Acute Respiratory Distress Syndrome, Short Review
Gutierrez WL1, Gutierrez SV2*
1 Anesthesiology and Intensive Care, Intensive Care Unit, Fundación Salud Bosque Bogotá D.C, Colombia.
2 Anesthesia Resident, Fundación Universitaria Sanitas, Anesthesia and Perioperative Medicine Bogotá D.C, Colombia.
*Corresponding Author
Sergio Esteban Gutiérrez Vidal,
Anesthesia Resident, Fundación Universitaria Sanitas,
Anesthesia and Perioperative Medicine Bogotá D.C, Colombia.
Tel: +571 4024886
E-mail: serguvi472@hotmail.com
Article Type: Case Report
Received: May15, 2015; Accepted: July 13, 2015; Published: July 15, 2015
Citation: Gutierrez WL, Gutierrez SV (2015) Acute Respiratory Distress Syndrome, Short Review. Int J Anesth Res. 3(6), 130-134. doi: dx.doi.org/10.19070/2332-2780-1500032
Copyright: Gutierrez SV© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Acute respiratory distress syndrome (ARDS) is a common syndrome in intensive care units, proper diagnosis and understanding of pathophysiology with the corresponding management positively affect the outcomes of patients with ARDS. The pathophysiology of ARDS is complex and involves a series of multiple biomolecular agents. There are multiple definitions of ARDS, the last assigned being the Berlin definition. There are some unknown aspects regarding ARDS that will be recognized within a few years of research. The purpose of this review is refresh some aspects as pathophysiology and classification about ARDS.
2.Introduction
3.Methods
4.Epidemiology
5.Pathophysiology ARDS
6.ARDS Definition
7.Treatment
8.Conclusions
9.References
Keywords
Respiratory Distress Syndrome; Adult; Pathophysiology; Definition; Treatment.
Introduction
Acute Distress respiratory syndrome (ARDS) is a frequent disease at intensive care unit (ICU), mostly secondary to sepsis. The syndrome it’s similar to other diseases in ICU, but the pathophysiology is different. The intensivist is responsible for a proper diagnosis, actually exist multiple definitions that are established, the objective of those definitions are maintain statistical data. ARDS is the worst manifestation secondary to pulmonary injury, after that a systemic reaction occurs that includes acute injury and systemic inflammation. ALI and ARDS must be considered as first manifestation in an infectious or inflammatory process. The lung is important in systemic injury because it receive all cardiac output and the incorrect function of the lung is clinically fast and relevant.
Methods
A non-systematic review was made upon a series of different articles, consulting sources regardless their publication date in PUBMED/ MEDLINE databases, Science Direct, OVID and complemented by articles referenced in the those articles. Keywords were used, such as: Respiratory distress syndrome, adult; physiopathology; definition, treatment. Both the search and selection of articles was made separately, not restricted to any publication.
Epidemiology
The incidence of ALI (acute lung injury) and ARDS has been difficult to calculate because there are not uniform definitions about them, as it varies according to its etiology and other demographic factors, on the other hand there’s lack of reporting and underdiagnoses. Goss et al. Working with NIH database, prospectively estimate an incidence of 64.2 cases per 100,000 persons-years [1]. Other reports as the one made by Rubenfeld calculate 78.9 per 100,000 persons-years. Predisposing factors include sepsis, pneumonia, pancreatitis, transfusion among others. In patients with alcohol abuse or chronic lung disease the risk is higher [2]. In 1980 the mortality rate was estimated approximately 64-70% [3-5], however, recent studies report a mortality risk of 29-42% [6,7]. Some studies estimate that the mortality rate varies according etiology, for instance. Sepsis mortality is 43%, pneumonia 36% and trauma 11% [8]. The first factor that reduces the risk of mortality is the use of protective lung ventilation, using fluids in a conservative way and other therapies that improve sepsis or other etiology.
