Tophaceous gout of the spine: A case report and review of the literature
Youdi Xue1MD, Limin Liu2MD,Yueming Song2MD, Zeyu Huang2 MD
1 Department of Orthopaedic Surgery, Xuzhou Central Hospital, China
2 Department of Orthopaedic Surgery, West China Hospital, Sichuan University, China.
*Corresponding Author
Youdi Xue,
Department of Orthopaedic Surgery,
Xuzhou Central Hospital, China.
E-mail: xueydspine@163.com
Article Type: Case Report
Received: July 21, 2014; Accepted: August 16, 2014; Published: August 19, 2014
Citation: Youdi Xue, Limin Liu, Yueming Song, Zeyu Huang (2014) Tophaceous gout of the spine: A case report and review of the literature. Int J Anesth Res. 2(6), 59-62. doi: dx.doi.org/10.19070/2332-2780-1400015
Copyright: Youdi Xue, MD.© 2014 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Tophaceous gout is the final phase in the development of gout. Tophi form from the deposition of monosodium urate crystals can be found in the surrounding joints and periarticular tissues. Accumulation of tophi in the spine is rare. We report a case of spinal gout involving the thoracic spine resulted in spinal cord compression and incomplete paraplegia. Surgery was performed for decompressing the spinal canal, and tophaceous gout is certified from intraoperative and histological examination.
2.Case report
3.Discussion
4.References
Keywords
Images Study; Spinal Cord Compression; Tophaceous Gout.
Case report
A 48-year-old male was admitted to the orthopedic department presented with a history of progressive motor weakness of both lower extremities and numbness below the xiphoid process over the last five months. His condition was aggravated over the last month and he was nonambulatory on admission. His case history included diabetes mellitus, hypertension,and gouty arthritis. Insulin and oral drugs were used for controlling blood glucose and blood pressure respectively, but nothing was given for gouty arthritis except nonsteroidal antiinflammatory drugs to relieve the intermittent pain. Physical examination showed that the patient presented with central obesity and had massive subcutaneous nodules suggesting gout tophi in limbs distal joints. Atrophy of the quadriceps femoris was observed with muscle power decreased to grade 3(3/5) and muscle conus elevated with exaggerated knee and ankle jerks and positive babinski signs; Hypoesthesia below the T6 level was also observed. Laboratory studies was remarkable for an elevated erythrocyte sedimentation rate (111.0mm/h,normal, 21mm/h) and C-reactive protein (94.80mg/L; normal, 5mg/L). The patient's white blood count was normal (9040/mm3).Routine radiography revealed no useful information. From the computed tomography (CT) lesions were seen as hyper dense soft tissue mixed with nodular deposits at the thoracic level of 7-8(figure1). Magnetic resonance imaging(MRI) of the thoracic spine revealed space-occupying erosions posterior to the epidural space at T7-8 level and the focal spinal stenosis were considered, small erosions were also noted at endplate at T7-10 segment and anterior to the vertebral bodies at the same level.(figure2).
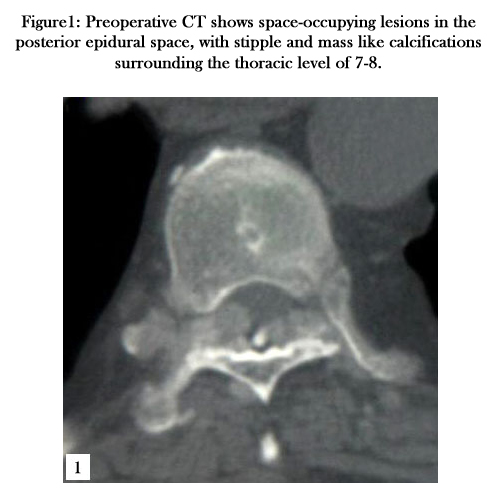

Figure1: Preoperative CT shows space-occupying lesions in the posterior epidural space, with stipple and mass like calcifications surrounding the thoracic level of 7-8.
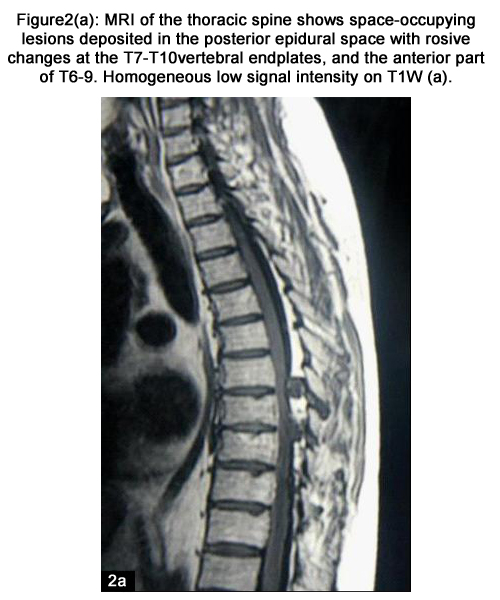
Figure2(a): MRI of the thoracic spine shows space-occupying lesions deposited in the posterior epidural space with erosive changes at the T7-T10vertebral endplates, and the anterior part of T6-9. Homogeneous low signal intensity on T1W (a).
