Comparison of Continuous Epidural Analgesia and Continuous Femoral Analgesia
on Postoperative Pain and Knee Rehabilitation after Total Knee Arthroplasty
N. Erdogan1, S.Savlı1, M.Kaya1*, G.Ozalp2, G.Oguz1, N. Kadıogulları1
1 Dept of Anesthesiology, Ankara Oncology Education and Research Hospital, Ankara, Turkey.
2 Dept of Anesthesiology, Associate Professor, Ankara Oncology Education and Research Hospital, Ankara,Turkey.
*Corresponding Author
Mensure Kaya,
Yunusemre Mah. Asan Sok,
41/7 Yenimahalle 06170,
Ankara,Turkey.
Tel: 90 312 3158036;
Fax: 90 312 3454979
E-mail: mensurekaya@yahoo.com
Article Type: Research Article
Received: January 14, 2014; Accepted: February 5, 2014; Published: February 7, 2014
Citation: M Kaya et al (2014) Comparison of Continuous Epidural Analgesia and Continuous Femoral Analgesia on Postoperative Pain and Knee Rehabilitation after Total Knee Arthroplasty. 2(1), 28-32. doi: dx.doi.org/10.19070/2332-2780-140008
Copyright: M Kaya© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
This study assessed the efficacy of postoperative analgesia and rehabilitation scores of continuous epidural analgesia or continuous femoral analgesia after total knee arthroplasty. Thirty patients received epidural analgesia (Group E), whereas 30 patients received continuous femoral analgesia (Group F). Pain and rehabilitation scores, total bupivacaine consumption and rescue analgesic consumption were compared.
Pain scores were similar between the two groups. Total bupivacaine consumption was significantly higher in Group F. One patient in Group E and 13 patients in Group F required for supplemental analgesics (p<0.05).Maximum knee flexion degrees were not different between the two groups.
In this study, an effective pain control was obtained with both continuous epidural analgesia and continuous femoral analgesia after total knee arthroplasty.
2.Introduction
3.Materials and Methods
4.Results
5. Discussion
6. References
Keywords
Continuous Peripheral Nerve Blocks; Postoperative Analgesia; Epidural Analgesia Knee Arthroplasty.
Introduction
Postoperative analgesia management after total knee arthroplasty is very important for improving the function of knee joint, strengthening muscular contraction and early mobilization of patients. Systemic opioids, epidural and peripheral nerve blocks are widely used for pain relief after knee arthroplasty. In many prospective randomized controlled studies, it is suggested that regional analgesia techniques provide superior pain relief and faster postoperative knee rehabilitation than traditional intravenous or intramuscular routes [1-3]. The concerns about interactions of anticoagulants and central neuroaxial techniques increased the interest in peripheral nerve blocks [1, 2, 4, 5]. The aim of this study was to compare the analgesic efficacy, early rehabilitation and the side effects of continuous epidural analgesia with continuous femoral analgesia after total knee arthroplasty.
Materials and Methods
After approval from our institutional ethics comittee and written informed consent from each patient, 60 ASA physical status I-III patients scheduled for elective unilateral total knee artroplasty under spinal anesthesia were included in this prospective study. The patients were randomly allocated to one of two postoperative analgesia groups; first group receiving continuous epidural analgesia (Group E, n=30), second group receiving continuous femoral analgesia (Group F, n=30). Sealed opaque envelopes were used for the randomization process. Patients with columna vertebralis deformities, mental detoriation, chronic analgesic use, peripheral neuropathy, coagulation abnormalities, systemic arthritis-arthralgy, allergy to local anesthetics and <50 or >100 kg weight were excluded from the study. Low molecular weight heparin once a day beginning 12-16 h before anaesthesia, was used for thrombopophylaxis. At preoperative interview, the patients were instructed in the use of the visual analogue scala (VAS 0=no pain 100=severe pain) and the patient controlled analgesia (PCA) device (Acute Pain Manager-APM, Abbott, IL, USA).