Epidemiology
The incidence of ALI (acute lung injury) and ARDS has been difficult to calculate because there are not uniform definitions about them, as it varies according to its etiology and other demographic factors, on the other hand there’s lack of reporting and underdiagnoses. Goss et al. Working with NIH database, prospectively estimate an incidence of 64.2 cases per 100,000 persons-years [1]. Other reports as the one made by Rubenfeld calculate 78.9 per 100,000 persons-years. Predisposing factors include sepsis, pneumonia, pancreatitis, transfusion among others. In patients with alcohol abuse or chronic lung disease the risk is higher [2]. In 1980 the mortality rate was estimated approximately 64-70% [3- 5], however, recent studies report a mortality risk of 29-42% [6, 7]. Some studies estimate that the mortality rate varies according etiology, for instance. Sepsis mortality is 43%, pneumonia 36% and trauma 11% [8]. The first factor that reduces the risk of mortality is the use of protective lung ventilation, using fluids in a conservative way and other therapies that improve sepsis or other etiology.
Pathophysiology ARDS
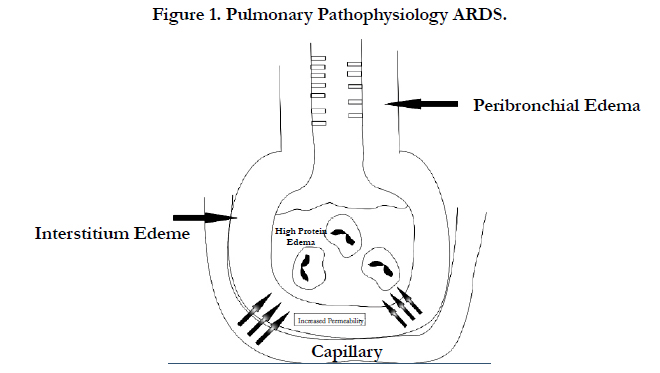
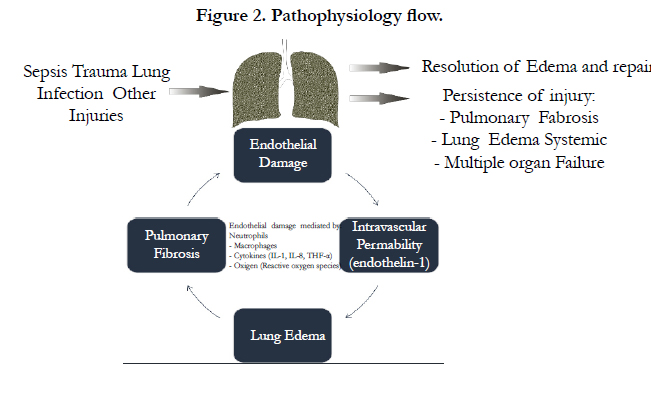
Ever since ARDS was defined, we continue defining the pathophysiology and the pathophysiological interaction mechanisms, acute or exudative initial phase is of quick onset and consists in dyspnea, hypoxemia, respiratory failure and pulmonary edema. The onset of respiratory failure requires mechanical ventilation and this respiratory failure is given by arterial hypoxemia associated with pulmonary edema due to filtration of proteins, decrease of compliance by alveolar edema and surfactant dysfunction, increase of dead space by injury or destruction of the microvascular bed [9, 10]. Increase of intra-abdominal pressure with decreased chest compliance, increases respiratory labor when ARDS causes are extra pulmonary [11]. Acute phase biopsy is infrequently used, in that biopsy findings are: edema, accumulation of neutrophils, monocytes, macrophages and erythrocytes in the alveolar space, alveolar epithelial damage and presence of microthrombies [12]. Endothelial damage leads to an increase in intravascular permeability, animal study showed formation of gap junctions [13] (Figure 1). Endothelial damage markers are mainly endothelin-1 [14] and VWF antigen [15]. Damage in this syndrome is mainly to alveoli type 1 (90%) and to a lesser extent, the cells type II (10%). The loss of epithelial integrity contributes to edema formation, and inadequate repair produces fibrosis. There is a critical role of neutrophils by which an increase of neutrophils in Bronchoalveolar lavage is observed [16], however, it can occur without the presence of neutrophils but it is rare [17], for neutrophils to generate damage, there must have molecular contact with mediators as I-CAM and CD11/CD18 [18], after that, a apoptosis process is generated with help of neutrophils and macrophages, the latter, prevent proteolytic enzyme activity, once activated, neutrophils can release proteolytic enzymes (elastases, collagenases, gelatinases A and B) which leads to an imbalance between proteases and antiproteases [19-21], neutrophils also release cytokines, reactive oxygen species and growth factors. Cytokines can deform the neutrophil and make it pass easily through the vascular bed. The main cytokines involved in this process are the TNF-α, IL-1, IL-8 (chemoattractant factor) [22-24] and IIL 10 and IL-11 [25, 26] interleukins acting as protectors. The reactive oxygen species are involved in this process also creating an imbalance between oxidants and antioxidants, reactive oxygen species increase the permeability of the cell membrane, oxidize proteins and DNA. The injuries may also be associated with mechanical ventilation since the volutrauma, barotrauma generate a proinflammatory cascade in which mainly metalloproteinases associate (Figure 2).
