Pediatric Renal Transplantation in Children with Weight 20kg or Less: A Single-Center Experience
I Arruza Urquijo1, G Ojinaga García1, M Herrero Goñi2, M Aguirre Meñica2, L Madariaga Dominguez2, C Gonzalez Paniagua1, I Grijalba Ipiñaza1, G Najarro Ajuria1, G Ortiz Labrador1, L Martinez Goenaga1, A Arruza Echevarría3, A Mavarez-Martinez4*, N Stoicea4, SD Bergese4,5, A Martinez Ruiz1
1 Department of Anesthesiology, Hospital Universitario de Cruces, Baracaldo, Vizcaya, Spain.
2 Department of Pediatric Nephrology, Hospital Universitario de Cruces, Baracaldo, Vizcaya, Spain.
3 Department of Urology, Hospital Universitario de Cruces, Baracaldo, Vizcaya, Spain.
4 Department of Anesthesiology, The Ohio State University Wexner Medical Center, Columbus, OH, USA.
5 Department of Neurological Surgery, The Ohio State University Wexner Medical Center, Columbus, OH, USA.
*Corresponding Author
Ana Mavarez-Martinez MD,
Department of Anesthesiology, The Ohio State University,
Wexner Medical Center, Columbus, OH, USA.
Tel: 614-293-3559
Fax: 614-366-1943
E-mail: ana.mavarezmartinez@osumc.edu
Received: January 07, 2019; Accepted: January 30, 2019; Published: January 31, 2019
Citation: I Arruza Urquijo, G Ojinaga García, M Herrero Goñi, M Aguirre Meñica, L Madariaga Dominguez, A Mavarez-Martinez, et al., Pediatric Renal Transplantation in Children with Weight 20kg or Less: A Single-Center Experience. Int J Anesth Res. 2019;7(1):555-564. doi: dx.doi.org/10.19070/2332-2780-19000112
Copyright: MM Ana© 2019. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Renal transplantation (RT) is the treatment of choice for children with Chronic Kidney Disease (CKD). This technique benefits survival and quality of life. Long-term outcomes in pediatric transplantation have significantly improved over the past 20 years; however, children less than 5 years of age weighing 20 kg or less still remain a considerable challenge, with higher mortality rate and graft loss.
Methods: In this article, we present the pediatric RT experience at Hospital Universitario de Cruces, the main center for transplants in Spain. Children who underwent RT within the period of January 2012 - January 2017 were retrospectively reviewed to identify those with weight less than 20 Kg. The following parameters were collected: pre-transplant characteristics, surgical technique, anesthesia characteristics, intra-operative and post-operative surgical or medical complications, pre and post-transplant creatinine levels, renal graft survival, and late post-operative complications.
Results: Within a period of 5 years, a total of 13 pediatric patients (weight ≤ 20kg) underwent RT at Hospital Universitario de Cruces. The patient sample represented 37.14 % of the 35 renal transplants performed on pediatric patients at this institution. All 13 patients received a standard surgical and anesthetic perioperative management. Post-transplant creatinine levels significantly decrease after surgery during the early postoperative period from 6.45 mg/dl preoperatively (range, 1.90 - 12.26) to 0.59 mg/dl postoperatively (range, 0.27 - 1.27). The mean follow-up period was 1.5 year (range, 1 - 3) with 12 patients out of 13 (92.31%) presenting with 1-year graft survival.
Conclusions: A multidisciplinary collaboration, including surgeons, nephrologists, and anesthesiologists specialized in handling transplants for underweight children should be a priority. Close intraoperative monitoring of vital signs and optimal fluid therapy is essential for anesthetic management due to the possible perioperative hemodynamic changes.
2.Abbreviations
3.Introduction
4.Methods
4.1 Statistical Analysis
5.Results
5.1 Pre-transplant Patient Characteristics
5.2 Surgical Technique
5.3 Perioperative Monitoring
5.4 Intraoperative Management
5.5 Postoperative Management
5.6 Postoperative Complications
5.7 Graft Survival
6.Discussion
6.1 Preoperative Assessments
6.2 Intraoperative Management
6.3 Postoperative Management
7.Conclusions
8.References
Keywords
Renal Transplantation; Anesthesia; Kidney Failure; Pediatric; Low weight; Transplant Surgery.
Abbreviations: ASA
RT: Renal Transplantation; CKD: Chronic Kidney Disease; CVP: Central Venous Pressure; PICU: Pediatric Intensive Care Unit; CMV: Cytomegalovirus; EBV: Epstein-Barr Virus; BKV: BK Virus; MPA: Mycophenolic Acid; WHO: World Health Organization; PRBC: Packed Red Blood Cells; MMF: Methylprednisolone–Mycophenolate Mofetil; MMR: Mumps and Rubella; CVC: Central Venous Catheter; NSAIDS: Nonsteroidal Anti-Inflammatory Drugs; PiCCO: Pulse Contour Cardiac Output; UTI: Urinary Tract Infections.
Introduction
Renal transplantation (RT) is the treatment of choice for children with chronic kidney disease (CKD) and is clearly superior to the various dialysis techniques when considering long-term outcomes. Before 1980, adolescents and children with CKD were rarely candidates for transplantation and few were selected to undergo dialysis. After that decade, a gradual increase in pediatric transplantation was reported with specific pediatric anesthetic requirements and with more complex surgical techniques [1, 2].
The outcomes of RT have improved dramatically since 2000. Advances in nephrology, nutrition, anesthesia, transplant surgery, improved postoperative management, and effective immunosuppressive protocols have led to an increase in the survival rate of pediatric patients undergoing RT. Despite these advances, underweight (≤ 20 kg) children remain being a significantly challenging population, with higher rates of mortality and graft loss after RT [2].
Access to different dialysis techniques before RT has become an important tool. Patients with previous abdominal surgery who are unable to undergo peritoneal dialysis or those with prior failure of double lumen catheters unable to undergo hemodialysis can be benefited from other dialysis techniques [3]. Dialysis techniques adjusted to accommodate very low weight patients have increased the survival rate for children; nevertheless, the incidence of complications in this group remains high [4].
The type of graft selected to be transplanted can impact outcomes on RT. Smaller grafts from deceased pediatric donors, especially below 2 years of age, have not been a viable option until recently. New surgical techniques like using both donated kidneys en bloc into the recipient aorta segment have become an alternative procedure. Similarly, parents and relatives have become candidates for living donation, although it is recommended to have a certain ratio between the size of the kidney that is being received and the available space in the abdomen of the recipient [5].
Anesthesia management during RT plays an important role on early graft function. An appropriate blood pressure adjustment during surgery with continuous monitoring of central venous pressure (CVP) and good perioperative fluid and electrolyte management results in improved graft outcomes [6]. Likewise, postoperative admission to the pediatric intensive care unit (PICU) to achieve a steady hemodynamic state is essential for post-RT management. Large fluid volumes infused during surgery in order to support mean arterial blood pressure and to maintain a state of intraoperative hypervolemia before graft reperfusion can result in pulmonary edema requiring postoperative ventilation in recipients ≤ 20 kg [7].