Patients were premedicated with midazolam 0.07 mg/kg im before surgery. In the operation room before performing spinal anesthesia, all of the patients received an infusion of 5 ml/kg NaCl % 0.9. Routine monitorization included ECG, noninvasive blood pressure, heart rate and pulsoxymeter and the basal measurements were noted.
In group F, all femoral blocks were performed in the holding area or operating room before surgery. Under sterile conditions 55 mm block needle was inserted perpendicular to skin approximately 1 cm lateral to the femoral artery pulse that was marked 1 cm under the inguinal ligament, then the needle was rotated cephalad at a 45°angle. Peripheral nerve stimulator (Stimuplex- DIG©; Braun, Geisingen, Germany) adjusted to 1.5 mA output, 2 Hz frequency and 0.1 msn was used for the localization of the femoral nerve. When a quadriceps muscle contraction was elicited with a stimulus of 0.5 mA or less (patellar twitch), 20 G femoral catheter (Contiplex® D set, B. Braun Melsungen AG) was placed with Seldinger technique. Catheters were threaded 8-10 cm into the femoral nerve sheath and fixed to skin with a suture to avoid catheter dislodgement. After negative aspiration test for blood, 30 ml of bupivacaine 0.25 % was given through the catheter as initial bolus dose. Sensory block was assessed in the distrubitions of the femoral (anterior aspect of the thigh), the lateral femoral cutaneous (lateral aspect of the thigh), and the obturator nerve (medial aspect of the knee) 30 minutes after injection of local anesthetic by using cold perception (partial or complete loss of temperature sense). Motor block was assessed by testing the knee extension (femoral nerve) and thigh adduction (obturator nerve). Presence of block was defined as weakness at operative leg against the resistance made by the hand of examiner. The results of sensory and motor tests were reported as either yes or no for every nerve distribution area.
After the assessment of sensorial and motor blocks, spinal anesthesia was performed at L3-4 or L4-5 interspace with 15 mg 0.5 % isobaric bupivacaine in sitting position. Adequate anesthesia was verified by the absence of sensation (cold perception) at T10 or above 20 minutes after the injection of the local anesthetic. In group E, patients received combined spinal-epidural anesthesia (Espocan®+Docking System+Perifix®Soft Tip; Braun, Melsungen, Germany). In sitting position epidural puncture was performed with an 18 G Tuohy needle in the L3-4 or L4-5 interspace by using loss of resistance technique. After subaracnoid administration of 15 mg of 0.5% isobaric bupivacaine, a 20G epidural catheter was threaded 5 cm into the epidural space and then fixed with suture to the skin as femoral catheters.
In both groups, the number of attempts for correct catheter placement and ease of catheter placement (easy, moderate, and difficult) was noted. After spinal anesthesia, mean arterial pressure (MAP) and heart rates (HR) were recorded every 5 min during the first 30 min and then every 15 min until the end of the surgery. Hypotension was defined as MAP<70 mmHg and treated with an infusion of 200 ml of 0.9 % NaCl solution and/or ephedrine 5-10 mg IV. Bradycardia was defined as HR< 50 beats/min and treated with atropine 0.5 mg IV. The sensorial and motor block levels 20 min after spinal anesthesia, operation time and ephedrine consumption during the surgery were noted for both groups.
At the end of the operation, all patients were taken to the recovery room. When the level of the sensorial block regressed to L1, patients in both groups received a bolus dose of 10 ml 0.25 % bupivacaine through the catheters and then the catheters were connected to the PCA device which was adjusted to deliver PCA boluses of 0.05 ml/kg 0.125 % bupivacaine with the lockout time of 30 min and 0.1 ml/kg/h continuous infusion during the first 48 h postoperatively.
