Factors Impacting the Likelihood of Death in Patients in Intensive Care Unit
Saylan S1, Kostakoglu U2, Karatas M3, Yilmaz G4, Eroglu A1*
1 Karadeniz Technical University, Anesthesiology and Intensive Care Medicine, Trabzon, Turkey.
2 Kanuni Training Hospital, Infectious Disease, Trabzon, Turkey.
3 Kanuni Training Hospital Chest Disease, Trabzon, Turkey.
4 Karadeniz Technical University Infectious Disease, Trabzon, Turkey.
*Corresponding Author
Dr. Ahmet Eroglu,
Karadeniz Technical University,
Anesthesiology and Intensive Care Medicine, Trabzon, Turkey
E-mail: aheroglu@hotmail.com
Received: March 06, 2016; Accepted: April 11, 2016; Published: April 14, 2016
Citation: Eroglu A, et al. (2016) Factors Impacting the Likelihood of Death in Patients in Intensive Care Unit. Int J Anesth Res. 4(4), 225-228.DOI : dx.doi.org/10.19070/2332-2780-1600051
Copyright: Eroglu A© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background and Purpose: Intensive care units are special treatment units with high-tech equipment developed for the treatment and follow up of life-threatening organ failure seen in the course of both chronic and acute illnesses. These units have the highest mortality rates among hospital sections. To evaluate the factors affecting mortality in patients treated in ICUs and to determine the measures needed to reduce mortality rates.
Methods: This retrospective cohort study was performed using patient files, ICU records, infection control committee surveillance data and information processing data between 1 January - 31 December, 2013, at the Kanuni Education and Research Hospital.
Results: Average length of hospitalization was 17.3 ± 20.6 days. Mean Charlson co-morbidity index was 3.1 ± 1.8, and mean APACHE II score 19.7 ± 3.0. Four hundred ninety-seven patients (61.4%) died. The mortality rate was 23.7 per 1000 patient days. APACHE II score, the presence of nosocomial infections, and cerebrovascular disease were identified as independent risk factors affecting mortality in multivariable analysis. Mortality rate predicted by APACHE II score was 45.6%. The standardized mortality rate was 1.35. Hospitalization exceeded 48 hours in 566 patients, and 309 nosocomial infections developed in 205 of these. The nosocomial infection rate was 25.4 per 1000 patient days.
Conclusion: High APACHE II score, Charlson co-morbidity index and nosocomial infections are the most important factors affecting mortality.It is vitally important that infection should be prevented in to reduce mortality rates, and appropriate treatment should be initiated at once in the presence of infection. Therefore, in addition to the development of rapid diagnostic methods, training should be provided to increase hospital management and personnel awareness of the importance of the subject. Communication between units should be enhanced, and intensive care conditions and services should be improved.
2.Introduction
3.Material & Method
3.1.Statistical Analysis
4.Results
5.Discussion
6.Conclusion
7.Acknowledgements
8.References
Keywords
Intensive Care; Mortality; Infection.
Introduction
Intensive care units (ICUs) with technologically advanced equipment and 24-hour monitoring of vital signs aim to treat patients with a need for intensive care due to dysfunctions in one or more organs or organ systems [1, 2]. Patients hospitalized in these units often have multiple diseases, and acute problems associated with these need to be treated. High mortality rates are the most significant problem during this treatment in the ICU [2, 3]. Many factors, such as reasons for hospitalization in the ICU, invasive mechanical ventilation requirements, multiple organ dysfunction syndrome (MODS), higher acute physiology and chronic health evaluation (APACHE-II) score, hospital infections, trauma, old age, concomitant systemic diseases and length of stay in the ICU, all affect mortality [2, 3].
This study was intended to evaluate the factors affecting mortality in patients treated in ICUs and to determine the measures needing to be taken to reduce mortality rates.