ARDS Definition
Although the beginning of the UCI was in the mid-50s in the United States, it was only until 1967 when this syndrome associated with septic patients was first defined. The person responsible for carrying out the definition at that time was Dr David Ashbaugh [27] with his workgroup. The definition was made thanks to the groups curiosity to find a similar syndrome to that seen in newborn infants called infant respiratory distress, that clinical condition consisted of tachypnea, dyspnea, cyanosis, hypoxemia, alveolar infiltrates.
The pathological definition of ARDS is given mainly by Katzenstein’s 1976 description as diffuse alveolar damage, among its features there are extensive lung density, interstitial and alveolar edema and hyaline membrane [28].
It wasn’t until 1988 when Murray [29] in an attempt to define more precisely, includes a series of variables focusing on risk factor, time in which the illness have presented and lung damage score. Murray’s scale also called LISS (Murray lung injury score system) includes 4 variables that include: number of blocks occupied in chest radiography, degree of hypoxemia measured by PaO2/FIO2, PEEP and pulmonary compliance. Although this scale is approved by some intensivists, it has the limitation that it has not been fully validated [30] and has a low specificity by failing to differentiate from other conditions such as cardiogenic pulmonary edema, diffuse alveolar hemorrhage, etc.
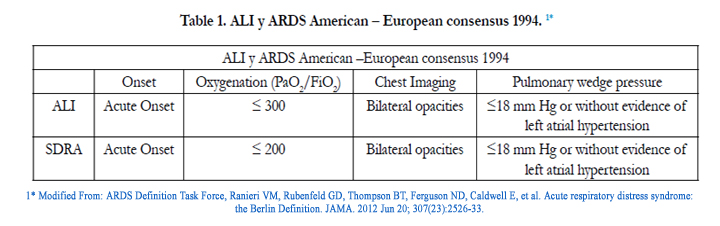
Later in 1994 there is a consensus that leads to a new definition of ARDS given by the conference of American-European consensus [31] whose purpose was to achieve a more specific definition and differentiate it from similar clinical conditions, this work could not be performed by Murray’s scale. This definition includes a series of criteria: 1. sudden onset of severe acute respiratory distress 2. Bilateral infiltrates on frontal chest radiography 3. Absence of left atrial hypertension (pulmonary wedge pressure below 18 mm Hg) or without signs of severe left ventricular failure 4. Severe hypoxemia determined by PaO2/FIO2 ≤ 200 mm Hg) (Table 1). In this definition, criteria was reserved according to its stage from moderate to severe, because the mild conditions were considered as ALI, this stage, unlike to ARDS, has PaO2/FIO2 values between 200-300 mm Hg.

After, Andres Esteban studies made in the Hospital of Getafe [32], demonstrated that there wasn’t a proper relationship between the syndrome’s anatomical-pathology and the definition given by the American-European consensus, for that reason the European society of intensive care, in its 2011 congress in the Berlin, provides a new definition of what is ARDS [33] (Table 2). The new definition had certain requirements such as feasibility, reliability and validity. In this new definition, the variables were: start time, thoracic imaging, origin of edema and hypoxemia given by a PaO2/FIO2 < 300 mm Hg with PEEP or CPAP > 5. Prior to the selection of these variables there were a series of variables they were not taken into account because they were clinically difficult to obtain in all cases, this include: plateau pressure, dead space measurement, lung water, evidence of inflammation, pulmonary shunt and chest CT images.