Pain at rest and on movement of the operated leg was assessed with VAS at 0, 6, 12, 24 and 48 h after the operation. When VAS pain score was ≥ 40, patients received morphine 0.1 mg/kg subcutanously as a rescue analgesic. Postoperative hemodynamic parameters were evaluated at the same times. The Bromage scale was used to assess the duration of motor block due to spinal anesthesia in both groups.
Early rehabilitation was initiated on the first day after operation and maximum knee flexion degree of each patient was assessed and recorded at first and second days. Supplemental analgesic consumption, total bupivacaine use, total number of bolus demands and side effects like nause-vomiting, hypotension, headache, backache and urinary retention were recorded.
All of the catheters were removed the end of postoperative 48 h. Local inflammatory signs (focal pain, redness,and induration) at the insertion site was defined as catheter infection. The length of hospital stay and satisfaction of patients from the analgesic technique used (good, moderate, and inadequate) were noted. All of the patients underwent a neurological evaluation at discharge from the hospital.
The statistical analysis was performed using SPSS 10.0 for Windows. Parametric data with normal distrubition were compared by using Student’s t test and abnormal distribution with Mann Whitney U test. Nonparametric data were compared by using Chi-square test and Mann Whitney U test with a Bonferoni correction for multiple comparisons as appropriate and a p value <0.05 was considered significant. All data are presented as mean ± SD, median (min-max) and percent.
Results
The demographic characteristics of patients and operation time were similar between the two groups (Table1). No patient required general anesthesia due to failure of neuroaxial block and no patient was excluded at any stage of the study.
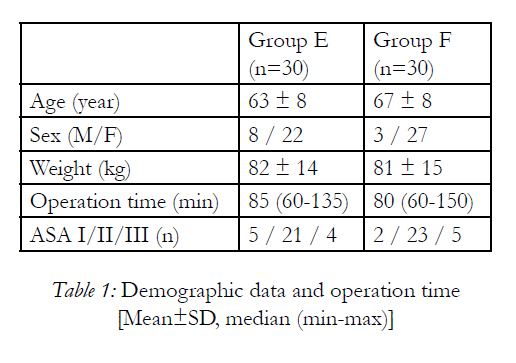

Table 1: Demographic data and operation time [Mean±SD, median (min-max)].
Sensorial block level 20 min after spinal anesthesia was at T10 in Group E and T8 in Group F. MAP, HR and ephedrine consumption during the surgery were similiar between the groups. Number of attemps for catheter placement, difficulty of catheterization, regression time of sensorial block to L1 and resolution time of motor block were not significantly different between groups (Table 2).
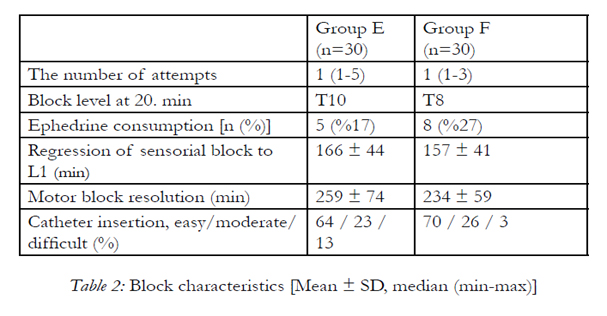
Table 2: Block characteristics [Mean ± SD, median (min-max)].
VAS pain scores at rest and on movement are presented in Table 3. Adequate pain relief was achieved with both regional analgesia techniques; no statistically significant difference was noted between groups.
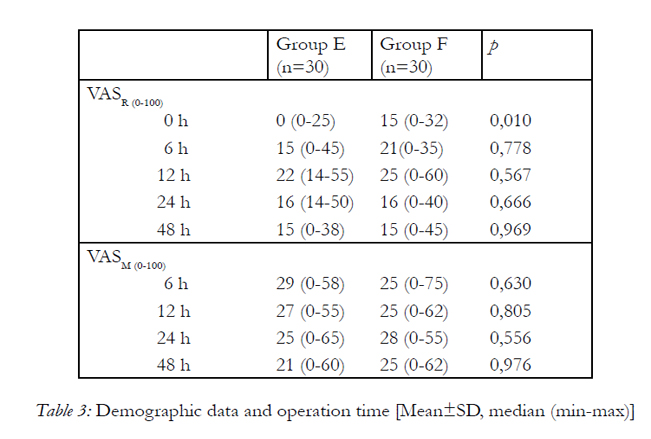
Table 3: Demographic data and operation time [Mean±SD, median (min-max)].