Material & Method
This retrospective cohort study was performed at the Kanuni Education and Research Hospital adult ICUs (Anesthesia ICU, Internal Medicine ICU, Surgical ICU and Neurology ICU), which contain a total of 46 beds. ICU patient / nurse ratios range from 3/1 to 4/1 due to a shortage of nurses, and on some nights it may rise to 6/1. Age, sex, diagnosis on admission to the ICU and underlying disease, APACHE II score, Charlson co-morbidity index, duration of hospitalization, infections (pneumonia, surgical site infections, urinary tract infections, bloodstream infections, skin and soft tissue infections and other nosocomial infections), treatments, invasive procedures and prognosis of patients hospitalized in the ICUs between 1 January 2013 and 31 December 2013 were recorded. Charlson co-morbidity index scores represent the sum of the scores for patients’ comorbid diseases [4]. All data were obtained from patient files, nurses’ observations, infection control committee records, pharmacy data, treatment, surgical notes, and laboratory reports. All procedures performed for diagnosis and treatment were recorded. Diagnosis of nosocomial infections was based on Center for Disease Control (CDC) criteria [5]. The expected mortality rate was based on APACHE II scores. The standardized mortality ratio (SMO) [observed mortality ratio / mortality rate predicted by APACHE II scores] was calculated [6].
Factors that may influence mortality, such as age, sex, organ failure, malignancies, heart disease, diabetes mellitus, chronic obstructive pulmonary disease, trauma, APACHE II score, underlying disease, emergency and elective surgery, transfusion, prophylactic antibiotic use, invasive procedures, total parenteral nutrition and duration, steroid use and duration, other immunosuppressive use and duration thereof, indications and suitability of the antibiotics used, ICU nosocomial infections and associated factors, bacteremia, and presence of pneumonia were recorded. Their relations with mortality were then evaluated.
Statistical Analysis
Descriptive statistical analysis was performed for all parameters. The Kolmogorov-Smirnov test was used to determine the eligibility of variables. Data in conformity with normal distribution were analyzed using Student’s t-test, and those not conforming to normal distribution were analyzed using the Mann Whitney-U test. Data obtained by measurements were given as mean ± standard deviation. Data obtained by counting were given as numbers (%); analyses were performed using the Chi-square test. In addition, multivariate analyses were performed using logistic regression. The results of the analysis were presented as P values, odds ratio (OR), and 95% confidence interval (95% CI). P<0.05 was regarded as significant.
Results
Eight hundred ten patients, 443 male and 367 female, were admitted to the adult ICU units in our hospital in 2013. Mean age was 66.2 ± 15.9. Geriatric patients (> 65 years) represented 62.1%. Respiratory failure, hemodynamic instability, mental status disorder and monitoring needs were the most common indications for ICU admission.
Mean length of hospitalization was 17.3 ± 20.6 days. Mean Charlson co-morbidity index was 3.1 ± 1.8, and mean APACHE II score 19.7 ± 3.0. APACHE II score was 20 or more in 54.6% of patients. Eighty-eight percent of patients underwent urinary catheterization, 84% arterial catheterization, 74% mechanical ventilation, and 71% central venous catheterization. Thirty-seven percent of patients required vasopressors on admission to the ICU.