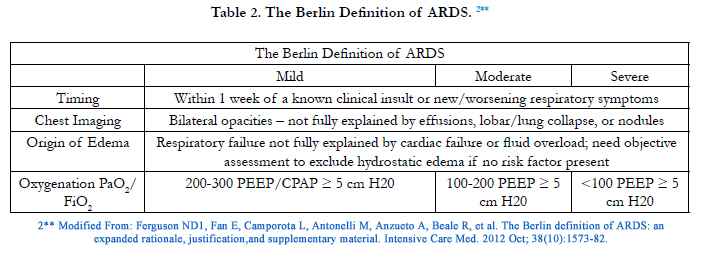
Among the new developments included in the new definition there are the elimination of acute and chronic concept, it eliminates the ALI concept, and it is replaced by mild ARDS, It is included in all severities to have the patient with PEEP ≥ 5. Expanding criteria obligation:
- Time must be sharp and be within 1 week after knowing the injury or respiratory symptoms.
- Chest image continues with the definition of bilateral infiltrates that are not explained by pleural effusion, lobar atelectasis or pulmonary lung nodules.
- Given the reduced use of pulmonary artery catheters, it was considered to remove pressure in pulmonary wedge definition, besides considering that a patient can coexist with cardiogenic edema plus ARDS
Berlin definition is based on a series of criteria and principles that the organization considered relevant to the development of the current definition, such as feasibility reliability, criterion validity, predictive validity, face validity, content validity.
Most ARDS are identified at 72 hours, clinically components of the syndrome are hypoxemia, TAC or RX bilateral opacities, pulmonary mix increase, dead space increase and reduce compliance.
The Berlin definition has a number of advantages such as allowing the coexistence of ARDS and cardiogenic pulmonary edema, it is at hand and defines temporality. The disadvantages of the Berlin definition are the exclusion of ALI from ARDS, the mild increase of area under the curve regarding the previous definition of the American-European Consensus (AECC) AUC 0.577 vs 0.536, It doesn’t use physiological variables, and needs further validation studies.
Phillips [34] in its editorial questioned whether the definition is just a superficial change. Other studies argue that 6.5% of patients with ALI / ARDS according to the AECC are not classified in ARDS according to the definition of Berlin by the fact that they have PEEP < 5 cm H20 [35] the panel of definition reports 12% [36], by definition moderate and severe ARDS are not with no-invasive ventilation (NIV), mortality at 28 days of mild and moderate ARDS is similar, and higher PEEP was not associated with higher survival.
Costa [37] considers that the new definition of Berlin for ARDS is useless and that it could have inserted more important variables and concepts such as pH, age, APACHE score, likewise, he questions the usefulness of thresholds Pa/Fi and believes that they are not important in diagnostics but that are useful in continuous monitoring, especially 24 hours after. He also argues that mild and severe ARDS are not different at the 0 hour in terms of mortality, but at 24 hours there is a significant difference between mild and severe ARDS and therefore considers that one of the thresholds is useless.
Also they consider lung compliance as a high predictor of mortality and considers it as a physiological variable of importance in the clinical condition.
Treatment
The panel that forms the definition suggests according to the severity of ARDS a specific treatment. The ventilatory management can be done invasively or non-invasively, you can use other kinds of techniques such as prone ventilation, nitric oxide, high frequency ventilation. Protective vents should be administered at 6 ml / kg, they have shown best results regarding ventilation with volumes of 12 ml/kg, with mortalities of 31 vs 40% respectively, statistically significant [38].
Given that ARDS is closely associated with severe sepsis in the field of ICU there should be an automatic management according to the isolated germ from blood cultures or identified in other crops, helped by vasopressor support. Conservative fluid management does not show improved mortality compared to liberal management, however, conservative management improves oxygenation and reduces duration of mechanical ventilation [39].
Numerous drugs have been used in clinical trials, exogenous surfactant, corticosteroids, ketoconazole, N-acetylcysteine among others. Some studies support the use of using β2 agonists, however others controvert it. They have also described the use of statins in their management with contradictory results [40, 41]. ARDS management must be integral, focusing on hemodynamic and ventilatory monitoring practice.
Conclusions
ARDS is a syndrome of multifactorial etiology of clinical importance in ICU, its pathophysiology involves processes of apoptosis and the role of neutrophils as triggers of the inflammatory process through interleukins leading to interstitial edema and in some cases fibrotic regeneration processes. The definition of ARDS since its beginning in 1967 has changed, the current definition is the Berlin, which is useful in the ICU but needs further validation and better variables that impact more clearly on morbidity and mortality in ICU patients. The understanding of the pathophysiology has allowed to have multiple therapeutic targets mainly focused on lung protection measures. There are many drugs in development to improve survival in patients with ARDS, we hope have more pathophysiologic knowledge in the incoming years.