Postoperative MAP values were lower in Group E,and statistically significant at 6 and 12 h (Bonferroni correction p<0.0083). HR was not different between groups.
Total amount of bupivacaine consumption was significantly higher in Group F (419 ml in Group E, 476 ml in Group F). The total number of bolus demands from PCA infuser was found to be significantly different between the groups, 79 (8-179) in Group E and 189 (37-618) in Group F (p<0.05). Additional analgesic consumption was statistically different between the groups (p<0.05). One patient in Group E and 13 patients in Group F required for supplemental analgesics. Maximum knee flexion degrees were 54 ± 16.8 in Group E and 48 ± 13.7 in Group F on the first postoperative day, 84 ± 10.0 and 79 ± 12.4 respectively on second day (Table 4).
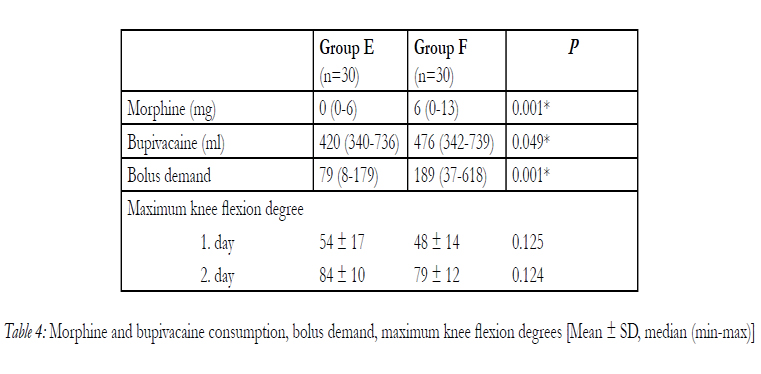
Table 4: Morphine and bupivacaine consumption, bolus demand, maximum knee flexion degrees [Mean ± SD, median (min-max)].
In Group F, the preoperative sensorial block in the cutaneous distribution of the femoral nerve, lateral femoral cutaneous nerve and obturator nerve was obtained at a rate of 100 %, 93 % and 100 % respectively. Preoperative motor block was found to be 100 % for femoral nerve and 90 % for obturator nerve in the same group. After spinal anesthesia complete sensorial and motor block of lower extremities was obtained in both groups. The motor block was absent (Bromage 0) at postoperative 6. h in the two groups.
There were no statistically significant differences between groups with regard to side effects like nausevomiting, hypotension, headache, backache and urinary retention. The length of hospital stay and patient satisfaction were similar (Table 5). None of the patients had local signs of infection or neurological deficit.
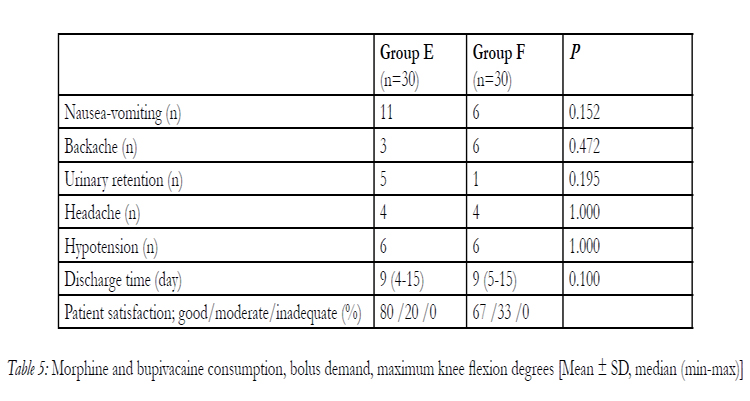
Table 5: Morphine and bupivacaine consumption, bolus demand, maximum knee flexion degrees [Mean ± SD, median (min-max)].