Surgical complications may manifest in both the early and late postoperative period. This problem is worse in underweight patients, due to the miniscule vascular anatomy, increased risk of developing thrombosis, and hemodynamic changes that may occur after graft revascularization. Surgical complications may be further divided into lymphatic complications such as lymphocele formation and other general surgery complication such as urinary leaks [8]. Infections can also delay the graft function after RT. The risk of developing late postoperative viral infections by opportunistic viruses such as cytomegalovirus (CMV), Epstein-Barr virus (EBV) or BK virus (BKV), is a clinical challenge considering the immunosuppressive therapy to prevent graft rejection [9].
The goal of this retrospective medical records review (January 2012 to January 2017) was to assess pediatric RT outcomes with the aim to analyze trends in anesthesia and surgical techniques, early and late post-transplant complications, and to report graft and patient survival.
Methods
This retrospective chart review included pediatric patients who underwent RT between January 2012 and January 2017 at Hospital Universitario de Cruces, Spain who weighed less than 20 kg at the time of transplantation. This chart review was approved by the Institutional Ethics Committee prior to data collection. The following data was reviewed: demographics of donors and recipients, etiology and characteristics of the disease, and performance or nonperformance of dialysis techniques before the transplantation. The following clinical aspects were also reviewed: pre-transplant and post-transplant immunosuppression, medical complications, intra-operative surgical complications, anesthesia characteristics, complications at PICU, pre-transplant and posttransplant creatinine levels at discharge from PICU, renal graft survival, and late post-operative complications.
Summary statistics were estimated and summarized as means (standard deviations) for continuous variables and frequencies (percentages) for categorical variables. Results were reported as tables and charts. The database was collected in Microsoft Excel®. No formal hypothesis testing was performed since variables and outcomes were analyzed only for one group.
Results
Within a period of 5 years (January 2012 -January 2017), a total of 35 pediatric transplants were performed at Hospital Universitario de Cruces; 13 out of 35 transplanted patients (37.14%) weighed ≤ 20 kg.
Out of the 13 RT recipients, 9 patients (69.23%) were males and 4 patients (30.77 %) were females with mean age 4.46 years (range, 2 – 8), mean weight 17.15 Kg (range, 14 - 20), and mean waiting time until RT 15.7 months (range, 1.81 - 52.77). CKD of two different etiologies were diagnosed: congenital uropathy in 10 patients (76.92%) and acquired nephropathy in 3 patients (23.08%) due to meningococcal sepsis, hemorrhagic shock, and idiopathic cause respectively. Before RT, 6 patients (46.15%) exhibited polyuria with increased hydration requirements, 7 patients (53.84 %) required use of gastrostomy for nutritional support, and 2 patients (15.38 %) presented hyperkalemia with preoperative values of 6.4 mEq/L and 4.9 mEq/L respectively (values returned to normal range after calcium chloride administration). Peritoneal dialysis was performed before RT for 6 patients (46.15 %), hemodialysis after peritoneal dialysis failure for 3 patients (23.08%), and 4 patients (30.77%) did not receive dialysis prior to their RT. All 13 patients completed the vaccination schedule according to their age before the procedure. Also, all 13 patients received induction immunosuppression of combined methylprednisolone, mycophenolic acid (MPA), and basiliximab (Table 1).
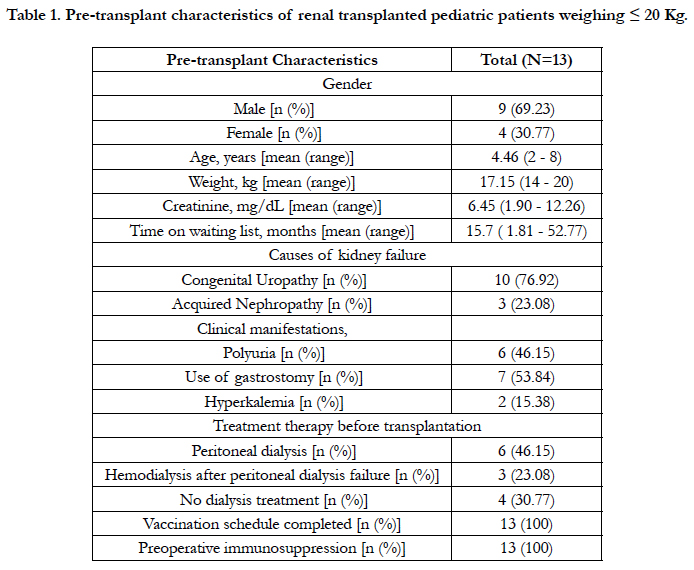

Table 1. Pre-transplant characteristics of renal transplanted pediatric patients weighing ≤ 20 Kg.
According to current weight-for-age world health organization (WHO) tables, weight for the study population was below normal (< 3rd percentile) in 1 patient (7.69%), normal (15th - 85th percentile) in 10 patients (76.92%), and above normal (>97th percentile) in 2 patients (15.38%). According to weight-for-height WHO tables, weight for the study population was below normal (3rd percentile) in 2 patient (15.38%), normal (15th - 85th percentile) in 7 patients (53.85%), and above normal (>97th percentile) in 4 patients (30.76%). In regards with height-for-age WHO tables, height was below normal (<3rd percentile) in 3 patients (23.08 %) and normal (15th - 85th percentile) in 10 patients (76.92 %) (Figure A).
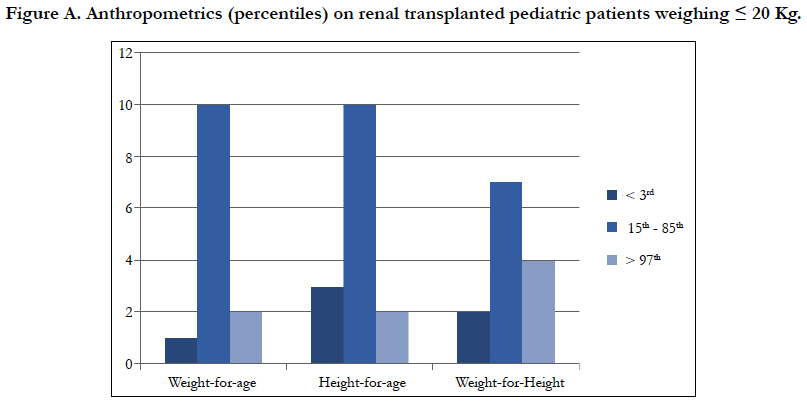
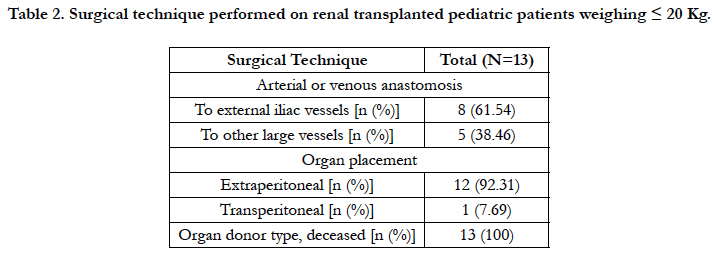
Table 2. Surgical technique performed on renal transplanted pediatric patients weighing ≤ 20 Kg.
