Palatoradicular Groove: An endoperiodontal continuum, Diagnosis and Management
Kumar P1, Kumar D2*, Sonowal ST3
1 Senior Resident, Unit of periodontics, Oral Health Sciences Centre, Post Graduate Institute of Medical Education & Research, Chandigarh, India.
2 Ex Senior Resident, Unit of Oral & Maxillofacial Surgery, Oral Health Sciences Centre, Post Graduate Institute of Medical Education & Research,
Chandigarh, India.
3 Senior Lecturer, Unit of Periodontics, Mansarovar Dental College, Bhopal, Madha Pardesh, India.
*Corresponding Author
Dr. Dinesh kumar,
Ex Senior Resident, Unit of Oral & Maxillofacial Surgery,
Oral Health Sciences Centre, Post Graduate Institute of Medical Education & Research,
Chandigarh, India.
Tel: +91 9855995525 (M)
E-mail: dr_dinesh78@yahoo.com
Received: November 13, 2015; Accepted: January 08, 2016; Published: January 12, 2016
Citation: Kumar P, Kumar D, Sonowal ST (2016) Palatoradicular Groove: An endoperiodontal continuum, Diagnosis and Management. J Translational Clin Case Rep Fam Physician. 2(1), 9-12.
Copyright: Kumar D© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
A 28-year-old man presented to the department of periodontology with chief complaint of recurrent swelling with pus discharge in the vestibular area of maxillary right lateral incisor since 3 weeks. On clinical examination a periodontal pocket of 12 mm was noted on palatal aspect in middle third running towards apex. On radiographic interpretation an irregular radiolucency at apex gave a suspicion of palatoradicular groove, which was then explored and managed surgically along with bone graft.
2.Case Report
3.Discussion
4.References
Introduction
Periodontitis is an inflammatory disease characterized by the destruction of the periodontal ligament and the alveolar bone [1]. It results from the interaction of the host defense mechanism with the dental plaque microorganisms [2]. Local factors such as irregularities in root anatomy, developmental abnormalities, subgingival restoration margins and overhanging dental restorations play a significant role in the pathogenesis of periodontitis. Inherent anatomic and morphologic features of the teeth can have a significant impact on the diagnosis, management, and prognosis of the involved tooth/teeth [3].
Anatomic aberrations are often seen in the human dentition. The maxillary incisor region of the permanent dentition where these anatomical aberrations are commonly seen is considered an area of embryonic hazard. Aberrations affecting the external and internal morphology can at times be the cause of complex pathological conditions involving the pulpal and periodontal tissues and can pose a challenge to the clinician for diagnosis and clinical management. One such anatomical aberration is a developmental groove involving the crown and extending a variable distance onto the root. The palatal surface of the maxillary lateral incisor and labial surface of the maxillary central incisor are most commonly involved. Such developmental grooves affecting maxillary lateral incisors are termed palatoradicular grooves (PRG). This anomaly has also been termed radicular anomaly, palatogingival groove, distolingual groove and radicular lingual groove [4, 5, 6, 7]. This anomaly can pose dilemmas for diagnosis and clinical management. A majority of palatoradicular grooves (93.8%) affect maxillary lateral incisors, and may result from an infolding of the enamel organ and the epithelial root sheath of Hertwig. Some have suggested that the anomaly results from an attempt to form another root [8]. Kovacs (1971) called this anomally ‘syndesmo-corono-radicular tooth’ [9]. These grooves act as a nidus for plaque accumulation which destroys the sulcular epithelium and later deeper parts of the periodontium, finally resulting in the formation of a severe localized periodontal lesion since proper cleaning of that site is difficult, if not impossible, for the patient. These grooves may also lead to combined endodonticperiodontal lesions, since there might be a communication between the pulp canal system and the periodontium through accessory canals. The prognosis of teeth affected by this anomaly depends upon the depth and extension of the groove. Shallow grooves may be corrected by odontoplasty in conjunction with periodontal treatment. However, when the groove is more advanced, treatment of the tooth is almost always doomed to be a failure either because of pulpal or periodontal breakdown.
