Patient Transfer Unit: Clinical Experience On Medical Evacuation In North-East
AB Tiwari1*, H N Madhusudana2, GS Basra2, GS Sandhu VSM3
1 Senior Advisor (Anaesthesiology), Air Force Hospital, Kanpur, India.
2 Classified Specialist (Anaesthesiology), Air Force Hospital, India.
3 Air Vice Marshal, PMO HQ (MC).
*Corresponding Author
GpCapt(Dr) AB Tiwari,
Senior Advisor (Anaesthesiology) 7 Air Force Hospital, Kanpur, 208004, India.
Tel: +919451614124
E-mail: dr.abtiwari@gmail.com
Received: October 08, 2018; Accepted: October 26, 2018; Published: October 29, 2018
Citation: AB Tiwari, H N Madhusudana, GS Basra, GS Sandhu VSM. Patient Transfer Unit: Clinical Experience On Medical Evacuation In North-East. Int J Anesth Res. 2018;6(7):537-542. doi: dx.doi.org/10.19070/2332-2780-18000108
Copyright: AB Tiwari© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Patient Transport unit (PTU) and its team CCATT (Critical Care Air transport Team) has been operating as a savior of north-east since 2008. It is an indigenously developed, stretcher modified unit. It houses the essential critical monitoring and electromedical life support electromedical equipment. The inhospitable terrain of north-eastern sector coupled with ‘the need for speed’ makes aeromedical retrievals (MEDEVAC) an essential and very often the only choice. There has been a significant number of MEDEVAC using this equipment and the experience gained over the year has caused several modifications in its basic design as well as opened a chapter for light weight mobile PTU i.e. Backpack PTU. There has been issues pertaining to its use in terms of criticality of patient, hours of its use on long term flying, on board interventions, communication related events, operational and administrative support. To utilize it judicially and gainfully it was proposed to study all the related aspects and formulate a severity screening scoring system so that the indenting, administrative and delivering units are on same platform.
2.Abbreviations
3.Introduction
4.Study Design
5.Material and Method
6.Observation
6.1 Mission MEDEVAC
6.2 Reason for MEDEVAC
6.3 Destination MEDEVAC
6.4 On board Intervention
6.5 Flying Time
7.Discussion
7.1 Administrative
7.2 Action by Indenting Unit
7.3 Communication Requirement
8.Conclusion
9.References
Keywords
Patient Transport Unit (PTU); Critical Care Air Transport Team (CCATT); CASEVAC; MEDEVAC; Life Support Trauma and Transport (Trolley); Portable Lab Analyser (i-STAT).C.
Abbreviations
PTU: Patient Transport Unit; CCATT: Critical Care Air Transport Team; LSTAT: Life Support Trauma and Transport.
Introduction
The history of aeromedical evacuation is closely associated with the beginning of manned aviation. Its origins are credited to the Chief of Dutch medical service M. De Mooy (“the Jules Verne of air-ambulance service”) in 1910, who was the first to, conceptualize the air transport of wounded patients [1]. Air transport of wounded patients in hot-air balloons is a military anecdote, as there is no historical evidence for it. First documentary evidence for deployment and established an aircraft ambulance goes to France for the transport of wounded patients in the First World War (The familiar concept of triage, from the French ‘‘trier’’, to sort) [2]. By Second Word War, organized air transport of wounded patients was established in the military.
From 2003 to August 2006 the US Air Force evacuated a total of 37,000 patients from Southwest Asia using MEDEVAC. Approximately up to 500 of these casualties were treated by CCATT´s [3]. In flight critical care has enabled movement of trauma patients over long distances to reach definitive care within hours of injury.
The Safe transport of the critically ill patient requires accurate assessment and stabilisation of the patient before transport. There should be appropriate planning of transport and optimum utilisation of communications. Safe transport requires the deployment of appropriately trained staff with essential equipment, and effective liaison between referring, transporting and receiving staff at a senior level.
On 22 Dec 2007, 5 Air Force Hospital, proposed to establish a critical care air transport team (CCATT) to optimally utilise the expertise and knowledge of medical officers of the IAF (Care Givers in the sky). On 18 Apr 2008, first CCATT air transport was a case of spinal injury and since then there has been a generation change in structure and composition of the PTU. Today we have successfully evacuated a total 132 cases.
The analysis of different aspect of evacuation since indenting till return of CCATT back home has revealed several issues. These need to be addressed to provide a guideline for safe and efficient MEDEVAC and optimal utilization of resources.
Study Design
The study is designed to compile and analyse the data collected over since the first Medevac. The post CCATT feedback is the basis of this study, which is elaborate and includes every details of incidence since indenting, emplaning, on board activities and deplaning.