Discussion
In this study, effective pain control facilitating knee rehabilitation was obtained with continuous epidural analgesia and continuous femoral analgesia after total knee arthroplasty.
Postoperative severe pain after total knee arthroplasty is associated with the reflex spasm of quadriceps muscle and adequate pain relief is neccesary for postoperative knee rehabilitation and functional recovery [2]. When pain is inadequately treated, early mobilization of patients can not be achieved; therefore capsuler contraction and adhesions threating the success of surgery will occur [2,6].
All of the patients in this study have participated the exercise and early rehabilitation programme after knee arthroplasty at the orthopedic clinic. There was no significant difference in maximum degree of knee flexion between the two groups at the first and second postoperative days. At the end of the second day, 84 ± 10.0 and 79 ± 12.4 degrees were achieved in Group E and Group F respectively. The concentration of local anesthetic and the doses used in this study did not cause motor block which could hinder the early mobilization postoperatively.
In the present study comparing the epidural block and femoral 3-in-1 block, we didn’t find any difference in the analgesic efficacy between the two regional techniques. Nevertheless total bupivacaine and rescue analgesic consumption and total number of bolus demands from PCA infuser were more in Group F. The use of 16 % more bupivacaine and more additional analgesic need can be assessed as a disadvantage of femoral analgesia. There was no adverse effect caused by the low doses of morphine used as rescue analgesic in this study. Although lower doses of local anesthetics are used for epidural analgesia, disturbing side effects such as sympathetic block are likely to occur due to central blockade 1,2. The other frequent side effects of epidural block include orthostatic hypotension, nauseavomiting and urinary retention. Although a significant difference was not shown in this study, the incidence of nausea-vomiting and urinary retention was higher in Group E. The similar incidence of headache and backache was thought to be associated with the spinal anesthesia performed for the surgery.
Although the intraoperative and postoperative hemodynamic variables were statistically similar between the two groups, MAP and HR were lower in Group E in the postoperative period. The orthostatic hypotension due epidural analgesia can cause a delay in functional recovery and rehabilitation by by restricting early postoperative mobilization. In a prospective randomized study, it was reported that side effects were observed 4 times more with epidural analgesia than with continuous femoral analgesia [2]. And in another study, femoral 3 in 1 block has been shown to produce lower incidences of nausea and vomiting [6].
We used the same continuous infusion and bolus doses of local anesthetic in both groups for 48 hours. Although the safety of continuous infusion is reported, it may lead to the accumulation of the local anesthetic that is administered at large volumes and had a potential risk of toxicity after prolonged periods of infusions [7,8]. There were no clinical symptoms or signs of local anesthetic toxicity during the study period. The continuous infusion of 0.125 % bupivacaine at the rate of 0.14 ml/kg/h is considered as “gold standart” to maintain adequate and safe femoral analgesia [9]. We used 0.125 % bupivacaine 0.05 ml/kg with a lockout time of 30 minutes and 0.1 ml/kg/h continuous infusion as recommended during the first 48 h postoperatively. In this study, all the catheters were placed successfully in both groups. The number of attempts for catheterisation was not different between the two groups. Comparing with the other regional techniques, femoral nerve 3-in-1 block is easier to perform requiring no special positioning of the patient [10]. Catheter placement into femoral nerve sheath using a peripheral nerve stimulator is found to be successful in 80-100 % of patients [3,11,12]. We could not compare the duration of the procedure as spinal anesthesia was chosen for the surgery and epidural catheter was placed as a part of combined spinal-epidural technique in the present study.
