Analysis of Psycho Social Stresses In Family History of Suicide Victims by Suicidal Hanging
Malini. S1, Roy A2*
1 Assistant Director, Forensic Science Laboratories, Bangalore, India.
2 Research Scholar, Bangalore, India.
*Corresponding Author
Abhijit Roy,
Research Scholar working in the area of Forensic Psychology,
Bangalore,India.
E-mail: roy.abhijit009@gmail.com
Received: June 12, 2015; Accepted: October 10, 2015; Published: October 15, 2015
Citation: Malini. S, Roy A (2015) Analysis of Psycho Social Stresses In Family History of Suicide Victims by Suicidal Hanging. Int J Behav Res Psychol,3(8), 146-149. doi: dx.doi.org/10.19070/2332-3000-1500026
Copyright: Roy A© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The third causes of death among youths worldwide is suicide. Suicide rate in India is approximately 11.4 per 1 lakh in male and 8.0 per 1 lakh in female. In Indian study predominant suicidal victims are males, literates, married and from rural background. Aim of the present study is to asses Psychological factors, socio demographic characteristic in relation to family history of suicide associated with complete suicide by hanging. Out of 128 suicidal cases 80 cases which meet the criteria were selected for the present study. Data were collected using semi structured performer for the demographic, psychological, social, tying pattern. Knot analysis for type and handedness were analysed for family history and without the family history of suicide cases. More than 60% of suicide victims were in the age group of 15 to 34 yrs. Male outnumbered females in this study. Psychosocial stress were found in 71% of suicide victims. Granny or Reef knots were the most preferred used for suicidal hanging with family history of suicide. Using right hand proved left hemisphere dominance. Specific focus on identifying psychosocial factors, demographic variable, and increase risk of suicide can be identified at an early stage. The present study indicates that Suicide prevention strategies through family education programme can prevent the rate of suicide with family history and without family history of suicide.
2.Introduction
3.Methods
3.1.Newspaper report
3.2.Police station
3.3.Office of register of birth & death
3.4.Interaction with the family of the suicide victim
3.5.Interaction with Forensic Medicine experts
4.Results
5.Discussion
6.Conclusion
7.Acknowledgement
8.References
Keywords
Stress; Psychological Factors; Suicidal Hanging; Family History; Family Education.
Introduction
Suicide is an outcome of a complex process that begins with the idea of suicide followed by active attempts and eventually death of the individual.
A recent WHO [1] report reveal that the number of suicides in India accounted for yearly third of the global total and more than twice as many in China which is second on the list. The high rate of committing suicide were noticed among the young group of people between age group of 15 to 30 years in India.
National Crime Record Bureau (NCRB) [2] says that the number of suicide increased to 1, 34,799 in 2013 from 1, 10,851 in 2003. India also has witnessed spur in farmer suicide cases because of drought, unable to pay back bank loan because of deficit Monsoon rain.
According to NCRB [2] report (2013) highest incident of suicide of 16,622 suicide were reported from Maharashtra followed by 16,610 in Tamil Nadu. Both the state accounted 12.3% of total suicide. Andhra Pradesh, West Bengal & Karnataka accounted for 10.8%, 9.7% & 8.4% respectively of the total suicide report in the country. These five states together accounted for 53.5% of total suicide reported in the country.
WHO [1] report reveals that pesticide, hanging & firearms are the most common methods of suicide at the global level.
Majority of suicide victims (37.80%) in India are those below the age of 30 yrs. This imposes a huge social, emotional & economic burden on society. Thus suicide is the major public and mental health problem which demands the urgent action. Suicide in family members appears to be a predisposing factor for suicide irrespective of psychopathology. The available literature has also highlighted genetic transmissions thus indicating hereditary aspects in suicidal behaviour. However environmental effects have also been identified. The usage of right hand were noticed in all the samples with family history of suicide collected for the study indicating that the victims were left hemisphere dominant. Left side of the brain unable to find out the logical solution coupled with hereditary aspects along with delusion of unworthiness and helplessness resulting in such self-destructive behaviour [3]. The available literature has indicated that simple knots are used in homicide hanging while granny or reef knot are absorbed in all samples collected in the present study for the suicidal hanging. The studies have indicated that veil or soft ligature material commonly used for hanging with family history and without family history of suicide [4]. The knot analysis which assist in driving useful information has been clearly articulated in a clear and systematic manner in the available literature.