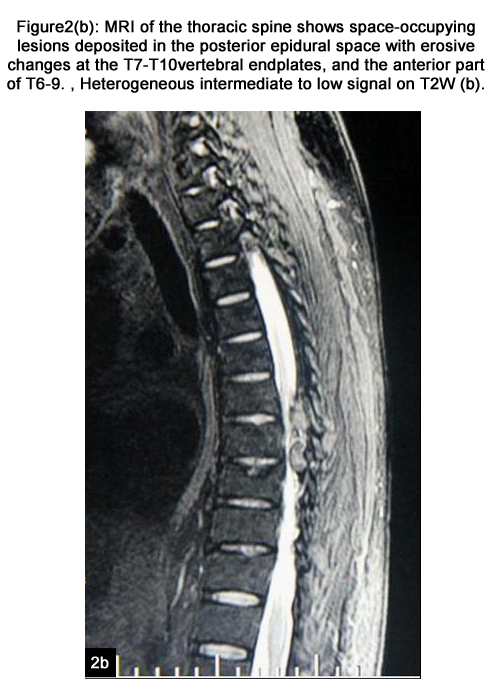
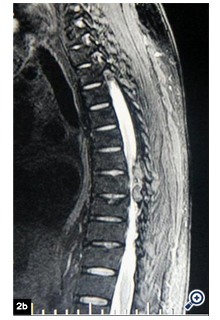
Figure2(b): MRI of the thoracic spine shows space-occupying lesions deposited in the posterior epidural space with erosive changes at the T7-T10vertebral endplates, and the anterior part of T6-9. , Heterogeneous intermediate to low signal on T2W (b).
Because the symptoms were progressively aggravated, surgical intervention was carried out for decompression by laminectomy in the T7-T10 vertebral levels. During the surgery, massive chalkywhite, paste-like granular materials were observed at the laminar surfaces and extradural space with extension to the ventral epidural space, which caused severe spinal canal stenosis and dural compression. The subsequent histological studies amorphous material surrounded by multinucleated giant cells. (figure3) The diagnosis of tophaceous gout was therefore established. After surgery, uric lowering medication and rehabilitation was given, and the muscle power of both lower limbs begins to recover progressively. At one years follow up, the muscle power regains almost normal and the hypoesthesia below the T6 level is disappear.
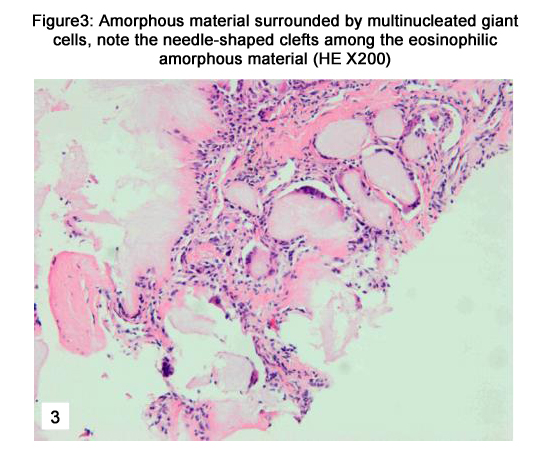
Figure3: Amorphous material surrounded by multinucleated giant cells, note the needle-shaped clefts among the eosinophilic amorphous material (HE X200)
Discussion
Gout is a very common metabolic disorder mainly due to hyperuricemia that results from an imbalance between the rate of production and excretion of uric acid in the body [1]. The peripheral joints are the most frequent involved structures, whereas tophi deposition can happen everywhere in the body such as axial skeleton. Gout involvement of spine is rare but it can cause pain with or without fever, radiculopathy, myelopathy, or cauda equina syndrome according to the different level or part involved.[2,3]. The lumbar spine is the most common affected level followed by cervical and thoracic spine, and the involved region can be any part of spine including osseous part and ligamentous or muscular part [4]. Our patient had gouty erosions almost involved every spinal structures, and this has not been reported before.
