerber LM, Sheikh J (2012) Prevalence of Psychiatry Disorders and Associated Risk Factors in Women during their Postpartum Period: A Major Public Health Problem and Global Comparison. Int J Women’s Health. 4: 191-200.
- Henry JD, Crawford JR (2005) The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br J Clin Psychol. 44: 227–239.
- Bener A, Yousafzai MT (2012) Comparison of Reliability and Validity of the Postpartum Depression Anxiety Stress Scales (DASS-21) with the Beck Depression Inventory (BDI-II) and Edinburgh Postpartum Depression Scale (EPDS) in Arabian Women. International Journal of Applied Sc. & Computations.19(2): 141-156.
- Antony MM, Bieling PJ, Cox BJ, Enns MW, Swinson RP (1998) Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales (DASS) in clinical groups and a community sample. Psychol Assess. 10: 176-181.
- Reich M, Lesur A, Perdrizet-Chevallier C (2008) Depression, quality of life and breast cancer: a review of the literature. Breast Cancer Res Treat. 110(1): 9-17.
- Koo J, Hood N ,et al., (2004) Health-related quality of life and psychological status in breast cancer prognosis: analysis of multiple variables. J. Clin. Oncol. 22(20): 4184-4192.
- Gloster AT, Rhoades HM, Novy D, Klotsche J, Senior A, et al., (2008) Psychometric properties of the Depression Anxiety and Stress Scale-21 in older primary care patients. J Affect Disord. 110(3): 248-259.
- King MT, P Kenny, J Shiell, Hall J, Boyages J (2000) Quality of life three months and one year after first treatment for early stage breast cancer: influence of treatment and patient characteristics. Qual Life Res. 9(7): 789-800.
- Bener A, El Ayoubi HR, Ali AI, Al-Kubaisi A, Al-Sulaiti H (2010) Does consanguinity lead to decreased incidence of breast cancer? Cancer Epidemiol. 34(4): 413-418.
- Lichtenstein P, Holm NV, Verkasalo PK, Lliadou A, Kaprio J (2000) Environmental and heritable factors in the causation of cancer: analysis of cohorts of twins from Sweden, Denmark, and finland. N Engl J Med. 343(2): 78-85.