Vascular anastomosis from the donated kidney to the recipient was performed to external iliac vessels in 8 patients (61.54%) and to other large vessels in 5 patients (38.46%). RT was performed in a standard extraperitoneal fashion in 12 patients (92.31%) and transperitoneal (extraperitoneal only in the upper pole), in 1 patient (7.69%). For all 13 RT, single-J ureteral stents and Penrose drains were routinely placed. Organs from deceased donors were used for all 13 RT (Table 2).
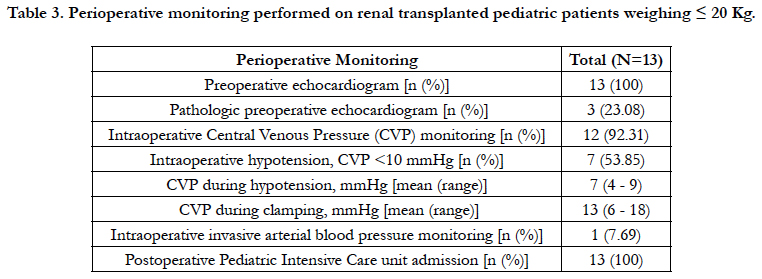
Table 3. Perioperative monitoring performed on renal transplanted pediatric patients weighing ≤ 20 Kg.
Echocardiogram was performed preoperatively in all 13 patients during their preoperative visit; 3 out of 13 patients (23.08%) were diagnosed with the following pathologies: mild mitral regurgitation, mild hypertrophic cardiomyopathy, and dilated versus hypertrophic cardiomyopathy with electric repercussion and mild systolic dysfunction (EF 50-53%). Intraoperatively, CVP was monitored on 12 patients (92.31%). Intraoperative hypotension, defined as CVP less than 10mmHg, was identified in 7 patients (53.85 %), with the mean CVP being 7 mmHg (range, 4 - 9). The mean CVP during clamping was 13 mmHg (range, 6 - 18). Invasive blood pressure through a radial arterial line was monitored only on 1 patient (7.69 %) per anesthesiologist criteria. Postoperatively, all 13patients (100 %) were extubated and transferred to PICU for postoperative monitoring and volume resuscitation management (Table 3).
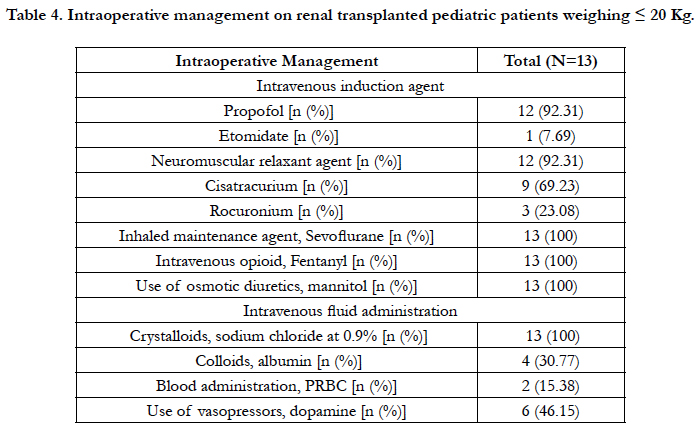
Table 4. Intraoperative management on renal transplanted pediatric patients weighing ≤ 20 Kg.
Intravenous anesthesia induction was performed with propofol in 12 patients (92.31%) and with etomidate in 1 patient (7.69 %) due to egg allergy. Neuromuscular relaxant was administered to 12 patients (92.31 %): cisatracurium for 9 patients (75 %) and rocuronium for the remaining 3 patients (25 %). For all 13 patients, the volatile agent used for anesthesia maintenance was sevoflurane and the opioid used was fentanyl. No complementary regional techniques were used for pain control, given the low patients weight. Intravenous fluid maintenance was performed with crystalloids - sodium chloride 0.9% (7 to 20 ml/kg/h). Prior to unclamping, mannitol (600 to 1000 mg/kg) was administered for all 13 cases (Table 4).
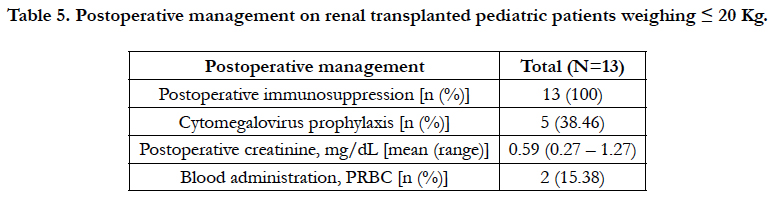
Table 5. Postoperative management on renal transplanted pediatric patients weighing ≤ 20 Kg.
Intraoperatively hypotensive patients (N = 7) received the following therapy: volume expansion with albumin (150 - 400 mg/ kg and) instituted for 4 patients (30.77 %) and continuous infusion of Dopamine (3.5 - 5 mcg/kg/min) for 6 patients (46.15 %). Two patients (15.38 %) required blood product administration of packed red blood cells (PRBC) at 10 - 20 ml/kg, based on preoperative hemoglobin value of 9.2 g/dl and 6.3 g/dl, respectively (Table 4).
During PICU stay, all 13 patients received immunosuppression after RT: 12 patients with a combination of methylprednisolonemycophenolate mofetil (MMF)-basiliximab and, 1 patient a combination of methylprednisolone-MMF-thymoglobulin due to sensitization as a result of previous failed transplant. For all 13 patients, tacrolimus was added to the immunosuppressive regimen after serum creatinine was measured below 3 mg/dl, usually on postoperative day 2. CMV prophylaxis was achieved in 5 patients (38.46 %) who were donor-positive/recipient-negative for CMV. The mean postoperative serum creatinine at discharge from PICU - 0.59 mg/dl (range, 0.27 - 1.27) significantly decreased when compared to the mean preoperative serum creatinine value - 6.45 mg/dl (range, 1.90 – 12.26). Two patients (15.38 %) were transfused with 1 unit of PRBC postoperatively due to postoperative anemia (Table 5).
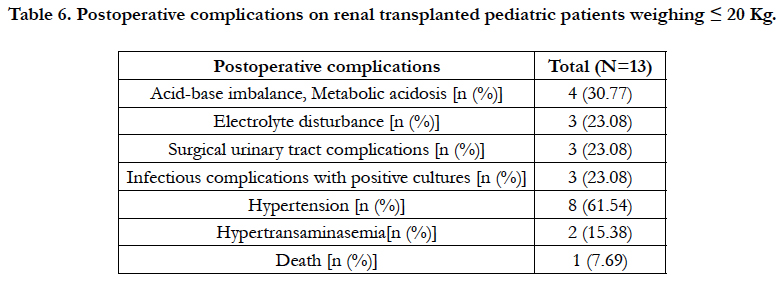
Table 6. Postoperative complications on renal transplanted pediatric patients weighing ≤ 20 Kg.