Material and Method
The material is the data base compiled over year and the scientific analysis of every bits of information including the positive and negative feedback endorsed by the CCATT members in their post-mission report.
Since the first mission on 07 Apr 2008 till date there have been 88 CCATT missions including Backpack PTU and a total of 132 cases of different severity have been evacuated. The cases were mostly from Army (90/132) (Table 1). The remaining were from Assam Rifle (21/132) and AF (15/132). Of the total, dependents evacuated (5/132), most were from the Air Force (4/5). These evacuations were accomplished by:
a. By PTU: (Figure 1)(Table 1).
b. By Mobile PTU: (Figure 2). A total of 03 poly trauma victims were evacuated using mobile PTU in 2012. All patients were stable. The reason for deployment was the availability of only Dornier Aircraft for the critical requirement of MEDEVAC. The constraints were in terms of limited space to house monitors, the casualties and the need to shift the equipment and Team members to the front of the aircraft both during takeoff and landing.
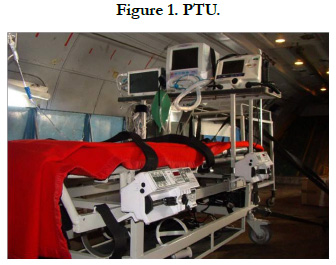



Table 1. Year Wise Medevac.


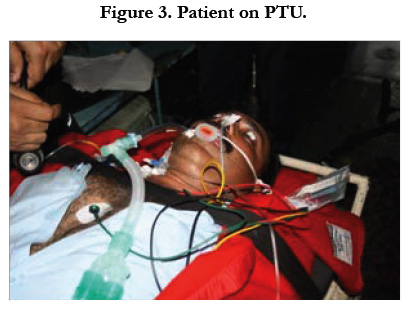
The reasons for evacuation of the cases were medical (80/132) and rest surgical cases (52/132) (Table 2). The medical cases were mostly Cardiac, Neurological, Sepsis and Hepatic failure, while surgical cases were mostly Poly Trauma, Head/intracranial Injury, Burn, Gun shot injury, Abdominal, Chest injury and Ac. Pancreatitis (Figure-3). Other reasons were Eclampsia with Hypertensive encephalopathy, Schizophrenia, Acute Lumbago, Bleeding per urethra, ECG abnormality, Haemoptysis (INV), Malignancies cases grouped under miscellaneous category. These cases did not require critical care monitoring or intervention but their evacuation had been asked for the reasons for CCATT tasking were mostly better facility and super specialist care at Tertiary care centres.
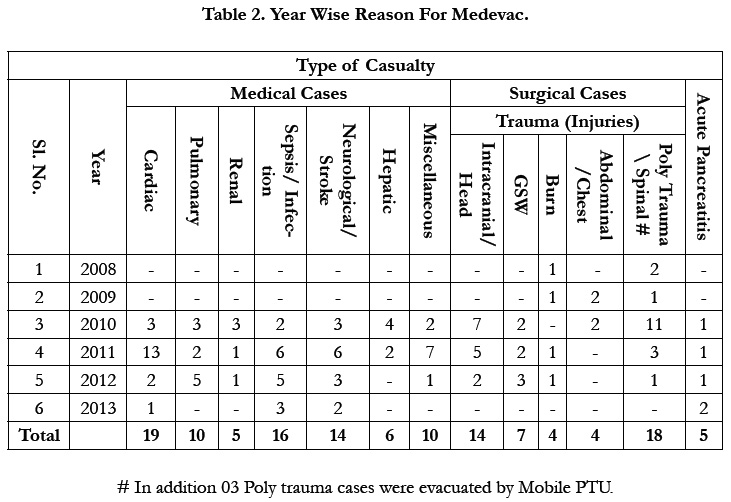
Table 2. Year Wise Reason For Medevac.

The MEDEVAC destination has been mostly CH(EC) Kolkata (121/132) and remaining to Army Hospital (Research and Referral) (02/132), CH(AF) Bangalore (01/132) and one case to Medical College, Guwahati (Table 3).
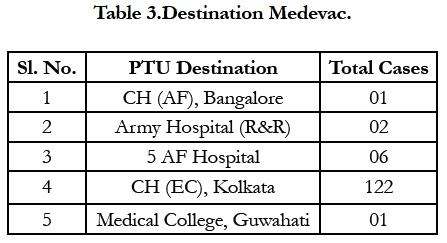
Table 3.Destination Medevac.