In the present study an attempt has made to explore psychological factors, social factors coupled with family history associated with suicide.
Methods
The sample consists of 80 cases that occurred in the general population residing in an around Bangalore city during the year 2013-2014.
The data was collected from the following five sources.
The suicidal cases reported in all daily newspaper of Karnataka were collected. Suicidal reports in English and Kannada paper were compared to determine replication of same case. From newspaper the concern jurisdiction police station were noted.
The jurisdiction of police station were visited to verify the authenticity of the statement reported in the newspaper. The available information of various identification data of the victims like age, sex, marital status, suspension of the dead body along with place of incidence, time and suspected cause of death were noted from the inquest report available in the police records and were sorted in a tabular format
Information regarding death due to suicide and confirmation of address of suicide victims were obtained from register of birth & death.
Questionnaires related from childhood till the day of suicide, various factors developmental milestone, education, peer relation, occupation, interaction and interpersonal problems with family members or significant members, learning difficulties or psychosocial stresses, family history of suicide, psychiatry problem were recorded in detail. The questionnaire consisting of 40 questions which covered all psychosocial factors, psychosocial stresses including handedness of the victim.
The Forensic Medicine experts who had conducted the postmortem on suicide victim were interacted to collect information relating to ligature material, ligature mark, injury to neck structure type of knots, handedness and other related aspects from postmortem examination. The information collected from the above sources were tabulated for cross-checking and to avoid duplication. The interaction with the Forensic Medicine expert gave a detailed autopsy information related, position of mark, type of mark, material used, position of knot, type of knot, number of knot and other related information.
A semi structured Performa was used to collect demographic details of each suicidal cases from the jurisdiction police station. A semi structured Performa to asses psychosocial stresses associated with suicide victim were used in obtaining the information from a key informant of the suicide victim. Key informant are the family members of the victim and who are living with the suicide victim for not less than five years.
Results
In present study majority of suicide victims were in the age group of 15 to 34 years. The data so collected were analysed statistically by using descriptive statistics.
In the present study 61.25% of the cases were in the age group 15-34 yrs. Followed by that 15% were found in the age group of 45-54 yrs. 55 & above age group were found under 12.50% and the least was found with the age group of 35-44 yrs. which was only 9%.
The study has indicated that males 67.50% has outnumbered females 32.50% in this study. A large number of victims 77% were literate and 23% were illiterate. The student population were foundto be of 33.5%, semi-skilled workers were 39% and remaining were retired, part-time employed, unemployed, housewives. 61% of the victims were married, 34% were unmarried, and 5% were divorcee, widow, and widower. 48.5% of the victims had migrated from rural area and 51.5% from the urban background. The male outnumbering female in hanging cases is similar to the study made by Sharma & Harish et.al (2005) [5]. The difference in gender that are found in the study appears that Indian female are capable of facing the problem with responsibility, courage probably due to strong emotional ties with family and children [6].
Family history of suicide was a significant risk factor for suicide independent of family history of severe mental disorder. The rate of suicide was twice as higher in family of suicide victims compare to other family. Strongest risk factor for the suicide in the family as mental disorder has been indicated in many literatures but family history of suicide independent of severe mental disorder was a significant risk factor. Suicide in family members appears to be predisposing factors for suicide irrespective of psychopathology. Available literatures have also highlighted genetic transmission thus indicating hereditary aspects in suicidal behaviour. However the environmental effect also has been indicated.
