Size of Bulla Ethmoidalis and Sinonasal Mucosa: Does it Matters in Osteomeatal Complex Obstruction?
Hosapatna M, Prasanna LC, Ankolekar VH*
Associate Professor, Department of Anatomy, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India.
*Corresponding Author
Dr. Mamatha Hosapatna,
Associate Professor, Department of Anatomy,
Kasturba Medical College, Manipal Academy of Higher Education,
Manipal. Karnataka, India, Pin: 576104.
Tel: +91 8762938099
E-mail: vrinda.hari@manipal.edu
Received: June 28, 2018; Accepted: July 06, 2018; Published: July 07, 2018
Citation: Hosapatna M, Prasanna LC, Ankolekar VH. Size of Bulla Ethmoidalis and Sinonasal Mucosa: Does it Matters in Osteomeatal Complex Obstruction?. Int J Anat Appl Physiol. 2018;4(2):87-90. doi: dx.doi.org/10.19070/2572-7451-1800015
Copyright:Hosapatna M© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Bulla ethmoidalis is derived from the Latin word where bulla means a hollow, thin-walled, bony prominence. It is formed by pneumatisation of the bulla lamella or second ethmoid basal lamella. An extensively pneumatised bulla may expand anteriorly coming into intimate contact with the posterior free margin of the uncinate process, thereby narrowing or partially blocking the hiatus semilunaris.
Material and Methods: 40 bisected halves of the formalin fixed adult human head and neck specimens were procured from the Department of Anatomy. Retrospectively, we procured 20 CT films both in coronal and axial views of paranasal sinus from the Department of Radiology. Anatomical variations and mucosal abnormalities are analysed.
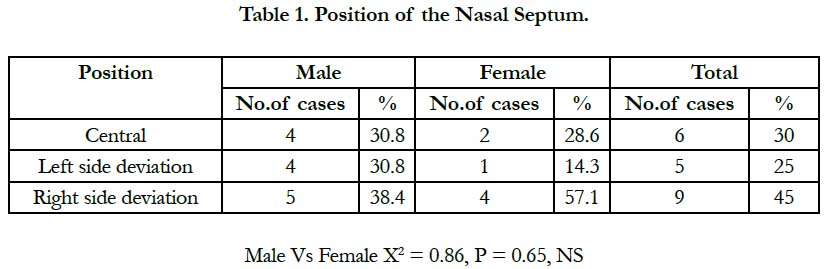
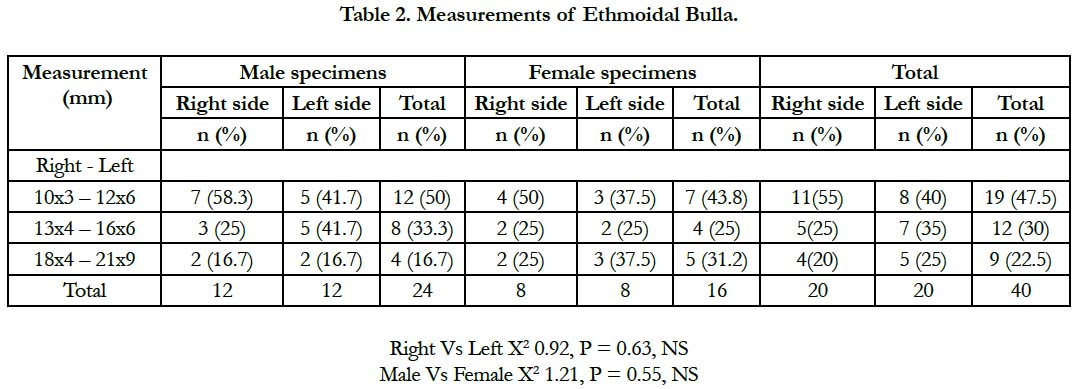
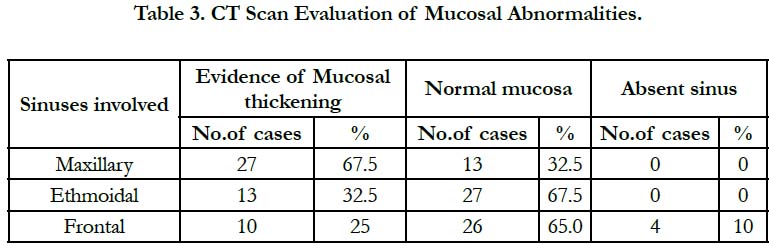
Results: In the present study of the position of nasal septum in 20 PNS CTs, 6 (30%) CTs showed centralized nasal septum, 5 (25%) showed left side deviation and 9 (45%) had right side deviation of the nasal septum. Bulla measuring 10x3 mm to 12x6 mm were present in 19(47.5%) specimens, 13x4 to 16x6 mm present in 12 (30%) and 18x4 to 21x9 mm seen in 9 (22.5%) cases. CT evaluation of Mucosal thickening was observed in maxillary sinus 27 (67.5%) cases, followed by ethmoidal sinus 13 (32.5%).
