Management of Postoperative Bleeding after Minimally Invasive Mitral Valve Repair: A Case Report
Xin Yan Hu
Allegiance Health, Jackson MI, USA.
*Corresponding Author
Xin Yan Hu CRNA, MA, MSN,
Allegiance Health, 205 N East Ave,
Jackson, MI 49201, USA.
E-mail: kellyhuxinyan@yahoo.com
Article Type: Case Report
Received: March 04, 2015; Accepted: May 10, 2015; Published: May 12, 2015
Citation: Xin Yan Hu (2015) Management of Postoperative Bleeding after Minimally Invasive Mitral Valve Repair: A Case Report. Int J Anesth Res. 3(4), 101-104. doi: dx.doi.org/10.19070/2332-2780-1500026
Copyright: Xin Yan Hu© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Excessive postoperative bleeding after cardiac surgery is one of the major risk factors for increased morbidity and mortality. Effective and timely management is essential in averting the need for surgical re-exploration and preventing adverse outcomes. This case report describes the perioperative course of a patient undergoing minimally invasive mitral valve repair and the management of postoperative bleeding. The point of care testing technique of thromboelastography (TEG) is explored. Literature is reviewed for current evidence in treatment options for postoperative bleeding after cardiac surgery, including TEG-guided transfusion, fibrinogen replacement, activated Factor VII, antifibrinolytic agents, and DDAVP. The hemostatic management in the case report is then analyzed based on the current evidence.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.Acknowledgement
7.References
Keywords
Hemostasis; Thromboelastography; Fibrinogen; Platelets.
Introduction
Compared with conventional mitral valve surgery, minimally invasive mitral valve repair is associated with decreased postoperative pain, decreased blood product use, improved postoperative respiratory function, cosmetic advantage, and improved patient satisfaction [1, 2]. In a propensity-matched comparison, Atik et al., found that only 16 percent of patients who underwent minimally invasive mitral repair, in contrast to 50 percent of patients in the conventional mitral valve repair group, required red blood cell transfusion (p < .0001).
Excessive postoperative bleeding after cardiac surgery is associated with surgical re-exploration and increased postoperative stroke, prolonged intubation, prolonged ICU stay, and increased 30-day mortality [3]. Despite the decreased risk of bleeding compared with conventional mitral valve surgery, hemorrhage after minimally invasive surgery requires equally prompt and effective management to prevent postoperative complications. Important factors include deferential diagnosis of the causes of bleeding, timely testing, and appropriate interventions. This case report describes the perioperative course of a patient undergoing minimally invasive mitral valve repair and the management of postoperative bleeding. Discussions are based on the current evidence in testing techniques and treatment options for postoperative bleeding after cardiac surgery, including TEG-guided transfusion, fibrinogen replacement, activated Factor VII, antifibrinolytic agents, and DDAVP.
Case Report
A 61-year-old, 99.8kg female presented with Grade IV Mitral Regurgitation (MR) for minimally invasive mitral valve repair/replacement. Past medical history was significant for hypertension, obesity, myocardial infarction two years before, and MR present for the past two years. Past surgical history included childhood surgery for supernumerary kidney disease and total knee arthroplasty. Her home medications consisted of metoprolol, atorvastatin, lisinopril, and aspirin. The last dose of aspirin was taken two days prior to the surgery. A transthoracic echocardiogram demonstrated well-preserved left ventricular function, all heart valves free of lesion other than the mitral valve, an elevated pulmonary arterial pressure, and an elevated right ventricular systolic pressure. Electrocardiogram (ECG), carotid duplex, and the coagulation panel were normal and the platelet count was 172 x 109/L.
General anesthesia with a double-lumen tube was established uneventfully following administration of fentanyl, etomidate, and rocuronium. A radial arterial line and an intrajugular quadruplelumen central venous catheter were inserted. Epsilon aminocaproic acid (Amicar) 10grams bolus dose was administered, followed with 1g/hr of continuous infusion. Heparin 10,000 units were administered per surgeon request prior to femoral vein and
artery cannulation. During the left ventricular vent placement, the patient’s ECG converted from sinus rhythm to atrial fibrillation with a decompensating blood pressure despite vasopressor infusion. The team determined that immediate initiation of the cardiopulmonary bypass (CPB) was necessary. An additional 20,000 units of Heparin were administered. The post-heparin activated clotting time (ACT) was above 400 seconds and continued climbing when the CPB was established. The ACT continued to read up to 799 seconds, which gradually trended down to 468 seconds by the end of the 111-minute CPB period. Complex mitral valve repair was completed uneventfully. After the patient was successfully taken off CPB, protamine was administered at the dose of 1mg per 100 unit of heparin. Cell saver blood 500 ml was infused. The post-protamine ACT read 105 seconds. TEG showed R value 9.1 minutes, K 2.2 minutes, α angle 59.8 degrees, MA 56.8 mm and LY30 0.2%. The double-lumen tube was exchanged for a regular endotracheal tube. The patient remained stable with epicardial ventricular pacing at 72 beats/minute. The patient was transported to cardiovascular unit (CVU) with Amicar and propofol infusing.