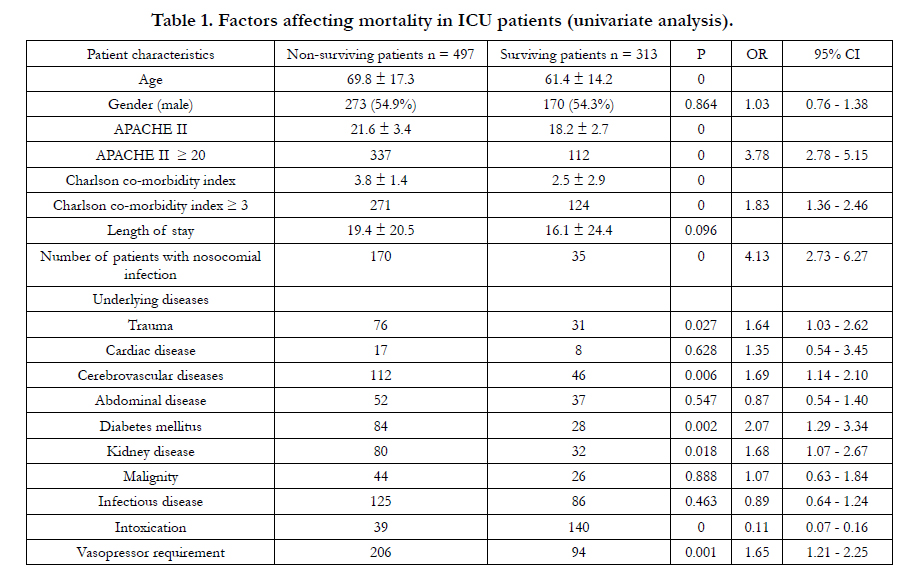
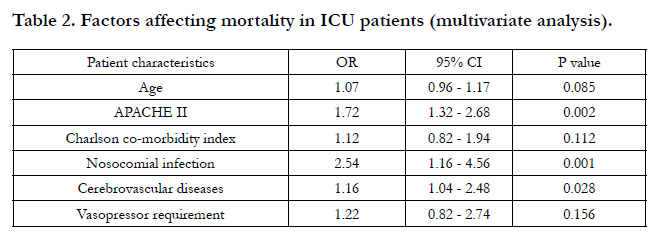
Four hundred ninety-seven patients (61.4%) died. The mortality rate was calculated at 23.7 per 1000 patient days. Age, high APACHE II score, presence of hospital infection, high Charlson co-morbidity index, trauma, cerebrovascular disease, diabetes mellitus, presence of renal failure, and vasopressor requirement were identified as factors affecting mortality (Table 1). At multivariable analysis, APACHE II score, the presence of nosocomial infections, and cerebrovascular disease were independent risk factors affecting mortality (Table 2). Mortality rate predicted by APACHE II score was 45.6%. Standardized mortality rate was 1.35, with 55.7% of deaths in the first 15 days and 19.5% after 30 days. Most patients (50.2%) who died in the first 15 days had trauma and cerebrovascular disease, while 46.4% of deaths after 30 days were due to infection.

Five hundred sixty-six patients were hospitalized for longer than 48 hours, and 309 nosocomial infections developed in 205 of these. Nosocomial infection rate was 25.4 per 1000 patient days, and 170 of patients diagnosed with such infection died. Mortality in 62 (12.5%) patients was attributed to infection. In 21 (33.9%) of these infections, patients had died by the time culture growth was notified. Seventeen patients (27.4%) had bacterial growth resistant to empirical treatment. Treatment started after 3.5 ± 1.1 days in 11 patients (17.7%). Mortality occurred in 13 (21%) patients despite appropriate treatment.
Discussion
ICUs are special treatment units with high-tech equipment developed for the treatment and follow up of life-threatening organ failure seen in the course of both chronic and acute illnesses [1, 7]. These units have the highest mortality rates among hospital sections [2, 3]. Many factors, including previous diseases and new developing events, determine the prognosis of patients monitored in these units. It is important for physicians dealing with intensive care to be aware of these factors and mortality rates, and to identify high-risk patients. Mortality analysis should therefore be performed in the ICU and for physicians’ benefit.
Mortality rates range between 16% and 71%, depending on the characteristics of the patients in the ICU [7-9]. In our study, the mortality rate was 61.4%. Patients admitted to ICUs have different characteristics, making it difficult to compare mortality rates. The standardized mortality rate is therefore recommended for comparing mortality rates between ICUs [6, 10]. One study compiling data from 12,162 patients treated in 24 ICUs in the UK reported mortality rates in different ICUs of 24-41%, with standardized mortality rates between 0.91 and 1.34 [11]. Metnitz et al. studied 13 ICUs and reported standardized mortality rates of between 0.62 and 1.54 [12]. In our study, the standardized mortality rate was 1.35. This result is greater than 1, which indicates that our intensive care performance is insufficient. This may be attributed to such negative factors as high numbers of patients per nurse in the ICU, lack of an isolation room, insufficient m2 per bed, and less than 2 meters’ distance between beds. This rate can be reduced by improving ICUs and the quality of service they provide.