References
- Rubenfeld GD, Caldwell E, Peabody E, Weaver J, Martin DP, et al. (2005) Incidence and outcomes of acute lung injury. N Engl J Med 353(16): 1685- 1693.
- Ware LB, Matthay MA (2000) The acute respiratory distress syndrome. N Engl J Med 342(18): 1334-1349.
- Villar J, Slutsky AS (1989) The incidence of the adult respiratory distress syndrome. Am Rev Respir Dis 140(3): 814-816.
- Fowler AA, Hamman RF, Good JT, Benson KN, Baird M, et al. (1983) Adult respiratory distress syndrome: risk with common predispositions. Ann Intern Med 98(5 Pt 1): 593-597.
- Milberg JA, Davis DR, Steinberg KP, Hudson LD (1995) Improved survival of patients with acute respiratory distress syndrome (ARDS): 1983–1993. JAMA 273(4): 306-309.
- Seeley E, McAuley DF, Eisner M, Miletin M, Matthay MA, et al. (2008) Predictors of mortality in acute lung injury during the era of lung protective ventilation. Thorax 63(11): 994-998.
- Zambon M, Vincent JL (2008) Mortality rates for patients with acute lung injury/ARDS have decreased over time. Chest 133(5): 1120-1127.
- Meade MO, Cook RJ, Guyatt GH, Groll R, Kachura JR, et al. (2000) Interobserver variation in interpreting chest radiographs for the diagnosis of acute respiratory distress syndrome. Am J Respir Crit Care Med 161(1): 85-90.
- Ware LB, Matthay MA (2005) Clinical practice. Acute pulmonary edema. N Engl J Med 353(26): 2788-2796.
- Prewitt RM, McCarthy J, Wood LDH (1981) Treatment of acute low pressure pulmonary edema in dogs: relative effects of hydrostatic and oncotic pressure, nitroprusside, and positive end-expiratory pressure. J Clin Invest 67(2): 409-418.
- Pelosi P, D’Onofrio D, Chiumello D, Paolo S, Chiara G, et al. (2003) Pulmonary and extrapulmonary acute respiratory distress syndrome are different. Eur Respir J Suppl 42: 48S-56S.
- Pratt PC, Vollmer RT, Shelburne JD, Crapo JD (1979) Pulmonary morphology in a multihospital collaborative extracorporeal membrane oxygenation project. Am J Pathol 95(1): 191-214.
- Hurley JV (1982) Types of pulmonary microvascular injury. Ann NY Acad Sci 384: 269-286.
- Fagan KA, McMurtry IF, Rodman DM (2001) Role of endothelin-1 in lung disease. Respir Res 2(2): 90-101.
- Ware LB, Conner ER, Matthay MA (2001) von Willebrand factor antigen is an independent marker of poor outcome in patients with early acute lung injury. Crit Care Med 29(12): 2325-2331.
- Steinberg KP, Milberg JA, Martin TR, Maunder RJ, Cockrill BA, et al. (1994) Evolution of bronchoalveolar cell populations in the adult respiratory distress syndrome. Am J Respir Crit Care Med 150(1): 113-122.
- Matthay MA (1999) Conference summary: acute lung injury. Chest 116(1 Suppl): 119S-126S.
- Doerschuk CM, Quinlan WM, Doyle NA, Bullard DC, Vestweber D, et al. (1996) The role of P-selectin and ICAM-1 in acute lung injury as determined using blocking antibodies and mutant mice. J Immunol 157(10):4609-4614.
- Donnelly SC, MacGregor I, Zamani A, Gordon MW, Robertson CE, et al. (1995) Plasma elastase levels and the development of the adult respiratory distress syndrome. Am J Respir Crit Care Med 151(15): 1428-1433.
- Gando S, Kameue T, Nanzaki S, Hayakawa T, Nakanishi Y (1997) Increased neutrophil elastase, persistent intravascular coagulation, and decreased fibrinolytic activity in patients with posttraumatic acute respiratory distress syndrome. J Trauma 42(6): 1068-1072.