During the immediate postoperative period, 4 patients (30.77 %) developed metabolic acidosis and 3 patients (23.08 %) developed electrolyte disturbances: hyperkalemia, hypokalemia, hypophosphatemia, and hypomagnesemia. Surgical urinary tract complications were reported on 3 patients (23.08%):a) ureteral obstruction and vesical leak with subsequent nephrostomy and perivesical drainage, b) bladder suture dehiscence, and c) vesical clot with subsequent clot extraction. Infections with positive cultures were reported for 3 patients (23.08 %). Hypertension was present in 8 patients (61.54 %) postoperatively and hypertransaminasemia 2 patients (15.38 %) (Table 6).
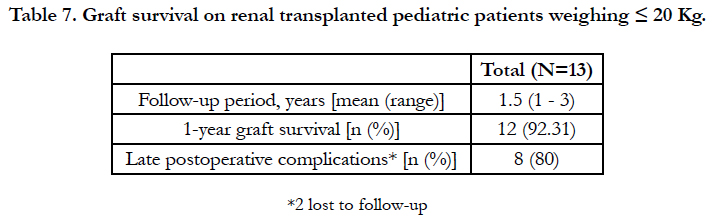
Table 7. Graft survival on renal transplanted pediatric patients weighing ≤ 20 Kg.
Death occurred in 1 patient (7.69%), who had a history of hemolytic uremic syndrome and mild mitral insufficiency. Postoperatively, the patient developed peritonitis for P. Aeruginosa and P. Mirabilis with subsequent sepsis for P. Putida. A massive bilateral intra-alveolar pulmonary hemorrhage and thrombotic microangiopathic glomerulopathy in 30% of the glomeruli led to multiple organ failure 16 days after transplantation (Table 6 and Table 8).
The mean follow-up period was 1.5 year (range of 1 - 3) with 12 patients out of 13 (92.31 %) presenting with 1-year graft survival (Table 7). After the 1 year follow-up, 2 patients (15.38%) continued their post-transplant follow-ups at a different medical center and late postoperative complications were not recorded. Late infections (after 1 year post-transplant) were diagnosed in 8 patients (80 %) out of the remaining 10 patients available for follow-up (Table 8).
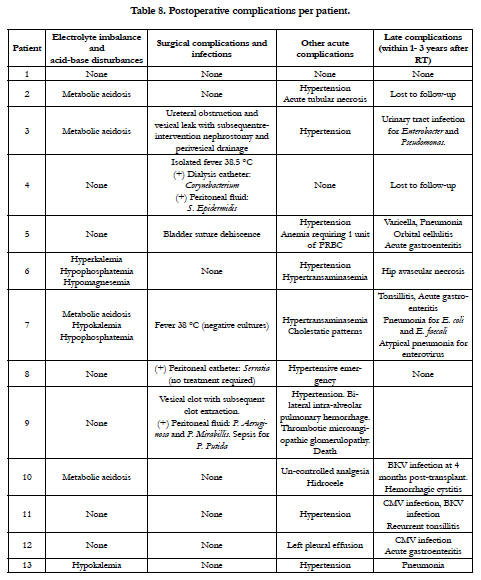
Table 8. Postoperative complications per patient.
Discussion
Worldwide, the incidence of CKD is reported to be approximately 18.5 - 58.3 per million children [10]. The most common etiologies of renal failure in pediatric populations are congenital disorders (eg. renal dysplasia, obstructive uropathy or reflux nephropathy in adolescents) and glomerular diseases (eg. focal segmental or lupus nephritis in older children) [11]. Congenital disease was the most common cause of CKD in our study population (76.92 %). RT has become the treatment of choice for pediatric patients with chronic renal conditions [1]. A multidisciplinary intervention during each operative stage (preoperative, intraoperative and postoperative) is essential to achieve a successful transplantation.
A systematic and standardized approach to pre-transplant evaluation should be used. Nutritional status, electrolyte imbalances, hemodynamic status, immunizations, and additional evaluations can be added based on individual patient needs.
Proper nutrition is essential for age related growth and neurological development of children undergoing RT with favorable long-term outcome [12]. According to Spanish Pediatric Registry of Terminal Renal Insufficiency II (“REPIR II” for its acronym in Spanish) in 2008, 7% of all children with CKD were malnourished, mostly patients younger than 2 years of age [13]. In the study population, the mean age was 4.46 years with a mean weight 17.15 kg. Based on current WHO weight-for-age and weight-forheight tables [14], 76.92 % of the children in the study had an adequate grow pattern according to their age, and 53.85% an adequate grow pattern according to their height. A total of 53.84% of our study population received nutrition via gastrostomy before RT for supplementary nutritional intake to achieve adequate growth.
Post-dialysis electrolyte status should be reviewed considering that hyperkalemia is a common finding involved in cardiac conduction abnormalities. If present, hyperkalemia should be corrected prior to induction of anesthesia [15]. Our data indicated that 2 out of 13 patients (15.38 %) presented hyperkalemia before RT. After calcium chloride administration, values returned to normal range.
Cardiology evaluation must be completed by echocardiography, pediatric patients with CKD frequently presenting a hyperdynamic circulatory state. Among other clinical entities, pericardial effusions, arrhythmias, hypertension, and cardiomyopathies are frequently diagnosed in this patient population [16, 17]. All our study patients were evaluated preoperatively with echocardiogram and 3 patients were found to have cardiomyopathy and/or valve defects.
To protect pediatric patients from preventable infectious diseases, multiple vaccines are required throughout their early childhood due to the immunosuppression during CKD and the future RT. For patients undergoing RT, it is recommended to administer all routine childhood vaccines in addition to pneumococcal and annual influenza vaccines (patients and family) prior to transplantation. Generally the immune response is suboptimal and close monitoring is required with antibody titer and booster. Live attenuated vaccines, such as measles, mumps, and rubella (MMR) and varicella, should be administer at least one month before the transplant. Approximately 6 months after the RT, vaccinationschedule may be followed normally, according to the age of the patient. Live attenuated vaccines should be avoided after RT [18]. Retrospectively, all of our study patients received appropriate scheduled immunization according to their age before RT. Only 1 out of 13 study patients presented varicella infection 1 year after transplant, confirming that the proposed immunization therapy used at our institution for RT patients is successful. The routine use of erythropoietin and the optimization of medical treatment reduces the incidence of anemia in CKD patients [19]. Only 2 of our study patients (15.38 %) presented with preoperative anemia requiring blood product administration intraoperatively.