The sensorial block was found to be 100 % for both the femoral nerve and the obturator nerve in our study and the motor block was 100 % and 90 % respectively. Although the obturator nerve has beeen reported to be inadequately blocked with the femoral 3-in-1 technique, we obtained adequate postoperative analgesia [13,14]. This can be associated with the individual variations in the innervation of the knee. In our study, we achieved adequate analgesia and early knee rehabilitation despite the absence of motor block of the obturator nerve. Bouaziz et al have reported that the cutaneous distribution of obturator nerve was absent in 57 % of their patients [15]. The discrepancy between the sensory and motor block can also be a result of the high variation in the cutaneous distribution of the obturator nerve in our study.
None of the patients had motor block due to spinal anesthesia 6 h after the operation. Alhough continuous epidural analgesia with local anesthetic might be associated with a greater incidence of motor block, we didn’t observe any during the study [16]. This can be related to the use of low concentration of the local anesthetic and apropriate dose titration with PCA.
An effective postoperative analgesia management can facilitate early mobilization and functional recovery, thus reduces the duration of hospital stay and costs after total knee arthroplasty. Mahoney and colleagues have reported that epidural analgesia had improved pain control and early rehabilitation was associated with a reduction of approximately 2 days in the length of hospital stay but the high incidence of side effects should not be ignored [17]. Many other studies have demonstrated adequate analgesia, accelerated rehabilitation, minimal side effects and short hospital stay after single dose femoral block or continuous infusion [3,6,18,19,20]. In our study, the discharge times from the hospital were similar between the two groups.
The incidence of catheter infections generally increases as long as the catheters stay in place. The risk of infection limits the duration of postoperative analgesic use through the catheters. Cuvillon et al have reported colonization of 57 % of femoral catheters in 208 patients
after 48 h, 3 of which had infection requiring no antibiotics [21]. The rate of colonization was 28.8 % in 1443 epidural catheter series of Simpson at al and the incidence was not found to be related with the catheter duration [22]. Although bacterial analysis was not performed after the removal of the catheters, we did not observe any local infection signs or neurological deficit at discharge attributable to the blocks in our study.
In this study, we concluded that continuous femoral analgesia, providing similar analgesic efficacy, rehabilitation and ease of mobilization, can be a good alternative to epidural analgesia that is still widely used for postoperative analgesia after total knee arthroplasty. Although the incidences of side effects were similar between the two groups, larger series of patients are needed for further evaluation.
References
- Capdevila X, Barthelet Y, Biboulet P, Ryckwaert Y, Rubenovitch J, d’Athis F. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology 1999; 91(1): 8-15.
- Singelyn FJ, Deyaert M, Joris D, Pendeville E, Gouverneur JM. Effects of intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous three-in-one block on postoperative pain and knee rehabilitation after unilateral total knee arthroplasty. Anesth Analg 1998; 87(1): 88-92.
- Chelly JE, Greger J, Gebhard R, Coupe K, Clyburn TA, Buckle R, Criswell A. Continuous femoral nerve block improve recovery and outcome of patients undergoing total knee arthroplasty. J Arthroplasty 2001; 16(4): 436-45.
- Zaric D, Boysen K, Christiansen C, Christiansen J, Stephensen S, Christensen B. A comparison of epidural analgesia with combined continuous femoral-sciatic nerve blocks after total knee replacement. Anesth Analg 2006; 102. 1240-6.
- Singelyn FJ, Ferrant T, Malisse MF, Joris D. Effects of intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous femoral nevre sheath block on rehabilitation after unilateral total hip arthroplasty. Reg Anesth And Pain Med 2005; 30(5): 452-7.
- Barrington MJ, Olive D, Low K, Scott DA, Briltain J, Choong P. Continuous femoral nerve blockade or epidural analgesia after total knee replacement: a prospective randomized controlled trial. Anesth Analg 2005; 101(6): 1824-9.