- Christner P, Fein AM, Goldberg S, Lippmann M, Abrams W, et al. (1985) Collagenase in the lower respiratory tract of patients with adult respiratory distress syndrome. Am Rev Respir Dis 131(5): 690-695.
- Goodman R, Pugin J, Lee JS, Matthay MA (2003) Cytokine mediated inflammation in acute lung injury. Cytokine Growth Factor Rev 14(6): 523-535.
- Nathan CF (1987) Secretory products of macrophages. J Clin Invest 79(2): 319-326.
- Miller EJ, Cohen AB, Matthay MA (1996) Increased interleukin-8 concentrations in the pulmonary edema fluid of patients with acute respiratory distress syndrome from sepsis. Crit Care Med 24(9): 1448-1454.
- Parsons PE (1998) Interleukin-10: the ambiguity in sepsis continues. Crit Care Med 26(5): 818-819.
- Kurdowska A, Noble JM, Steinberg KP, Ruzinski JT, Hudson LD, et al. (2001) Anti-interleukin 8 autoantibody: interleukin 8 complexes in the acute respiratory distress syndrome. Am J Respir Crit Care Med 163(2):463-468.
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE (1967) Acute respiratory distress in adults. Lancet 2(7511): 319-323.
- Katzenstein AL, Bloor CM, Leibow AA (1976) Diffuse alveolar damage— the role of oxygen, shock, and related factors. A review. Am J Pathol 85(1): 209-228.
- Murray JF, Matthay MA, Luce JM, Flick MR (1988) An expanded definition of the adult respiratory distress syndrome. Am Rev Respir Dis 138(3): 720-723.
- Villar J, Blanco J, Kacmarek RM (2011) Acute respiratory distress syndrome definition: do we need a change? Curr Opin Crit Care 17(1): 13-17.
- Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, et al. (1994) The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 149(3 Pt 1): 818-824.
- Esteban A, Fernández-Segoviano P, Frutos-Vivar F, Aramburu JA, Nájera L, et al. (2004) Comparison of clinical criteria for the acute respiratory distress syndrome with autopsy findings. Ann Intern Med 141(6): 440-445.
- Ranieri VM, Rubenfeld GD, Thompson BT, Caldwell E, Fan E, et al. (2012) Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 307(23):2526-2533.
- Phillips CR (2013) The Berlin definition: real change or the emperor's new clothes? Crit Care 17(4):174.
- Hernu R, Wallet F, Thiollière F, Martin O, Richard JC, et al. (2013) An attempt to validate the modification of the American-European consensus definition of acute lung injury/acute respiratory distress syndrome by the Berlin definition in a university hospital. Intensive Care Med 39(12): 2161- 2170.
- Ferguson ND, Fan E, Camporota L, Antonelli M, Anzueto A, et al. (2012) The Berlin definition of ARDS: an expanded rationale, justification, and supplementary material. Intensive Care Med 38(10): 1573-1582.
- Costa EL, Amato MB (2013) The new definition for acute lung injury and acute respiratory distress syndrome: is there room for improvement? Curr Opin Crit Care 19(1): 16-23.
- Eisner MD, Thompson T, Hudson LD, Luce JM, Hayden D, et al. (2001) Efficacy of low tidal volume ventilation in patients with different clinical risk factors for acute lung injury and the acute respiratory distress syndrome. Am J Respir Crit Care Med 164(2): 231-236.
- Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, et al. (2006) Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 354(24): 2564–2575.
- Choi HS PM, Kang HM, Kim YJ, Choi CW, You JH, et al. (2008) Statin use in sepsis due to pneuomonia. Am J Respir Crit Care Med A580.
- Kor DJ, Iscimen R, Yilmaz M, Brown MJ, Brown DR, et al. (2009) Statin administration did not influence the progression of lung injury or associated organ failures in a cohort of patients with acute lung injury. Intensive Care Med 35(6): 1039–1046.
1* Modified From: ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012 Jun 20; 307(23):2526-33.
2**. Modified From: Ferguson ND1, Fan E, Camporota L, Antonelli M, Anzueto A, Beale R, et al. The Berlin definition of ARDS: an expanded rationale, justification,and supplementary material. Intensive Care Med. 2012 Oct; 38(10):1573-82.