The incision and approach to the recipient vessels is the surgeon’s choice and depend on each physician’s experience. Pararectal incision in the iliac fossa is the most commonly used approach [11]. In recipients weighing 15 kg or less, the incision can be extended to the costal margin (extraperitoneal) or even to a midline with transperitoneal access, preferred when large kidneys from an adult donor are transplanted. The extraperitoneal placement is preferable in patients who have been on peritoneal dialysis, because such dialysis can be continued after RT in case of delayed graft function [4]. Theoretically, the extraperitoneal position will facilitate future renal biopsies after the transplantation and prevent long-term complications such as obstructive intestinal adhesions, peritoneal infections, or intraperitoneal urinary leakage [20, 21].
For our study population, the transplanted kidney was placed in 12 patients (92.31%) extraperitoneally and in 1 patient (7.69%) transperitoneally.
In general, the largest and most suitable vessel of the recipient will be chosen for the anastomosis of the renal vessels to ensure a good blood flow and prevent incipient thrombosis. In children 15 kg or less, large vessels (aorta and the vena cava) are preferred for anastomosis. In older children, the iliac vessels are the choice for anastomosis [11]. Arterial kinking must be avoided and venous diameter must be wide enough to correspond recipient’s vessels [22]. In our study population, the external iliac vessels were used for anastomosis in 8 patients (61.54 %) and to other large vessels in 5 patients (38.46 %).
Fockens et al., advised to carefully perform the ureteral anastomosis to the bladder in order to avoid bleeding from the bladder or ureteral vessels and create clots into the fine urinary catheters with emergent re-intervention [23]. One of our study patients underwent re-intervention subsequent to ureteral stent obstruction and vesical leak.
A central venous catheter (CVC) to monitor CVP was used as routine monitoring. Invasive blood pressure monitoring is indicated for patients with low weight (<20 kg) or in patients with normal weight and serious cardiovascular disease or predictable cardiovascular instability (clamping of the aorta and/or vena cava). It is well known that this invasive technique does not exclude the risk of iatrogenic complications (high risk of vasospasm) in infants with low weight [24, 25]. For our study sample, CVP was monitored intraoperatively on 12 patients (92.31 %).
Pediatric patients are suitable candidates to be pre-medicated with midazolam. In elective cases, an inhalation induction can be performed. Intravenous induction is preferable [15] and in our study sample was achieved with propofol for 12 patients (92.31 %) and with etomidate for 1 patient (7.69 %). In CKD patients, it is essential to perform a proper reversal of neuromuscular blockade considering the reduced renal excretion of muscle relaxants [26-29]. Cisatracurium is the muscle relaxant drug of choice due to its Hofmann elimination. Rocuronium has a hepatic metabolism and hepatobiliary elimination. It can also be removed by renal excretion without being metabolized by up to 20% of its total. Its action may be prolonged in situations of hepatic and/or renal failure with an increased risk of developing postoperative residual curarization and respiratory complications. In this study sample, cisatracurium was the neuromuscular relaxant of choice in 69.23% of the patients, and rocuronium for the remaining 23.08 %.
The maintenance of anesthesia usually consists of an inhaled agent in combination with opioids. Nonsteroidal anti-inflammatory drugs (NSAIDS) are contraindicated at any time [6]. Epidural anesthesia in combination with general anesthesia is even more controversial in pediatric patients. This could be useful, as it provides hemodynamic stability and decreased postoperative pain. In any case, it would be limited to infants with higher weight than those included in our study [30]. Anesthesia maintenance in the study sample was performed for all patients with a combination of an inhaled agent (sevoflurane) and an opioid medication (fentanyl). No complementary regional techniques were used given the low weight of patients.
Fluid therapy should be guided by objectives and dynamic variables. In children below 20 kg, the maintenance of intravascular volume during surgery and in the immediate postoperative period is achieved using isotonic crystalloids, considering the metabolic acidosis present in many of these cases. Crystalloids containing potassium should be avoided [31]. Our study patients receivedcrystalloid sodium chloride at 0.9% for intraoperatively fluid management.
The new kidney requires a major proportion of the total intravascular volume of the recipient, and after unclamping the aorta, acute hypotension can occur affecting graft survival [11, 31]. During RT the adequate renal perfusion is achieved by maintaining the systolic blood pressure above 100 mmHg. Current clinical guidelines recommend that the CVP should be maintained in the range of 15-20 mmHg for children 5 years and younger, while older children could tolerate CVP values of 12-14 mmHg [7]. In this study sample, intraoperative hypotension was present in 7 patients (53.85%), with CVP values ranging from 4 mmHg to 9 mmHg.
The use of albumin solutions is suitable for the replacement of blood loss and/or volume prior to unclamping (within 30 minutes prior). Based on our retrospective data, albumin was used in 4 patients (30.77 %) who required fluid replacement intraoperatively. In the minutes before the arterial unclamping, diuretics such as furosemide and mannitol should be administrated. Our study patients received mannitol before unclamping; only mannitol has been proven to decrease the incidence of acute tubular necrosis and to improve early graft recovery [32].
The monitors for invasive continuous cardiac output such as Swan-Ganz or pulse contour cardiac output (PiCCO) system were not used in our study population since literature shows data obtained only from experimental animal models with limited evidence of adjustment for certain clinical values in pediatric patients. New pediatric cardiac monitoring studies are required in order to adjust the size of this devices and catheters to children’s use, and to avoid the high risk of iatrogenic complications [33-35].
In order to achieve good postoperative management, it is mandatory for our patients to be admitted into the PICU. Fluid therapy protocols, medications, and cardiovascular management are applied case by case in order to obtain an adequate capillary refill and optimal blood pressure for the immediate postoperative period [36]. The standardized goal in our critical care unit is to obtain a systolic blood pressure over 100 mmHg, with a CVP above 14 mmHg (or 10 cmH2O).
It has been shown that both hypovolemia and prolonged time of surgery are independent risk factors related to delay in graft function, and higher creatinine levels at 3 months, 6 months and 12 months [37]. Among our study patients, the mean creatinine decreased from 6.45 mg/dl preoperatively to 0.59 mg/dl after RT.
Fluid overload for adequate graft perfusion is accep[ed and can be reflected as moderate peripheral edema or some degree of acute pulmonary edema. One patient (7.69 %) from our study sample presented left pleural effusion postoperatively. Only unusual cases will require mechanical ventilation in the postoperative period [7].
Vasopressors might be required to maintain patients’ hemodynamic stability and homeostasis [11]. Dopamine use in RT has been clearly demonstrated to be more harmful than beneficialsince a denervated kidney is not expected to respond to its effect [38]. Continuous infusion of dopamine was used in 6 study patients (46.15 %) at a rate 3.5 - 5 mcg/kg/min intraoperatively and continued during PICU stay per clinical team decision. In contrast to literature reports, no complications related to dopamine use were documented in our study population.
Immunosuppression is highly individualized among different critical care units and different recipients based on each patients’ circumstances, graft compatibility and, whether or not they received previous immunization [39]. All study patients received preoperative and postoperative immunosuppression.