The victims of suicide with family history of suicide have more interpersonal stress and more academic problems compare to the suicidal victims without family history of suicide. The psychosocial stress were found in more than 71% of the suicidal victims with family history of suicide, 14% victims due to financial stresses and 15% were interpersonal stress, physical stress and alcohol/substance abuse. Among the interpersonal stresses due to marital discord, love failure, social dejection, unemployment, poverty, loss of job, job changes which are the occupational stress were found to be the major causes of poor socio economic status and thus had become the cause of suicide. The academic failure is seen more 19% of the younger population. The financial stress like losses of money due to gambling, unable to pay the debt, unable of payment towards the major illness, loss of job, job changes were also seen in 6% of the migrants of rural areas compare to that of urban areas. The findings of the present study is similar to the earlier findings [7]. Loss of property due to gambling, alcohol and drug addiction, luxurious living and disease like HIV, cancer, skin related and stomach related problem and incurable pain are some of the stressors that were reported by the family of the suicide victims.
Behavioural changes were seen in most of the suicidal victims of family history of suicide before 2 to 3 months of the actual act. Some of the suicidal victims were reported to be of highly aggressive and irritable before the suicidal act. Most of the suicide victims were depressed, reported their intention towards committing suicide to their family member and friends. Suicidal notes and audio/video recording were being found in few cases.
The migration from the rural areas in search of jobs, academic failure and poor socio economic status were the high risk factor along with the psychosocial stress among the male to commit suicide. The present study endorses the previous research finding by Narang et.al, [8] in their study on attempted suicide in Ludhiana.
The ligature material which were the most commonly used in hanging cases are Saree, followed by veil, bedsheet & curtain in both suicidal cases with family history and without family history of suicide. The hard materials like nylon rope, iron chain, cable wire had been the least choose of the ligature material by those victims. It has been observed that the person favouring hanging with history of suicide uses easily accessible material and attempts without planning or technical knowledge. The findings of the present study is similar to the finding by Choudhury et.al. [9], in their research study on suicidal hanging vs homicidal hanging have indicated that soft material are the most preferred choice than the hard material as a preferred ligature material for suspension. Majority of the suicidal victims with positive family history preferred granny knot or reef knot for constricting their neck due to their previous exposure in the family. 78% of the cases granny knot were found and in rest 28% of the cases multiple knot were found. Ahmad et.al, [10] in his study on Hanging as a method of suicide has indicated usage of soft material for suspension is similar to the findings of the present study.
Right hand was the most preferred hand to tie up the knot relating to tying habit in the present study. 82% of the cases right hand victims accounted for higher number indicating left hemisphere dominance. Followed by this were 10% ambidextrous and least 8% of the cases victims used left hand to tie up the knot in suicidal cases. The study has confirmed the hemisphere dominance in relation to knot tying habit [3].
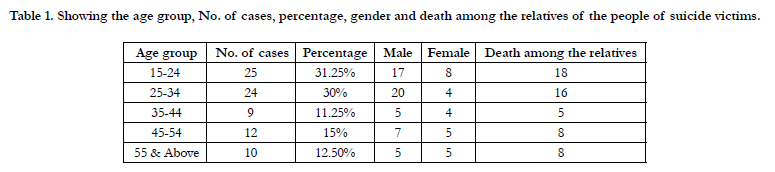

Table 1. Showing the age group, No. of cases, percentage, gender and death among the relatives of the people of suicide victims.
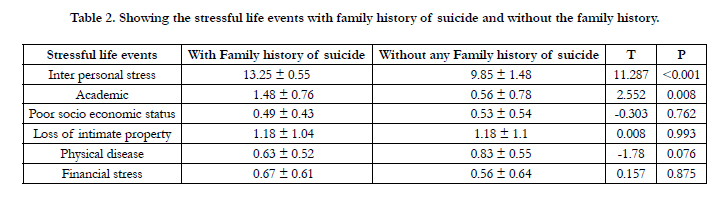
Table 2. Showing the stressful life events with family history of suicide and without the family history.