Thirty minutes after the arrival in CVU, the chest tube system collected over 300ml of sanguineous drainage. The vital signs stayed stable with blood pressure in the low normal range. The platelet count was 92 x 109/L and activated partial thromboplastin time (APTT) was 33 seconds. Six units of pooled platelets were transfused and an additional 100mg of protamine was administered. The chest tube collection approximated 450ml by the end of the first hour but started to decline. The follow-up TEG showed R 7.8 minutes, K 2.8 minutes, α angle 45 degrees, MA 58.4mm, and LY30 0.0%. Postoperative hemoglobin and hematocrit were 10.1 g/dL and 29.1% respectively. Laboratory studies the following morning showed a platelet count of 123 x 109/L and a normalized coagulation panel. The chest tube produced minimal drainage and was subsequently discontinued. The patient remained in CVU for 3 days for monitoring and treatment of atrial fibrillation and was discharged home on the 4th postoperative day.
Discussion
Excessive bleeding after cardiac surgeries can be due to surgical cause, platelet dysfunction, thrombocytopenia, coagulopathy, and/or fibrinolysis [4]. Common causes include platelet dysfunction, residual heparinization, fibrinolysis and hypothermia [5].
The patient in this case report was at risk for platelet dysfunction due to continuation of aspirin therapy until two days prior to the surgery. Despite aspirin’s irreversible inhibition of platelet function via acetylation of cyclooxygenase-1 and blockade of thromboxane A2 production, the current recommendation is continuation of the medication perioperatively, as it may improve the outcome without significantly increasing bleeding after cardiac surgeries [6, 7]. The pathophysiology of perioperative hemorrhage associated with cardiac surgeries may arise from disruption of the endothelium, as well as from the circulatory assist device surface [8]. Prompt identification and control of the postoperative bleeding is crucial as uncontrolled bleeding of greater than 400ml/hr during the first hour, or 200ml/hr for each of the first 2 hours warrants surgical re-exploration [5]. In minimally invasive mitral valve surgeries, chest tube drainage of greater than 100ml/ hr for 2 consecutive hours is considered abnormal [9].
Traditional laboratory coagulation measurements take at least 20- 40 minutes and are often not practical in case of emergencies. Point-of-care (POC) testing such as TEG, thromboelastometry (an advancement of classic thromboelastography), and wholeblood impedance aggregometry offer coaglulopathy data within 15-30 minutes and facilitate differential diagnosis [10]. TEG is a widely used POC testing modality for monitoring coagulopathy in cardiac anesthesia as well as in trauma and liver transplantation. TEG evaluates the whole blood and is believed to have higher predictive accuracy (88%) for postoperative bleeding compared with that of routine coagulation screening (33%) [3]. TEG is strongly associated with reduced blood transfusion and associated complications without incurring greater blood loss compared with traditional testing [11-14]. Transfusion algorithms based on TEG have been instituted in some facilities [13-15].
The main values of TEG include R (Reaction time; the time period before fibrin clot is formed; normal range 4-8 minutes), K (kinetic time; the speed to reach a specified clot strength; normal range 0-4 minutes), α angle (the speed of fibrin cross-linking; normal range 47-74 degrees), MA (maximum amplitude; the clot strength; normal range 54-72mm), and LY30 (Lysis 30 minutes after MA; the clot stability; normal range 0-8%) [10] (Figure 1). Specific graphs generated indicate coagulopathy of specific origin (Figure 2). For the patient in this case report, the only abnormal TEG value was R (9.1 minutes). Pathology for increased R value is mainly coagulation factor deficiency or anticoagulant use [16], which, in this case, suggests inadequate reversal of heparin. The elevated PTT further supports the diagnosis of residual heparin effect.
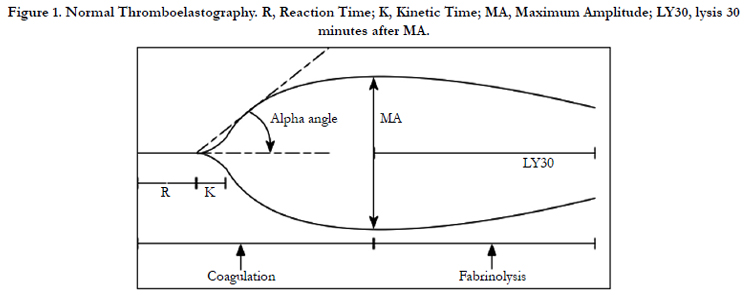
Figure 1. Normal Thromboelastography. R, Reaction Time; K, Kinetic Time; MA, Maximum Amplitude; LY30, lysis 30
minutes after MA.