Late post-transplant infection is common, partly as a consequence of immunosuppression, but also transmitted through the transplanted organ. Since transplanted organs for pediatric patients usually come from adult donors, the possibility that the kidneys come from a seropositive donor (with latent virus such as CMV, EBV, BKV, among others) is increased [5]. Therefore, compared to adult recipients, children are at a relatively higher risk of developing infections with CMV, EBV or BKV, which are associated with higher rates of complications, graft loss, and death [9, 40, 41]. CMV prophylaxis was administered in 5 out of 13 study subjects, since they were identified as donor-positive/recipient-negative; nevertheless, 2 out of these 5 patients were diagnosed with CMV viral replication after RT. Our results correlate with previous evidence, reporting that patients receiving CMV positive organs developed CMV infection. If possible, CMV testing should be considered in donated organs in order to avoid viral replication in recipients. Most transplant centers provide prophylactic antibiotic therapy with broad-spectrum agents (cotrimoxazole) for several months. Ganciclovir is generally effective for both prophylaxis and treatment of CMV infection, associated with lower rates of lymphoproliferative disorders.
Urinary tract infections (UTI) are common, especially if the recipient has an underlying uropathy. An initial infection in immunosuppressed patients may result in a deposition of a latent virus in the urothelium and subsequent infections. Respiratory infections with opportunistic organisms such as Pneumocystis carinii are also common [43, 44]. In our study population, the following late complications (1 year post-RT) were identified:1 patient (7.69 %) was diagnosed with UTI, 3 patients (23.08 %) with pneumonia, and 2 patients (15.38 %) with BKV infection. The same type of late infections in our study population were mentioned by existing literature requiring multidisciplinary approach. BKV infection requires immunosuppression reduction and sometimes treatment with ciprofloxacin, intravenous immunoglobulin and/ or leflunomide [44-46].
Rodricks et al., reported 26.5 % vascular thrombosis complication in renal transplant pediatric patients [47]. Clinical manifestations include severe pain, acute graft rupture or massive bleeding. Although thrombosis can be an immediate event, it can also clinically manifest after several days as a result of organ dysfunction with decreased urine output, pain in the graft area, or fever [48]. In the study sample at our institution, none of our pediatric patients exhibited postoperative vascular thrombosis.
Thrombotic events may be a manifestation of an underlying prothrombotic condition, requiring an extended hematology investigation [49]. If thrombosis is suspected, Doppler ultrasound of renal vessels or a renogram should evaluate graft perfusion and during this interval the recipient might require a dialysis session. Unfortunately, only few arterial thromboses can be reversed with interventional radiology through stents and thrombectomy. A suspicion of an underlying arterial or venous suture stenosis points to urgent surgical revision [48]. If the delayed function persists, graft biopsies may be required to exclude the possibility of graft rejection. Most thrombosed grafts are removed in order to prevent infections or local calcifications [8, 50].
Other vascular complications requiring angioplasty include arterial stenosis or kinking and manifest with impaired renal function and hypertension. Hypertension is commonly present and treated in order to protect the graft [48]. In the early postoperative period, hypertension is allowed in order to provide adequate graft perfusion based on current guidelines (>90th percentile) [51]. Out of the 13 study patients, 8 patients (61.54 %) developed hypertension after RT.
Rossi et al., reports ureteral complications in 10% of RT patients. Urinary leakage may be an early manifestation, presenting as urine drainage through the wound or swelling/edema of the abdomen and genitals. This leakage compresses the venous drainage and compromises blood supply to the organ. Urinary drainage to the peritoneum may be undetected, especially during the recovery phase after a delayed graft function [52]. Surgical urinary tract complications were present in 3 patients (23.08 %) with only 1 patient (7.69%) requiring perivesical drainage insertion due to vesical leak.
Graft survival has significantly improved over time as shown in successive cohort studies conducted in pediatric recipients [53]. This progress can be attributed to many factors, such as improvements in the pre-transplant preparation, surgical techniques optimization, organ selection, more effective immunosuppressive drugs, advanced knowledge of pediatric pharmacokinetics, and use of evidence-based medicine protocols [5, 22]. Graft survival has significantly improved in kidneys transplanted to children less than 5 years of age [53-55]. In our cohort, 12 out of 13 patients (92.31 %) presented graft survival at 1 year follow-up from RT.
Conclusions
Our survival and transplant surgical outcomes in children with weight under 20 kilograms are similar to those reviewed in the literature. A multidisciplinary collaboration, including surgeons and anesthesiologists specialized in handling transplants for underweight children should be a priority. Nephrology optimization in the pre-operative and post-operative period plays a fundamental role in avoiding possible complications during surgery. Close intraoperative monitoring of vital signs and optimal fluid therapy is essential for anesthetic management due to the possible perioperative hemodynamic changes. Our study concluded that guidelines and clinical pathways are required in order to establish strategies for integrated action in the transplant center.
References
- Ruiz E, Ferraris J. 25 years of live related renal transplantation in children: The Buenos Aires experience. Indian J Urol. 2007 Oct;23(4):443-51. doi: 10.4103/0970-1591.36720. PubMed PMID: 19718302.
- Mickelson JJ, MacNeily AE, Leblanc J, White C, Gourlay WA. Renal transplantation in children 15 kg or less: the British Columbia Children’s Hospital experience. J Urol. 2006 Oct;176(4 Pt 2):1797-800. PubMed PMID: 16945652.
- Novljan G, Rus RR, Premru V, Ponikvar R, Battelino N. Chronic Hemodialysis in Small Children. Ther Apher Dial. 2016 Jun;20(3):302-7. doi: 10.1111/1744-9987.12441. PubMed PMID: 27312919.
- Butani L, Perez RV. Effect of pretransplant dialysis modality and duration on long-term outcomes of children receiving renal transplants. Transplantation. 2011 Feb 27;91(4):447-51. doi: 10.1097/TP.0b013e318204860b. PubMed PMID: 21131898.
- Rusai K, Szabo AJ. Recent developments in kidney transplantation in children. Curr Opin Organ Transplant. 2014 Aug;19(4):381-6. doi: 10.1097/ MOT.0000000000000102. PubMed PMID: 24991976.
- Ricaurte L, Vargas J, Lozano E, Díaz L; Organ Transplant Group. Anesthesia and kidney transplantation. Transplant Proc. 2013 May;45(4):1386-91. doi: 10.1016/j.transproceed.2012.12.014. PubMed PMID: 23726579.
- Aulakh NK, Garg K, Bose A, Aulakh BS, Chahal HS, Aulakh GS. Influence of hemodynamics and intra-operative hydration on biochemical outcome of renal transplant recipients. J Anaesthesiol Clin Pharmacol. 2015 Apr-Jun;31(2):174-9. doi: 10.4103/0970-9185.155144. PubMed PMID: 25948896.
- ElSheemy MS, Shouman AM, Shoukry AI, Soaida S, Salah DM, Yousef AM, et al. Surgical complications and graft function following live-donor extraperitoneal renal transplantation in children 20 kg or less. J Pediatr Urol. 2014 Aug;10(4):737-43. doi: 10.1016/j.jpurol.2013.12.013. PubMed PMID: 24495971.