A case is presented of a maxillary lateral incisor with a shallow palatoradicular groove extending up to the root apex with severe periodontal destruction. The tooth was successfully managed by restorative and surgical periodontal therapy.
With a prevalence of 2–5% the PRGs are one of the rare anomalies of tooth development [10]. Also it has been found that most of the grooves exhibit a length of more than 5 mm. The origin of PRG has been explained as a result of the alteration in the growth of inner enamel epithelium and Hertwig’s epithelial root sheath (HERS). Along with having numerous similarities to dens invaginatus, it has also been considered as an aborted attempt for the formation of an additional root [11]. Some authors have also suggested a genetic preponderance of this groove [12]. PRGs have been classified as simple and complex; while simple groove results from partial infolding of HERS, the complex one is characterized by direct communication with pulp. The most complex form of groove may even separate an accessory root from the main root trunk. Based on location they are classified as distal, mesial and central pattern. The distal pattern is most common and has been witnessed in approximately 70% of cases [13].
This report includes a case involving PRG and describes the relationship between the PRG, its affects on the periodontium, and the clinical management of such situations.
Case Report
A 28-years-old male patient reported with the chief complaint of swelling in the gums with pain in the right upper anterior tooth. Clinical examination revealed an abscess in the vestibular area of maxillary right lateral incisor and a deep periodontal pocket in the palatal aspect measuring 12 mm with an associated PRG. The same tooth was Grade II mobile. A periapical radiograph revealed a radiolucent area in relation to the apex of maxillary right lateral incisor with mild bone loss (Horizontal type) in coronal one third of the root (Figures1, 2, 3). Patient’s general medical history was taken and was found to be non-relevant. The etiology of the patient’s chief complaint was explained to him and written consent was taken. The initial treatment protocol, consisted of scaling and root planing followed by endodontic treatment as the lesion was endo- periodontal in nature (Figure 4). The abscess resolved completely and the mobility reduced to Grade I in severity. After a period of two months of post endodontic treatment, a full thickness flap was reflected to reveal the full extent of the groove. It also was noted that the interdental area distal to the maxillary right lateral incisor contained a large amount of granulation tissue (Figure 5). On the palatal aspect the groove extended to the apical third of the root. Scaling and root planing were carried out to remove the subgingival calculus and the granulation tissue was curetted. Due to extensive loss of bone, additive osseous surgery involving placement of a bone graft (PerioGlass) was carried out. The groove was restored to obliterate the defect, using glass ionomer restorative material to eliminate further plaque retention and its recurrence (Figures 6, 7). Sutures were placed and the patient was prescribed antibiotics and analgesics (amoxicillin 500 mg TID for five days and ibuprofen 400 mg TID for three days) (Figure 8). The patient was advised to use chlorhexidine gluconate mouthwash (0.12 percent) to supplement his oral hygiene regimen. Sutures were removed after ten days. The patient was instructed in proper oral hygiene measures and motivated to maintain his oral hygiene at a higher level to prevent recurrence of the disease. Healing was uneventful with satisfactory patient compliance. It was followed by supportive periodontal therapy. Patient was recalled for routine check up at 1, 3, 6 and 12 months, postoperative. Clinical examination revealed a reduction in Pocket depth to 4mm with radiographic evidence of significant bone fill in the apical area. No recurrence of pus discharge or sinus formation was noted (Figure 9).
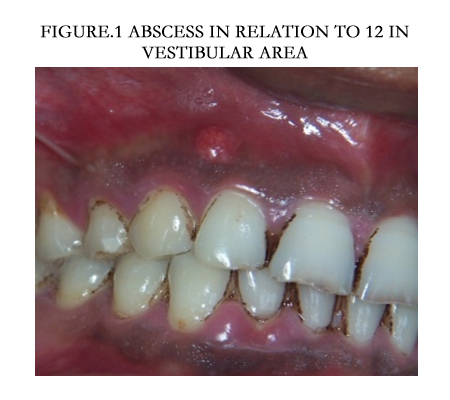