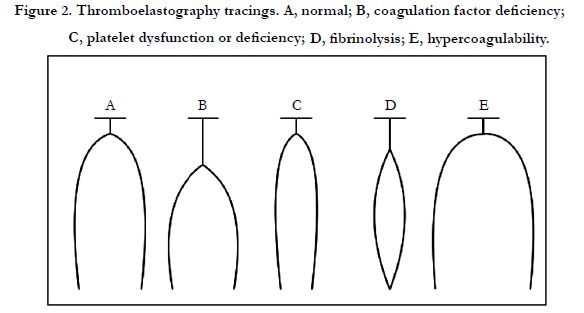
Figure 2. Thromboelastography tracings. A, normal; B, coagulation factor deficiency; C, platelet dysfunction or deficiency; D, fibrinolysis; E, hypercoagulability.
Platelet dysfunction or deficiency is mainly signified by MA. The patient’s MA was within the normal range, which suggested normal clot strength. Though the laboratory value of platelet count (92 x 109/L) indicated mild thrombocytopenia, a platelet count greater than 50 x 109/L has no correlation with post-CPB bleeding [5]. In addition, relative thrombocytopenia may persist for up to 72 hours after the cardiac surgery without consistent association with bleeding diathesis [5].
Despite the use of POC testing as guidance in treatment and blood transfusion, clinicians differ in their emphasis on the part of the coagulation pathway to be tackled. Various treatments and protocols including TEG-guided transfusion, fibrinogen replacement, activated Factor VII (FVIIa), antifibrinolytic agent, DDAVP have been explored. Some facilities use protocols based on TEG with success [12, 17]. Systematic reviews, however, conclude that the current evidence is weak in supporting TEG or thromboelastogram use to guide the transfusion in patients at high risk for massive transfusion [7, 18].
A number of recent studies found positive correlation between fibrinogen level and postoperative bleeding [19-21]. In addition, Gorlinger et al., and Rahe-Meyer et al., found that first line therapy with fibrinogen concentrate reduced transfusion requirements [22, 23]. A systematic review and meta-analysis by Gielen et al., however, revealed a significant but weak-to-moderate correlation between pre- and postoperative fibrinogen levels and postoperative blood loss, and suggested that additional studies are needed [24]. As for activated Factor VII (FVIIa), Menkis et al., pointed out that it should only be used in life-threatening situations after all the other pharmacological and surgical hemostatic interventions have failed because its use is associated with increased thrombotic events [7].
Current evidence supports the use of antifibrinolytic agents including Amicar and tranexamic acid (TA) [7]. DDAVP, on the other hand, is not recommended for routine use for post-CPB bleeding prophylaxis, but evidence supports its use in patients on aspirin within 7 days of the surgery, patients on CPB for greater than 140 minutes, and patients with demonstrated platelet dysfunction by TEG or platelet function assay [7, 25]. In this case report, the patient could have been given DDAVP considering her aspirin therapy within two days of the surgery.
Conclusion
Currently no consensus exists regarding the best monitoring modality or treatment for postoperative bleeding after cardiac surgeries. TEG holds great potential in goal-directed transfusion and reduction of unnecessary exposure to allogeneic blood products, but more clinical studies are needed to support its benefits. Though further evidence is needed, preoperative and post-CPB fibrinogen level may be useful in determining the need for fibrinogen concentrate administration to prevent or reduce postoperative bleeding. Antifibrinolytic therapy with Amicar or TA should continue to be part of the routine blood conservation strategy. In selected patients, DDAVP may be used towards hemostasis.
The postoperative hemorrhage in this case report was controlled in a timely manner and the potential surgical reexploration was averted. Based on the current evidence, the additional protamine administration to reverse the anticoagulant was supported by the POC testing and laboratory result. DDAVP instead of platelets, however, could have been used to avoid the exposure to allogeneic blood products.
Acknowledgement
The author would like to thank Mark Grieves, CRNA, MSN for his assistance and support in the completion of this article.
References
- Lucà F, van Garsse L, Rao CM, Parise O, La Meir M, et al. (2013) Minimally invasive mitral valve surgery: a systematic review. Minim Invasive Surg 179569.
- Atik FA, Svensson LG, Blackstone EH, Gillinov AM, Rajeswaran J, et al. (2011). Less invasive versus conventional double-valve surgery: a propensitymatched comparison. J Thorac Cardiovasc Surg 141(6): 1461-14618.
- Christensen MC, Krapf S, Kempel A (2009). Costs of excessive postoperative hemorrhage in cardiac surgery. The Journal of Thoracic and Cardiovascular Surgery 138(3): 687-93.