Several studies have shown that high APACHE II scores are associated with mortality [13-15]. In our study, 48.7% of patients with APACHE II scores of 15-19 and 75.1% with APACHE II scores over 20 died. The risk of mortality was 3.78 times higher in patients with APACHE II scores over 20. At multivariable analysis, this score was identified as an independent risk factor for mortality. These results indicate that initial APACHE II scores are an important parameter determining prognosis on patients admitted to the ICU.
The Charlson co-morbidity index is another parameter that can be used in determining prognosis. Christensen et al. reported that the Charlson co-morbidity index can help predict both short- and long-term mortality in ICU patients [16]. We observed statistically significant differences in Charlson co-morbidity index scores between surviving and non-surviving patients. The risk of death was 1.83 times higher in patients with scores above 3. However, the Charslon co-morbidity index was not identified as an independent risk factor for mortality at multivariable analysis, because it was calculated as dependent on co-morbid disease.
Primary diseases of patients in the ICU, comorbid conditions and concomitant infections in hospital also affect mortality. Raffin identified hospital-acquired infections, arrhythmias, renal failure, liver failure, and heart failure as the major causes of mortality in the ICU [17]. In our study, the development of nosocomial infection increased mortality 4.13-fold. It was also identified as an independent risk factor for mortality at multivariable analysis. Mortality in 12.5% of fatal cases was attributed to nosocomial infections, which shows the importance of these infections. Late infection culture results in these infections and thus increased mortality as a result of delays in effective treatment reveal the need for rapid diagnostic methods.
Mortality increased 1.64 times in the presence of trauma, 1.62 times in respiratory failure, 1.69 times in cerebrovascular disease, 2.07 times in diabetes mellitus, and 1.68 times in kidney disease. The presence of cerebrovascular disease emerged as an independent risk factor for mortality. Vasopressor requirement increased mortality 1.65 times. One retrospective study of 61113 patients reported 31-day hospital mortality of 31.4%, with age, multiple organ failure, HIV infection, chronic liver disease and the presence of cancer being identified as independent factors associated with mortality at multivariate analysis [18]. Kollef et al. investigated 357 patients undergoing mechanical ventilation and identified female gender, advanced age, higher APACHE II scores, multiple organ failure and the presence of ARDS as independent factors affecting mortality [13]. Retainer et al. reported advanced age as an independent risk factor for mortality [19]. In our study, age affected mortality at univariate analysis, but was not an independent risk factor at multivariable analysis. The numerous comorbid diseases that can cause mortality in elderly patients suggest that mortality increases in line with high Charlson co-morbidity index and APACHE II scores.
Schönhof et al. reported that surviving patients had longer stays in ICUs compared with non-surviving patients, and also had lower APACHE II scores, lower mouth occlusion pressure and younger age [14]. Luh et al. investigated 1231 patients from 132 ICUs in Sweden, Iceland and Denmark, and reported a 90-day mortality rate of 41%. They identified advanced age, acute physiology scores above 15, extrapulmonary respiratory failure, pulmonary infiltration in more than two regions on and immunosuppression as independently increasing mortality [20].
Conclusion
In conclusion, high APACHE II and Charlson co-morbidity index scores are the most important factors affecting mortality. Another factor affecting mortality is nosocomial infection. It is vitally important that infection should be prevented in to reduce mortality rates, and appropriate treatment should be initiated at once in the presence of infection. Therefore, in addition to the development of rapid diagnostic methods, training should be provided to increase hospital management and personnel awareness of the importance of the subject. Communication between units should be enhanced, and intensive care conditions and services should be improved.