Making the diagnosis of spinal gout is difficult since the spinal gout is not very common and the clinical manifestation is various, especially without history of gouty attacks or when the serum urate level is within the normal range, in fact, serum urate level may be normal in 30% patients with acute gouty attacks.
Images study is important to make the diagnosis of the spinal gout. Plain radiograph may be normal or with nonspecific abnormality such as degeneration, thicking of soft tissue. MRI features of tophaceous gout of the spine have been described in recent reports [5,6], which shows homogeneous and low-signal intensity on T1 weighted images as well as heterogeneous and various signal intensities on T2 weighted images. However, these changes are nonspecific; they can also be found with bacterial, fungal, or mycobacterial infections. The enhancement pattern is also variable, probably due to the differences in the relative amounts of vascular fibrous tissue in the tophi [5]. MR imaging to be non-specific in the diagnosis of gout with variable imaging appearances of tophi from low to intermediate signal on T1- and T2-weighted imaging, respectively [1]. CT appears very specific for the diagnosis of tophaceous gout, Tophi appear as typical massa of about 160-170 HU causing bony erosions with well-defined sclerotic margins [7],which is clearly inferior to that of deposits of calcium containing crystals, which have an attenuation of about 450 HU, but sometimes in old tophi or in necrotic centers of tophi, calcifications or ossifications can be found and diagnosis will be difficult to make under these conditions [6]. Dual-energy CT (DECT) is a novel image study on gouty disorder, and may be used to confirm the diagnosis. Because the DECT system is able to differentiate materials based on their chemical composition which enables easy classification of the scanned tissue. This allows accurate and specific characterization of monosodium urate crystals from calcium. DECT has the potential to be a problem-solving tool that can be utilized to diagnose the presence of gout in challenging clinical presentations and potentially obviating the need for biopsy [8,9].
The key to make the diagnosis is careful and overall history taking, analysis of images study, and image-guided fine biopsy or the pathological examination of specimen harvested from the surgery is necessary for the definitive diagnosis. Uric acid lowering medication is essential in order to decrease serum uric acid levels and to prevent recurrence of neurological compromise resulted from accumulation of tophi at the epidural space. Medical treatment of tophi with steroids may be effective if the nature of the cord compression is acute intense inflammation [10]. Thus the early diagnosis following the description of lowering uric medications can improve the prognosis and making the decompressive surgery unnecessarily. Surgical intervention should be considered if the neurological compromise is persistent without improvement under medical treatment.
References
- Schumacher HR Jr. Becker MA, Edwards NL, Palmer WE, MacDonald PA, Palo W, Joseph-Ridge N. Magnetic resonance imaging in the quantitative assessment of gouty tophi. Int J Clin Pract. 2006; 5(60):408-414.
- Arnold MH, Brooks PM, Savvas P, Ruff S. Tophaceous gout of the axial skeleton. Aust N Z J Med. 1998; 18(7):865-867.
- Paquette S, Lach B, Guiot B. Lumbar radiculopathy secondary to gouty tophi in the filum terminale in a patient without systemic gout:case report. Neurosurgery. 2000; 46(4):986-988.
- Konatalapalli RM, Demarco PJ, Jelinek JS, Murphy M , Gibson M, Jennings B, Weinstein A. Gout in the axial skeleton. J Rheumatol. 2009; 36(3):609-613.
- Hsu CY, Shih TT, Huang KM, Chen PQ, Sheu JJ, Li YW. Tophaceous Gout of the spine: MR imaging Features. Clin Radiol. 2002; 57:919-925.
- Talbott JH, Altman RD, Yü TF. Gouty arthritis masquerading as rheumatoid arthritis or vice versa. Semin Arthritis Rheum. 1978; 8:77–114.
- Gerster JC, Landry M, Dufresne L, Meuwly JY. Imaging of tophaceous gout:computed tomography provides specific images compared with magnetic resonance imaging and ultrasonography. Ann Rheum Dis. 2002;61:52-54.
- Fiona M McQueen, Anthony Doyle, Nicola Dalbeth. Imaging in gout - What can we learn from MRI, CT, DECT and US? Arthritis Res Ther.2011; 13:246-254.
- Nicolaou S, Yong-Hing C, Galea-Soler. Dual energy computed tomography as a potential new diagnostic tool in the management of gout in the acute setting. Am J Roentgenol. 2010; 194:1072–1078.
- Dhote R, Roux FX, Bachmeyer C, Tudoret L, Daumas Duport C, Christoforov B. Extradural spinal tophaceous gout: evolution with medical treatment. Clin Exp Rheumatol. 1997; 15(4):421-423.