- DiNardo JA, Zvara DA, Malden, MA (2008) Anesthesia for Cardiac Surgery (3rd Edtn), Blackwell Publishing.
- Kaplan JA (2008) Essentials of Cardiac Anesthesia, Sounders Elsevier, Philadelphia.
- Mangano DT (2002) Aspirin and mortality from coronary bypass surgery. New England Journal of Medicine 347(17): 1309-1317.
- Menkis AH, Martin J, Cheng DC (2012) Drug, devices, technologies, and techniques for blood management in minimally invasive and conventional cardiothoracic surgery: a consensus statement from the International Society for Minimally Invasive Cardiothoracic Surgery (ISMICS) 2011. Innovations (Phila) 7(4): 229-41.
- Achneck H, Sileshi B, Parikh A (2010) Pathophysiology of bleeding and clotting in the cardiac surgery patient: from vascular endothelium to circulatory assist device surface. Circulation 122(20): 2068-2077.
- Navia, JL (2001) Minimally invasive mitral valve surgery. Second Virtual Congress of Cardiology http://www.fac.org.ar/index.php
- Görlinger K, Shore-Lesserson L, Dirkmann D (2013) Management of hemorrhage in cardiothoracic surgery. J Cardiothorac Vasc Anesth 27(4): 20-34.
- Manikappa S, Mehta Y, Juneja R, Trehan N (2001) Changes in transfusion therapy guided by thromboelastograph in cardiac surgery. Ann Card Anaesth 4(1): 21-7.
- Westbrook AJ, Olsen J, Bailey M () Protocol based on thromboelastograph (TEG) out-performs physician preference using laboratory coagulation tests to guide blood replacement during and after cardiac surgery: a pilot study. Heart Lung Circ 18(4): 277-288.
- Yin J, Zhao Z, Li J (2014) Goal-directed transfusion protocol via thrombelastography in patients with abdominal trauma: a retrospective study. World Journal Of Emergency Surgery: WJES 9(28): 12.
- Kashuk J, Moore E, Sauaia A (2012) Initial experiences with point-of-care rapid thrombelastography for management of life-threatening post injury coagulopathy. Transfusion 52(1): 23-33.
- Clements A, Jindal S, Morris C (2011) Expanding perfusion across disciplines: the use of thrombelastography technology to reduce risk in an obstetrics patient with Gray Platelet Syndrome--a case study. Perfusion 26(3):181-4.
- MacDonald SG, Luddington RJ (2010) Critical factors contributing to the thromboelastography trace. Semin Thromb Hemost 36(7):712-22.
- Girdauskas E, Kempfert J, Kuntze T (2010) Thromboelastometrically guided transfusion protocol during aortic surgery with circulatory arrest: a prospective, randomized trial. J Thorac Cardiovasc Surg 140(5): 1117-24.
- Wikkelsoe AJ, Afshari A, Wetterslev J, Brok J, Moeller AM (2011) Monitoring patients at risk of massive transfusion with Thrombelastography or Thromboelastometry: a systematic review. Acta Anaesthesiol Scand 55(10):1174-89.
- Uji M, Terada Y, Noguchi T (2012) Perioperative fibrinogen concentrations in cardiac surgery with cardiopulmonary bypass. Masui 61(8): 814-9.
- Waldén K, Jeppsson A, Nasic S, Backlund E, Karlsson M (2014) Low preoperative fibrinogen plasma concentration is associated with excessive bleeding after cardiac operations. Ann Thorac Surg 97(4):1199-1206.
- Karkouti K, Callum J, Crowther MA (2013) The relationship between fibrinogen levels after cardiopulmonary bypass and large volume red cell transfusion in cardiac surgery: an observational study. Anesth Analg 117(1):14-22.
- Görlinger K, Dirkmann D, Hanke AA (2011) First-line therapy with coagulation factor concentrates combined with point-of-care coagulation testing is associated with decreased allogeneic blood transfusion in cardiovascular surgery: a retrospective, single-center cohort study. Anesthesiology 115(6): 1179-91.
- Rahe-Meyer N, Solomon C, Hanke A (2013) Effects of fibrinogen concentrate as first-line therapy during major aortic replacement surgery: a randomized, placebo-controlled trial. Anesthesiology 118(1): 40-50.
- Gielen C, Dekkers O, Stijnen T (2014) The effects of pre- and postoperative fibrinogen levels on blood loss after cardiac surgery: a systematic review and meta-analysis. Interact Cardiovasc Thorac Surg 18(3): 292-8.
- Wademan BH, Galvin SD (2014) Desmopressin for reducing postoperative blood loss and transfusion requirements following cardiac surgery in adults. Interact Cardiovasc Thorac Surg 18(3): 360-70.