- Andrews PA, Emery VC, Newstead C. Summary of the British Transplantation Society guidelines for the prevention and management of CMV disease after solid organ transplantation. Transplantation. 2011 Dec 15;92(11):1181-7. doi: 10.1097/TP.0b013e318235c7fc. PubMed PMID: 22002346.
- Collins AJ, Foley RN, Gilbertson DT, Chen SC. United States Renal Data System public health surveillance of chronic kidney disease and end-stage renal disease. Kidney Int Suppl (2011). 2015 Jun;5(1):2-7. PubMed PMID: 26097778.
- Williams A. Paediatric renal transplantation. Paediatrics and Child Health. 2012 Aug 1;22(8):346-50.
- Bertram JF, Goldstein SL, Pape L, Schaefer F, Shroff RC, Warady BA. Kidney disease in children: latest advances and remaining challenges. Nat Rev Nephrol. 2016 Mar;12(3):182-91. doi: 10.1038/nrneph.2015.219. PubMed PMID: 26831913.
- Areses Trapote R, Sanahuja Ibáñez MJ, Navarro M; Investigadores Centros Participantes en el REPIR II. Epidemiology of chronic kidney disease in Spanish pediatric population. REPIR II Project. Nefrologia. 2010;30(5):508-17. doi: 10.3265/Nefrologia.pre2010.May.10402. PubMed PMID: 20613854.
- World Health Organization. WHO child growth standards: length/height for age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age, methods and development. World Health Organization; 2006.
- Uejima T. Anesthetic management of the pediatric patient undergoing solid organ transplantation. Anesthesiol Clin North America. 2004 Dec;22(4):809-26. PubMed PMID: 15541937.
- O'Regan S, Matina D, Ducharme G, Davignon A. Echocardiographic assessment of cardiac function in children with chronic renal failure. Kidney Int Suppl. 1983 Nov;15:S77-82. PubMed PMID: 6584680.
- Bailey GL, Hampers CL, Hager EB, Merrill JP. Uremic pericarditis: clinical features and management. Circulation. 1968 Sep;38(3):582-91. PubMed PMID: 5673609.
- Danziger‐Isakov L, Kumar D, AST Infectious Diseases Community of Practice. Vaccination in solid organ transplantation. Am J Transplant. 2013 Mar;13 Suppl 4:311-7. doi: 10.1111/ajt.12122. PubMed PMID: 23465023.
- National Clinical Guideline Centre (UK). Anaemia Management in Chronic Kidney Disease: Partial Update 2015. London: Royal College of Physicians (UK); 2015 Jun. PubMed PMID: 26065064.
- Ranghino A, Segoloni GP, Lasaponara F, Biancone L. Lymphatic disorders after renal transplantation: new insights for an old complication. Clin Kidney J. 2015 Oct;8(5):615-22. doi: 10.1093/ckj/sfv064. PubMed PMID: 26413290.
- Heap SL, Webb NJ, Kirkman MA, Roberts D, Riad H. Extraperitoneal renal transplantation in small children results in a transient improvement in early graft function. Pediatr Transplant. 2011 Jun;15(4):362-6. doi: 10.1111/j.1399-3046.2011.01482.x. PubMed PMID: 21320247.
- Dharnidharka VR, Fiorina P, Harmon WE. Kidney transplantation in children. N Engl J Med. 2014 Aug 7;371(6):549-58.
- Fockens MM, Alberts VP, Bemelman FJ, Pes MP, Idu MM. Internal or external stenting of the ureterovesical anastomosis in renal transplantation. Urol Int. 2016;96(2):152-6. doi: 10.1159/000440702. PubMed PMID: 26535578.
- Sondergaard S, Parkin G, Aneman A. Central venous pressure: we need to bring clinical use into physiological context. Acta Anaesthesiol Scand. 2015 May;59(5):552-60. doi: 10.1111/aas.12490. PubMed PMID: 25684176.
- Michelet D, Brasher C, Marsac L, Zanoun N, Assefi M, Elghoneimi A, et al. Intraoperative hemodynamic factors predicting early postoperative renal function in pediatric kidney transplantation. Paediatr Anaesth. 2017 Sep;27(9):927-934. doi: 10.1111/pan.13201. PubMed PMID: 28736994.
- Carlos RV, Torres ML, de Boer HD. The use of rocuronium and sugammadex in paediatric renal transplantation: two case reports. Eur J Anaesthesiol. 2016 May;33(5):383-6. doi: 10.1097/EJA.0000000000000338. PubMed PMID: 26351827.
- Robertson EN, Driessen JJ, Booij LH. Pharmacokinetics and pharmacodynamics of rocuronium in patients with and without renal failure. Eur J Anaesthesiol. 2005 Jan;22(1):4-10. PubMed PMID: 15816565.
- Murphy GS, Szokol JW, Marymont JH, Greenberg SB, Avram MJ, Vender JS. Residual neuromuscular blockade and critical respiratory events in the postanesthesia care unit. Anesth Analg. 2008 Jul;107(1):130-7. doi: 10.1213/ane.0b013e31816d1268. PubMed PMID: 18635478.
- Srivastava A, Hunter JM. Reversal of neuromuscular block. Br J Anaesth. 2009 Jul;103(1):115-29. doi: 10.1093/bja/aep093. PubMed PMID: 19468024.
- Coupe N, O'brien M, Gibson P, De Lima J. Anesthesia for pediatric renal transplantation with and without epidural analgesia–a review of 7 years experience. Paediatr Anaesth. 2005 Mar;15(3):220-8. PubMed PMID: 15725320.
- Othman MM, Ismael AZ, Hammouda GE. The impact of timing of maximal crystalloid hydration on early graft function during kidney transplantation. Anesth Analg. 2010 May 1;110(5):1440-6. doi: 10.1213/ANE.0b013e3181d82ca8. PubMed PMID: 20418304.
- Andrews PM, Cooper M, Verbesey J, Ghasemian S, Rogalsky D, Moody P, et al. Mannitol infusion within 15 min of cross-clamp improves living donor kidney preservation. Transplantation. 2014 Oct 27;98(8):893-7. doi: 10.1097/TP.0000000000000154. PubMed PMID: 24831920.
- Ballestero Y, Urbano J, López-Herce J, Solana MJ, Botrán M, Vinciguerra D, et al. Pulmonary arterial thermodilution, femoral arterial thermodilution and bioreactance cardiac output monitoring in a pediatric hemorrhagic hypovolemic shock model. Resuscitation. 2012 Jan;83(1):125-9. doi: 10.1016/j.resuscitation.2011.06.039. PubMed PMID: 21763249.
- Torgay A, Pirat A, Akpek E, Zeyneloglu P, Arslan G, Haberal M. Pulse contour cardiac output system use in pediatric orthotopic liver transplantation: Preliminary report of nine patients. Transplant Proc. 2005 Sep;37(7):3168-70. PubMed PMID: 16213339.