Discussion
While facing the changes of life style uncertainty about their future, victim have drawn the idea of committing suicide as a way to achieve emotion relief or escaping from the stress. Male have become vulnerable to suicide due to frustration in job or hunting for job. The victims between 15-34 yrs. have a higher rate of suicidal act due to mismatch between preference and reality, unable to cop up with the reality, fanciful, reluctant to express their emotion outwardly because of the cultural background immature coping shortage are the causes of suicide.
Family history of suicide and family history mental disorder are the two risk factors that the National Institute of Mental health lists. Suicide, Peterson has said that can represent Learned or transmitted way of coping with unbearable stress. Unable to find logical solution and with their previous exposure to suicide behaviour among the relative of suicide victim, suicide becomes one of the escaping act.
Conclusion
The suicide is the complex phenomena affected by variety of biological, social and psychological factors. Social transformation, social support and education of immature coping strategies to handle negative left event in an integrated manner is required. Multiple approaches should be adopted for intervention with the goal of suicide prevention [11]. Family education programme for early identification risk of suicide are urgently required. The priority areas to achieve this goal requires promoting and supporting mental health services, NGO’s, primary care workers, and trained a gate keeper like teachers, police officers, counsellor/psychologist, researchers, clinicians, policymakers and survivor from suicidal acts. Work place culture should made the workers feel comfortable. Thus reducing the job stress Employee Assistants Programme (EAP) should be made available in all work places. Warning sign of the suicide should be recognised at an early stage. Stress free environment should be created and if stress is recognised action should be taken to reduce the stress [12].
Increase in tendency of suicide by hanging is seen in more amount of youth. Government has to take steps to tackle this growing menace at the grass root level.
Acknowledgement
The authors reported no conflict of interest. The authors alone are responsible for the content of writing of the paper and funding have received on this work. Ethical approval was not required.
References
- World Health Report (2013). Mental Health-New Understanding New Hope. World Health Organization (WHO), Geneva.
- Accidental Deaths and suicides in India (2013). National Crime Records Bureau. Ministry of Home Affairs. Government of India.
- Chisnall RC (2010) Knot-tying habits, tier handedness and experience. J Forensic Sci 55(5): 1232-1244.
- Sharija S, Sreekumari K, Geetha O (2011) Epidemiological Profile of Suicide by Hanging in Southern Parts of Kerala: An Autopsy based Study. J Indian Acad Forensic Med 33(3): 237-240.
- Sharma BR, Harish D, Virender PS, Preminderjeet S (2005) Ligature mark on neck: How Informative? J Indian Acad Forensic Med 27(1): 10-15.
- Chavan BR, Singh GP, Kaur J, Kochar R (2008) Psychological autopsy of 101 Suicide cases from Northwest region of India. Indian J Psychiatry 50(1): 34-38.
- Kumar PN (2004) An analysis of suicide attempters versus completers in Kerala. Indian J Psychiatry 46(2): 144-149.
- Narang RL, Mishra BP, Nitesh M (2000) Attempted suicide in Ludhiana. Indian J Psychiatry 42(1): 83-87.
- Choudhry BL, Sharma RK, Deepak S (2012) Suicidal hanging versus Homicidal hanging. A case report. Indian J Forensic Med Toxicol 2(2): 32-33.
- Ahmad M, Hossain MZ (2010) Hanging as a Method of Suicide: Retrospective Analysis of Postmortem Cases. Journal of Armed Forces Medical College, Bangladesh 6(2): 37-39.
- Payne-James J, Busuttil A, Smock W (2003) Forensic medicine: clinical and pathological aspects. Cambridge University Press, UK. 266-269.
- Resnick H (1972) Eroticized repetitive hangings: a form of self-destructive behaviour. Am J Psychother 26: 4-21.