There has been minimal interventions on board in most of the cases. However on occasions, due to prolonged hours of flying and technical problem with ventilator the patients have been taken on Bain Circuit and ventilated manually. Inotrope support and sedation were titrated frequently. Endotracheal suctioning was required on board in some patient. The urobag and Chest drain checked. In one odd case ABG analysis and biochemical analysis were done. For patients on ventilator, ABG analysis was done before takeoff. None of the patient required intubation on board but few of them were on mechanical ventilation (Table 4). Intravenous lines do require change both at emplaning and on board. None of the patient so far has required Central line and chest tube placement, Invasive Pressure monitoring or Defibrillation on board. Though routine monitoring in terms of Pulse oximetry, ECG monitoring, Non-invasive BP monitoring was essentially carried out for every patient on PTU.


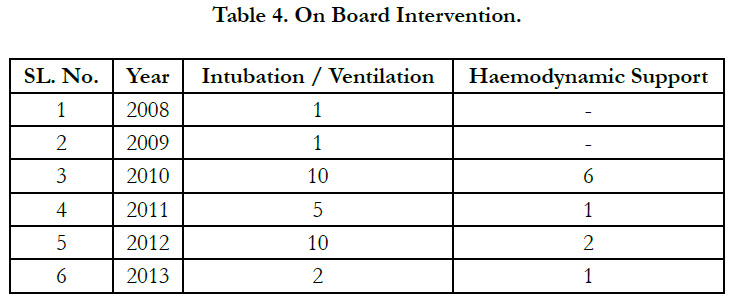
Table 4. On Board Intervention.
The CCATT move is a dedicated flight to destination. The precautions taken in situation of delayed takeoff were to keep the PTU plugged to SMC power supply at emplaning destination and load the PTU only when aircraft is ready to takeoff. The longest duration of flying has been to command hospital (AF), Bangalore, approximately 12hrs. with two refueling halts. The patient was on face mask and she was maintaining saturation. The second longest flying had been to Army Hospital (R&R), Delhi, 03hrs, this was nonstop and priority landing was accorded at air forcestation, Palam. The shortest time to destination has been to 5 AF Hospital, Jorhat and Medical College, Guwahati. (Approximately ½ hr. to 1hr.)
Discussion
The EMS guideline 2006 clearly dictates that Patients requiring critical interventions should be provided those interventions in the most expeditious manner possible, who are stable should be transported in a manner that best addresses the needs of the patient and the system. Patients with critical injuries or illnesses resulting in unstable vital signs require transport by the fastest available modality, and with a transport team that has the appropriate level of care capabilities, to a center capable of providing definitive care. Patients with critical injuries or illnesses should be transported by a team that can provide intra-transport critical care services. Those patients who require high-level care during transport, but do not have time-critical illness or injury, may be candidates for ground critical care transport.
The checklist for grading surgical severity are the parameters listed in different types of Trauma Scores. While the medical severity is evaluated by clinical and biochemical parameters. Royal Flying Doctor Services of Australia has provide a severity assessment criteria to prioritize the air evacuation (Table 5). A similar categorization has been followed by USAF, these categories have been defined in terms of time limits i.e. routine: within 72 h; priority: within 24 h; and urgent: immediately [5, 6].
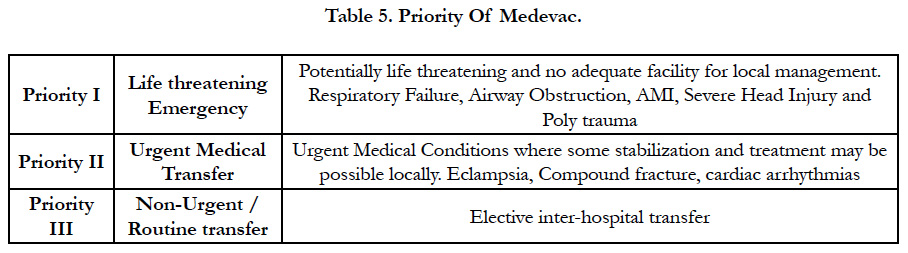
Table 5. Priority Of Medevac.
The Severity of the surgical and medical conditions itself dictate the criteria for MEDEVAC. The NATO lists out the following category of surgical and medical patients for MEDEVAC [7].
a. Surgical Conditions. Severe fractures, Spine injuries (paraplegia), Thorax trauma (instability, respiratory insufficiency), Open chest/abdominal injuries, Head Injury/ intracranial injury and Severe Blood loss.
b. Medical Conditions AMI, Pulmonary embolism, Acute cardiac insufficiency, Respiratory insufficiency, comas (metabolism) and Intoxications.