- Saugel B, Holzapfel K, Stollfuss J, Schuster T, Phillip V, Schultheiss C, et al. Computed tomography to estimate cardiac preload and extravascular lung water. A retrospective analysis in critically ill patients. Scand J Trauma Resusc Emerg Med. 2011 May 23;19:31. doi: 10.1186/1757-7241-19-31. PubMed PMID: 21605380.
- Van Arendonk KJ, Boyarsky BJ, Orandi BJ, James NT, Smith JM, Colombani PM, et al. National trends over 25 years in pediatric kidney transplant outcomes. Pediatrics. 2014 Apr;133(4):594-601. doi: 10.1542/peds.2013- 2775. PubMed PMID: 24616363.
- Tugmen C, Sert I, Kebabcı E, Murat Dogan S, Tanrısev M, Alparslan C, et al. Delayed graft function in kidney transplantation: Risk factors and impact on early graft function. Prog Transplant. 2016 Jun;26(2):172-7. doi: 10.1177/1526924816640978. PubMed PMID: 27207406.
- Kadieva VS, Friedman L, Margolius LP, Jackson SA, Morrell DF. The effect of dopamine on graft function in patients undergoing renal transplantation. Anesth Analg. 1993 Feb;76(2):362-5. PubMed PMID: 8424517.
- Dobbels F, Ruppar T, De Geest S, Decorte A, Van Damme‐Lombaerts R, Fine RN. Adherence to the immunosuppressive regimen in pediatric kidney transplant recipients: a systematic review. Pediatr Transplant. 2010 Aug;14(5):603-13. doi: 10.1111/j.1399-3046.2010.01299.x. PubMed PMID: 20214741.
- Chaudhuri A, Ozawa M, Everly MJ, Ettenger R, Dharnidharka V, Benfield M, Mathias R, Portale A, McDonald R, Harmon W, Kershaw D. The clinical impact of humoral immunity in pediatric renal transplantation. J Am Soc Nephrol. 2013 Mar;24(4):655-64. doi: 10.1681/ASN.2012070663. PubMed PMID: 23449533.
- Ginevri F, Nocera A, Comoli P, Innocente A, Cioni M, Parodi A, et al. Posttransplant de novo donor‐specific HLA antibodies identify pediatric kidney recipients at risk for late antibody‐mediated rejection. Am J Transplant. 2012 Dec;12(12):3355-62. doi: 10.1111/j.1600-6143.2012.04251.x. PubMed PMID: 22959074.
- Gupta RK, Jain M, Garg R. Pneumocystis carinii pneumonia after renal transplantation. Indian J Pathol Microbiol. 2004 Oct;47(4):474-6. PubMed PMID: 16295369.
- Di Cocco P, Orlando G, Mazzotta C, Rizza V, D'Angelo M, Clemente K, et al. Incidence of urinary tract infections caused by germs resistant to antibiotics commonly used after renal transplantation. Transplant Proc. 2008 Jul-Aug;40(6):1881-4. doi: 10.1016/j.transproceed.2008.05.014. PubMed PMID: 18675078.
- Santoveña AZ, Meseguer CG, Mejía SM, Melgar ÁA, Camblor CF, Hijosa MM, et al. BK virus infection in pediatric renal transplantation. Transplant Proc. 2015 Jan-Feb;47(1):62-6. doi: 10.1016/j.transproceed.2014.11.020. PubMed PMID: 25645771.
- Dixon SB, Lane A, O'brien MM, Burns KC, Mangino JL, Breese EH, et al. Viral surveillance using PCR during treatment of AML and ALL. Pediatr Blood Cancer. 2018 Jan;65(1). doi: 10.1002/pbc.26752. PubMed PMID: 28792686.
- Ng JC, Leung M, Wright AJ, Ensom MH. Clinical Pharmacokinetic Monitoring of Leflunomide in Renal Transplant Recipients with BK Virus Reactivation: A Review of the Literature. Clin Pharmacokinet. 2017 Sep;56(9):1015-1031. doi: 10.1007/s40262-017-0521-9. PubMed PMID: 28247238.
- Rodricks N, Chanchlani R, Banh T, Borges K, Vasilevska‐Ristovska J, Hebert D, et al. Incidence and risk factors of early surgical complications in young renal transplant recipients: A persistent challenge. Pediatr Transplant. 2017 Nov;21(7). doi: 10.1111/petr.13006. PubMed PMID: 28670838.
- Ammi M, Daligault M, Sayegh J, Abraham P, Papon X, Enon B, et al. Evaluation of the vascular surgical complications of renal transplantation. Ann Vasc Surg. 2016 May;33:23-30. doi: 10.1016/j.avsg.2016.03.002. PubMed PMID: 26995525.
- Dimitroulis D, Bokos J, Zavos G, Nikiteas N, Karidis NP, Katsaronis P, et al. Vascular complications in renal transplantation: a single-center experience in 1367 renal transplantations and review of the literature. Transplant Proc. 2009 Jun;41(5):1609-14. doi: 10.1016/j.transproceed.2009.02.077. PubMed PMID: 19545690.
- Nixon JN, Biyyam DR, Stanescu L, Phillips GS, Finn LS, Parisi MT. Imaging of pediatric renal transplants and their complications: a pictorial review. Radiographics. 2013 Sep-Oct;33(5):1227-51. doi: 10.1148/rg.335125150. PubMed PMID: 24025922.
- Hooper DK, Mitsnefes M. A systems-based approach to managing blood pressure in children following kidney transplantation. Pediatr Nephrol. 2016 Oct;31(10):1593-604. doi: 10.1007/s00467-015-3192-5. PubMed PMID: 26482251.
- Rossi V, Torino G, Gerocarni Nappo S, Mele E, Innocenzi M, Mattioli G, et al. Urological complications following kidney transplantation in pediatric age: A single‐center experience. Pediatr Transplant. 2016 Jun;20(4):485-91. doi: 10.1111/petr.12691. PubMed PMID: 26893216.
- Smith JM, Martz K, Blydt‐Hansen TD. Pediatric kidney transplant practice patterns and outcome benchmarks, 1987–2010: A report of the North American Pediatric Renal Trials and Collaborative Studies. Pediatr Transplant. 2013 Mar;17(2):149-57. doi: 10.1111/petr.12034. PubMed PMID: 23281637.
- Shen Q, Xu H, Fang XY, Liu HM, Zhai YH, Zhang X, et al. Clinical analysis of 39 cases who received transplantation of kidney from pediatric organ donors. Zhonghua Er Ke Za Zhi. 2016 Jul;54(7):531-5. doi: 10.3760/cma.j .issn.0578-1310.2016.07.013. PubMed PMID: 27412747.
- Sui M, Zhao W, Chen Y, Zhu F, Zhu Y, Zeng L, et al. Optimizing the utilization of kidneys from small pediatric deceased donors under 15 kg by choosing pediatric recipients. Pediatr Transplant. 2016 Feb;20(1):39-43. doi: 10.1111/petr.12645. PubMed PMID: 26616462.