Conclusion: The CT scan should not be used exclusively to diagnose chronic sinusitis or to determine the need for surgery. Rather, it should be used to provide supplementary clinical data to the history and endoscopic exam and assist in directing surgical treatment to the affected areas.
2.Introduction
3.Material and Methods
3.1 Collection of Specimens
3.2 Inclusion Criteria
3.3 Exclusion Criteria
3.4 Dissection Method
3.5 Paranasal sinus CT Method
4.Results
5.Discussion
6.Conclusion
7.References
KeyWords
CT Scan; Pneumatisation; Bulla Ethmoidalis; Hiatus Semilunaris.
Introduction
Bulla ethmoidalis is derived from the Latin word where bulla means a hollow, thin-walled, bony prominence. It is formed by pneumatisation of the bulla lamella or second ethmoid basal lamella [1]. It is one of the most constant features in the middle meatus containing the largest anterior ethmoidal cells, but it may be poorly aerated or completely unpneumatised, hence its alternative nomenclature of torus lateralis (lateral bulge) [2].
The ethmoid bulla is a primitive structure that forms on the medial orbital wall. There may be up to four cells pneumatising the bulla, with the most common one being positioned superoposteriorly. In most cases, the ostium opens supero-posteriorly into the middle meatus or sinus lateralis [3, 4].
The extent of pneumatisation of the ethmoidal bulla is variable ranging from no pneumatisation to extensive pneumatisation. An extensively pneumatised bulla may expand anteriorly coming into intimate contact with the posterior free margin of the uncinate process, thereby narrowing or partially blocking the hiatus semilunaris [5-8].
Mucociliary drainage of the sinuses eventually merges into two common pathways, allowing division into two anatomic and functional groups. The first group (frontal, anterior ethmoidal, middle ethmoidal and maxillary sinuses) drains into the middle meatus, around the ethmoid bulla, called as the ostiomeatal unit. This region is frequently involved by inflammatory disease. The second group (posterior ethmoidal and sphenoidal sinuses), draining into the sphenoethmoidal recess and superior meatus, is less frequently affected by inflammatory processes [9]. An enlarged bulla can compromise the infundibulum or middle meatus.
When sinus drainage is obstructed mucus, inflammatory cells and bacteria accumulate, oxygen tension in the sinuses is reduced and opsonisation/phagocytic, as well as immunoglobulin - dependent activities are impaired. Drainage and ventilation of the major paranasal sinuses are dependent on the patency of the ostiomeatal complex [10].
The role of anatomical variants in the sinusitis genesis is controversial. Theoretically, these variants could shift and compress ostiomeatal complex components determining an obstruction to the paranasal sinuses mucus drainage. Scribano et al., have observed that if the anatomical variant determines obliteration of the aerial space of the ostiomeatal complex drainage paths, the sinusal disease is more frequently detected at CT than when the anatomical variant does not obstruct these pathways [11].
40 bisected halves of the formalin fixed adult human head and neck specimens were procured from the Department of Anatomy, KMC, Manipal (India).
Adult patients presenting with history of nasal obstruction and headache, who are subjected to radiological investigations after a clinical examination and diagnosis as sinusitis were included for the study.
Patients with previous alteration of the paranasal sinus anatomy due to facial trauma, benign tumours of the sinonasal mucosa and previous sinus surgery were excluded from the study.
The anterior part of the skull was divided in the midline then the entire nasal septum was removed piecemeal taking care not to damage the ostiomeatal components. Middle concha was trimmed to view the relationship of structures within the middle meatus. The specimens were washed in normal saline. Then different colored plastic probes, yellow for maxillary and red for frontal were used to view the sinus ostium. Ethmoidal bulla area was identified and marked to take the measurements with digital Vernier calipers. The observations were noted for study and analysis.
Retrospectively, we procured 20 CT films both in coronal and axial views of paranasal sinus from the Department of Radiology, KMC & H, Manipal (India). We excluded patients with sinonasal pathology, recurrent sinus infection, surgeries related to nose.