Acknowledgements
This study was performed at the Kanuni Training and Research Hospital following the approval from local ethical committee. We are grateful to all the ICU staff for their invaluable help and support.
References
- Halpern NA, Pastores SM, Greenstein RJ (2004) Critical care medicine in the United States 1985–2000: an analysis of bed numbers, use and costs. Crit Care Med 32(6): 1254-1259.
- Mayr VD, Dünser MW, Greil V, Jochberger S, Luckner G, Ulmer H, et al. (2006) Causes of death and determinants of outcome in critically ill patients. Crit Care 10(6): R154.
- Zeggwagh AA, Mouad H, Dendane T, Abidi K, Belayachi J, et al. (2014) Preventability of death in a medical intensive care unit at a university hospital in a developing country. Indian J Crit Care Med 18(2): 88-94.
- Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40(5): 373-383.
- Horan TC, Andrus M, Dudeck MA (2008) CDC/NHSN Surveillance definition of healthcare-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 36(5): 309-332.
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE (1985) APACHE II: A severity of disease classification system. Crit Care Med 13(10): 818-829.
- Hersch M, Izbicki G, Dahan D, Breuer GS, Nesher G, et al. (2012) Predictors of mortality of mechanically ventilated patients in internal medicine wards. J Crit Care 27(6): 694-701.
- Confalonieri M, Gorini M, Ambrosino N, Mollica C, Corrado A, et al. (2001) Respiratory intensive care units in Italy: a national census and prospective cohort study. Thorax 56(5): 373-378.
- Boussat S, El'rini T, Dubiez A, Depierre A, Barale F, et al. (2000) Predictive factors of death in primary lung cancer patients on admission to the intensive care unit. Intensive Care Med 26(12): 1811-1816.
- de Vos M, Graafmans W, Keesman E, Westert G, van der Voort PH (2007) Quality measurement at intensive care units: which indicators should we use? J Crit Care 22(4): 267-274.
- Goldhill DR, Sumner A (1998) Outcome of intensive care patients in a group of British intensive care units. Crit Care Med 26(8): 1337-1345.
- Metnitz PG, Lang T, Vesely H, Valentin A, Le Gall JR (2000) Ratios of observed to expected mortality are affected by differences in case mix and quality of care. Intensive Care Med 26(10): 1466-1472.
- Kollef MH, O’Brien JD, Silver P (1997) The impact of gender on outcome from mechanical ventilation. Chest 111(2): 434-441.
- Schönhofer B, Euteneuer S, Nava S, Suchi S, Köhler D (2002) Survival of mechanically ventilated patients admitted to a specialised weaning centre. Intensive Care Med 28(7): 908-916.
- Somme D, Maillet JM, Gisselbrecht M, Novara A, Ract C, et al. (2003) Critically ill old and the oldest-old patients in intensive care: short- and longterm outcomes. Intensive Care Med 29(12): 2137-2143.
- Christensen S, Johansen MB, Christiansen CF, Jensen R, Lemeshow S (2011) Comparison of Charlson comorbidity index with SAPS and APACHE scores for prediction of mortality following intensive care. Clin Epidemiol 3: 203-211.
- Raffin TA (1989) Intensive care unit survival of patients with systemic illness. Am Rev Respir Dis 140(2 Pt 2): S28-35.
- Behrendt CE (2000) Acute respiratory failure in the United States. Chest 118(4): 1100-1105.
- Retamar P, López-Prieto MD, Rodríguez-López F, de Cueto M, García MV, et al. (2014) Predictors of early mortality in very elderly patients with bacteremia: a prospective multicenter cohort. Int J Infect Dis 26: 83-87.
- Luhr OR, Antonsen K, Karlson M, Aardal S, Thorsteinsson A, et al. (1999) Incidence and mortality after acute respiratory failure and acute respiratory distress syndrome in Sweden, Denmark, and Iceland. The ARF Study Group. Am J Respir Crit Care Med 159(6): 1849-1861.