We have proposed the Severity assessment Scale as per Table-6 for ascertaining the requirement of CCATT for air evacuation. This information will also help in optimizing the composition of the CCATT.
The analysis of experience of deployment of the PTU has generated a number of issues which needs to be addressed. These issues are:
i. PTU demand has not been suitably justified and non-critical patients have been tasked for CASEVAC by CCATT. To obviate this a checklist has been proposed for severity scoring of the casualty to ascertain criticality of the patient and differentiate between routine / critical (Table - 6).
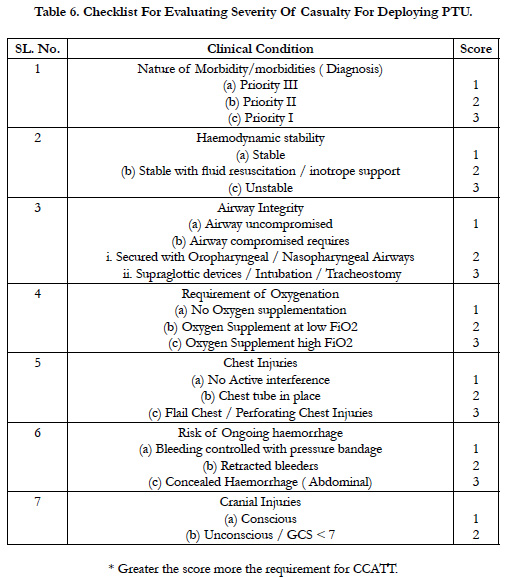
Table 6. Checklist For Evaluating Severity Of Casualty For Deploying PTU.
ii. Delays have been encountered in return of PTU from destination due to routing of aircraft to destination other than home base. Since PTU is the only medical facility in Armed Forces of its kind therefore priority should be given to its return movement.
iii. PTU has proved very useful in timely evacuation of critical casualties. Additional PTUs needs to be setup near Zonal hospitals in the Eastern sector to reduce response time.
iv. The resources on board have limited hours of battery life, therefore every priority should be given to avoid long refueling halts.
v. Provision for prepacked meal and preparation of movement order and manifest for the patient and CCATT members.
vi. AFMLUs should liaise with DGCA and CISF authority to avoid delay in transfer of casualties at civil airfields.
vii. Indenting unit needs to forward complete details and contact numbers of local liaison, who would be coordinating local administrative aspect at site of emplaning.
i. Assessment of casualty as per the checklist at Table-6 to assess criticality and need for CCATT or simple evacuation.
ii. Complete details of casualty to be forwarded to facilitate composition of CCATT and selection of on board medications to be carried and completion of preflight documentation and manifest.
iii. Timely transportation of casualty to emplaning unit and liaison with local SMO for medical support in case of delays.
iv. Lists of any additional routine transfer who wish to avail this mission to be intimated in advance for manifest and movement order purpose.
i. Provision for dedicated communication between CCATT and emplaning/receiving hospital. There is no compatibility between communication. At present we are relying on unsecure mobile communication with uncertain coverage.
Conclusion
The PTU is a step forward in the safe and speedy evacuation of casualties from remote geographical areas. The capability of onboard monitoring and cardiorespiratory support and intervention has permitted movement of casualties which could not be transported in earlier years.
The experience gained over the years can be utilized to overcome the limitations and short comings encountered and enhance professional and administrative capabilities of the unit. The objective would be to allow further interventions while airborne and ensure that all casualties can be safely transported to the appropriate Tertiary care facilities.
References
- Haller JS. Battlefield medicine: a history of the military ambulance from the Napoleonic Wars through World War I. SIU Press; 2011 Mar 29.
- Iserson KV, Moskop JC. Triage in medicine, part I: concept, history, and types. Ann Emerg Med. 2007 Mar;49(3):275-81. PubMed PMID: 17141139.
- Pierce PF, Evers KG. Global presence: USAF aeromedical evacuation and critical care air transport. Crit Care Nurs Clin North Am. 2003 Jun;15(2):221-31. PubMed PMID: 12755188.
- Transporting Your Patient Guidelines for Organizing and Preparing Patients for Transfer by Air. Royal Flying Doctor Service of Australia Western Operations. 2009. Version: 1.7.
- Command AM. Pamphlet 11–303. Access to the aeromedical evacuation system. Washington, DC: Department of the Air Force. 2000 Nov;3.
- Force UA. Instruction 41-307. Aeromedical evacuation patient considerations and standards of care. Washington, DC: Department of the Air Force. 2003 Aug;20.
- Erich Roedig, Brig. Gen. Ret. MD, CFS. Aeromedical Evacuation. 2006;157-06.