The coronal plane is the preferred imaging plane that best displays the ostiomeatal unit. All CT scans were obtained with Siemens Somatom AR scanner. After obtaining the preliminary lateral topogram of the skull, the area of scanning was defined to include the region from root of frontal sinus upto the hard palate. Coronal sections were performed with the patients in prone position, with extended neck and the plane perpendicular to the infraorbitomeatal line. The sections were taken with slice thickness of 5mm. The scans thus generated were photographed at appropriate window widths and window level. They were analysed for anatomical variations and mucosal abnormalities.
Results
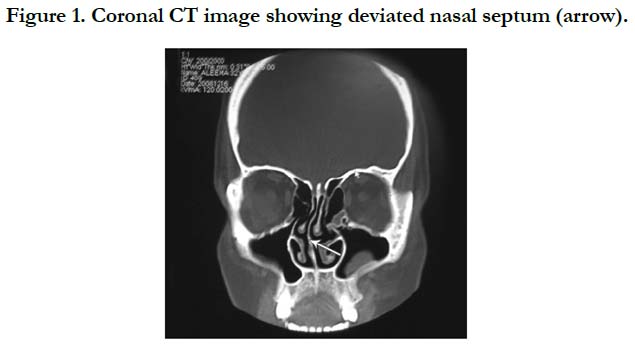
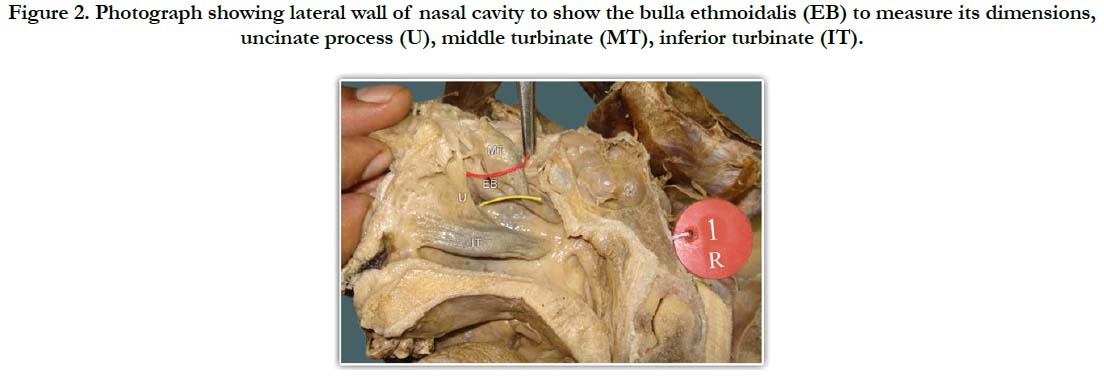
In the present study of the position of nasal septum (Figure 1) in 20 PNS CTs, 6 (30%) CTs showed centralized nasal septum, 5 (25%) showed left side deviation and 9 (45%) had right side deviation of the nasal septum. Male to female comparison of the position of the nasal septum showed p-value of 0.65, which is statistically not significant (Table 1). Bulla (Figure 2) measuring 10x3 mm to 12x6mm were present in 19 (47.5%) specimens, 13x4 to 16x6 mm present in 12 (30%) and 18x4 to 21x9 mm seen in 9 (22.5%) cases. Statistical comparison of right and left, male and female showed p-value of 0.63 and 0.55 respectively, which were statistically not significant (Table 2). CT evaluations of mucosal abnormalities in different sinuses were noted. Mucosal thickening was observed in maxillary sinus 27 (67.5%) cases, followed by ethmoidal sinus 13 (32.5%) cases and frontal sinus 10 (25%) cases, while in 4 (10%) cases showed absence of frontal sinus (Table 3).