- Esteve M, Veillette Y, Ecoffey C, Orhant EE. Continuous block of the femoral nerve after surgery of the knee: pharmacokinetics of bupivacaine. Ann Fr Anesth Réanim 1990; 9: 322-5.
- Kaloul I, Guay J, Côté C, Halwagi A, Varin F. Ropivacaine plasma concentrations are similar during continuous lumbar plexus blockade: using the anterior three-in-one and the posterior psoas compartment techniques? Can J Anesth 2004; 51: 52-6.
- Anker-Moller E, Spangsberg N, Dahl JB, Christensen EF, Schultz P, Carlsson P. Continuous blockade of the lumbar plexus after knee surgery: a comparison of the plasma concentrations and analgesic effect of bupivacaine 0.250% and 0.125%. Acta Anaesthesiol Scand 1990; 34: 468-472.
- Edwards ND, Wright EM. Continuous low dose 3-in-1 nerve blockade for postoperative pain relief after total knee replacement. Anesth Analg 1992; 75: 265-267.
- Liu SS, Salina FV. Continuous plexus and peripheral nerve blocks for postoperative analgesia. Anesth Analg 2003; 96: 263-72.
- Grant SA, Nielson KC, Greengrass RA, Steele SM, Klein SM. Continuous peripheral nerve block for ambulatory surgery. Reg Anesth Pain Med 2001; 26: 209-14.
- Parkinson SK, Mueller JB, Little WL, Bailey SL. Extent of blockade with various approaches to the lumbar plexus. Anesth Analg 1989; 68: 243-8.
- Macalou D, Trueck S, Meuret P, Heck M, Vial F, Ouloguem S, Capdevila X, Virion JM, Bouaziz H. Postoperative analgesia after total knee replacement: the effect of an obturator nerve block added to the femoral 3 in 1 nerve block. Anesth Analg 2004; 99: 251-4.
- Bouaziz H, Vial F, Jochum D, Macalou D, Heck M, Meuret P, Braun M, Laxenaire M C. An evaluation of the cutaneous distribution after obturator nerve block. Anesth Analg 2002; 94: 445-9.
- Collis RE, Plaat FS, Morgan BM. Comparison of midwife top-ups, continuous infusion and patient-controlled epidural analgesia for maintaining mobility after a low-dose combined spinal-epidural. Br J Anaesth 1999; 82: 233-6.
- Mahoney OM, Noble PC, Davidson J, Tullos HS. The effect of continuous epidural analgesia on postoperative pain, rehabilitation, and duration of hospitalization in total knee arthroplasty. Clin Orthop Relat Res 1990; 260: 30-37.
- Wang H, Boctor B, Verner J. The effect of single-injection femoral nerve block on rehabilitation and length of hospital stay after total knee replacement. Reg Anesth Pain Med 2002; 27 (2): 139-44.
- İsaac D, Falode T, Liu P, I’Anson H, Dillow K, Gill P. Accelerated rehabilitation after total knee replacement. Knee 2005; 12: 346-50. v
- Sundarathiti P, Ruananukul N, Channum T, Kitkunasathean C, Mantay A, Thammasakulsiri J, Sodsee W. A comparison of continuous femoral nerve block (CFNB) and continuous epidural infusion (CEI) in postoperative analgesia and knee rehabilitation after total knee arthroplasty (TKA). J Med Assoc Thai. 2009; 92(3): 328-34.
- Cuvillon P, Ripart J, Lalourcey L, Veyrat E, L’Hermite J, Boisson C, Thouabtia E, Eledjam JJ. The Continuous femoral nerve block catheter for postoperative analgesia: bacterial colonization, infection rate and adverse effects. Anesth Analg 2001; 93: 1045-9.
- Simpson RS Macintyre PE, Shaw D, Norton A, McCann JR, Tham EJ. Epidural catheter tip cultures: results of a 4 year audit and implications for clinical practice. Reg Anesth Pain Med 2000; 25: 360-7.