Discussion
The complex microarchitectural pathway comprising of the frontal recess, the maxillary ostium and the infundibulum is referred to as “ostiomeatal complex”. Even subtle mucosal disease in this area causes obstruction to the drainage of the anterior group of sinuses causing chronic sinusitis [12, 13]. Septal deviation is thought to laterally compress the middle concha and uncinate process into the infundibulum and thereby cause obstruction of the ostiomeatal unit [5]. Deviation of the nasal septum was found in 65% of cases in the present study. In other studies, this finding ranged from 14.1% to 80%: Dutra and Marchiori 14.1%, Kinusi et al., 23.3%, Arslan et al., 36%, Earwaker 44%, Perez Pinas et al., 80%, Maru 55.7% and 38% by Asruddin [11-14]. Septal deviation seems to be associated with more disease on the side of the deviation in adults [5]. The exact prevalence of enlarged ethmoid bulla is not known. Its size is an important factor when associated with opacification of anterior ethmoidal cells at CT in patients diagnosed with sinusopathy. However, one has not found in the literature an objective description of what could be considered an enlarged ethmoidal bulla [11]. Ethmoidal bulla measuring 10x3 mm to 12x6 mm were present in 19 (47.5%) specimens, 13x4 mm to 16x6 mm present in 12 (30%) and 18x4 mm to 21x9 mm seen in 9 (22.5%) specimens in the present study. According to Som, mucosal abnormalities ranged from minimal mucosal thickening to total sinus opacification [14, 9]. Maxillary sinus was the most commonly involved sinus (67.5%) in the present study, followed by ethmoidal sinus (32.5%) and frontal sinus (25%). Some disparities between frequencies and types of anatomical variants of ostiomeatal complex in different studies can be explained by some controversial factors. May be these divergences could be explained either by population differences, by the definition adopted for anatomical variants or by the methodology of analysis. Finally, since each variant seems to have a different influence on the development of the sinus disease, it would be convenient to determine the risk of each variant independently [11].
Conclusion
The CT scan should not be used exclusively to diagnose chronic sinusitis or to determine the need for surgery. Rather, it should be used to provide supplementary clinical data to the history and endoscopic exam and assist in directing surgical treatment to the affected areas. The size of the ethmoid bulla is an important factor which can narrow the infundibulum leading to obstruction of ostiomeatal complex. Mucosal abnormalities associated with sinusitis were predominantly seen in maxillary sinus, followed by ethmoidal and frontal sinuses respectively.
References
- Stammberger H, Hawke M. Essentials of endoscopic sinus surgery. 1st ed. St. Louis: Mosby; 1993. p.43.
- Dua K, Chopra H, Khurana AS, Munjal M. CT scan variations in chronic sinusitis. Ind J Radiol Imag. 2005 Jul 1;15(3):315.
- Jones NS. CT of the paranasal sinuses: a review of the correlation with clinical, surgical and histopathological findings. Clin Otolaryngol Allied Sci. 2002 Feb;27(1):11-7. PubMed PMID: 11903365.
- Anon JB, Rontal M, Zinreich SJ, Thumfart WF, Vidič B. Anatomy of the paranasal sinuses. New York: Thieme; 1996 Jan. p.3-41.
- Davis WE, Templer J, Parsons DS. Anatomy of the paranasal sinuses. Otolaryngol Clin North Am. 1996 Feb;29(1):57-74.
- Mafee MF. Preoperative imaging anatomy of nasal-ethmoid complex for functional endoscopic sinus surgery. Radiol Clin North Am. 1993 Jan;31(1):1-20. PubMed PMID: 8419967.
- Mattox DE, Delaney RG. Anatomy of the ethmoid sinus. Otolaryngol Clin North Am. 1985 Feb;18(1):3-42.
- Paul WF, Bruce H, Valerie JL. Otolaryngology, Head & Neck Surgery. In: Schllers De, Thomas JR editors. The nose and paranasal sinuses. 6th ed. Baltimore: Elsevier Mosby; 2014. p.3504.
- Bolger WE, Parsons DS, Butzin CA. Paranasal sinus bony anatomic variations and mucosal abnormalities: CT analysis for endoscopic sinus surgery. Laryngoscope. 1991 Jan;101(1 Pt 1):56-64. PubMed PMID: 1984551.
- Shikani AH. Sinusitis: A head and neck surgeon’s perspective. Med Gen Med. 1991;1(2).
- Araujo SA, Martins P, Souza AS, Baracat EC, Nanni L. The role of ostiomeatal complex anatomical variants in chronic rhinosinusitis. Radiol Bras. 2004;14:1-9.
- Riello AP, Boasquevisque EM. Anatomical variants of the ostiomeatal complex: tomographic findings in 200 patients. Radiol Bras. 2008 Jun;41(3):149- 54.
- Perez-Pinas I, Sabate J, Carmona A, Catalina-Herrera CJ, Jimenez-Castellanos J. Anatomical variations in the human paranasal sinus region studied by CT. J Anat. 2000 Aug;197 ( Pt 2):221-7. PubMed PMID: 11005714.
- Dua K, Chopra H, Khurana AS, Munjal M. CT scan variations in chronic sinusitis. Ind J Radiol Imag. 2005 Jul 1;15(3):315.