Figure1. Abscess in relation to 12 in vestibular area
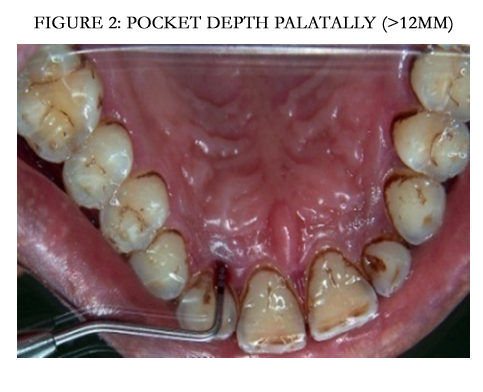

Figure2. Pocket depth palatally (>12mm)
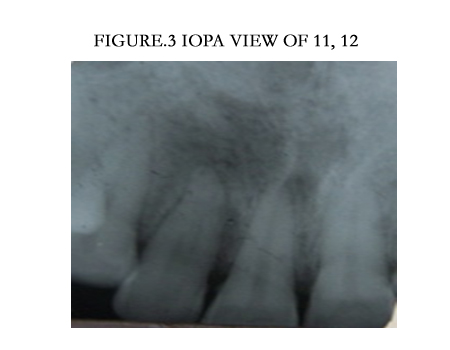

Figure3. IOPA view of 11, 12
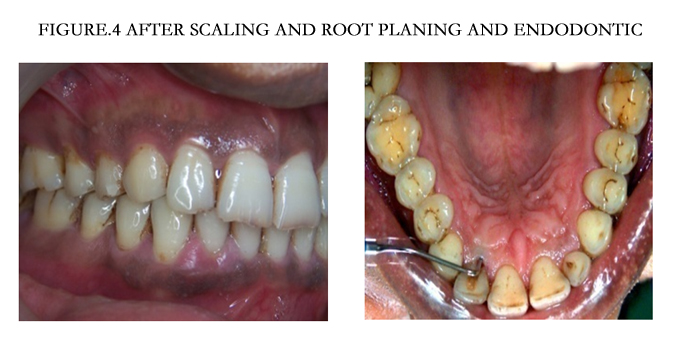

Figure4. After Scaling and Root Planing and endodontic
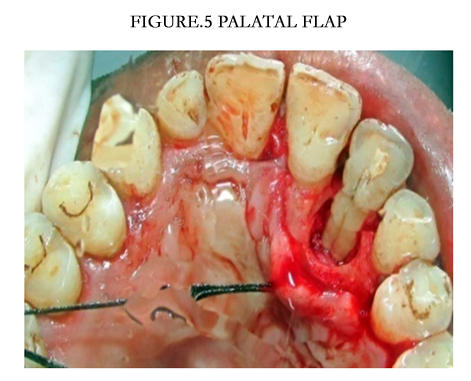

Figure5. Palatal flap
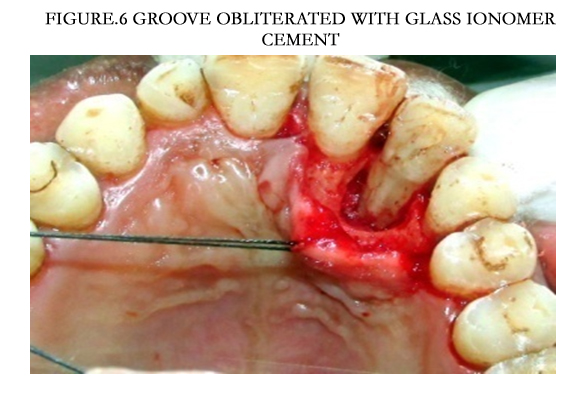
Figure6. Groove obliterated with Glass Ionomer Cement
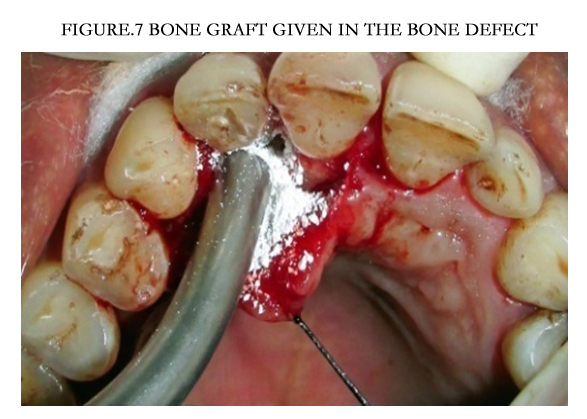

Figure7. Bone Graft given in the bone defect
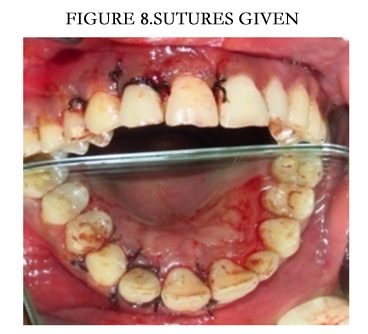

Figure8. Sutures given
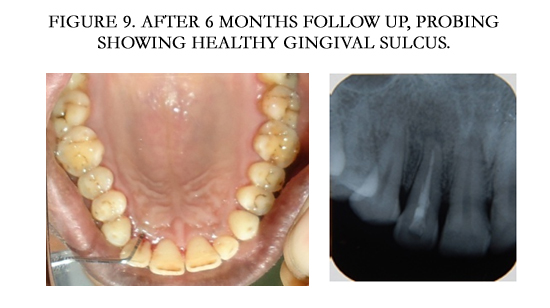

Figure9. After 6 months follow up, probing showing healthy gingival sulcus
Discussion
Palatoradicular groove is a rare developmental anomaly with a prevalence of 2-5% [7, 14]. This range represents different occurrences in different populations and sub-populations. Palatal grooves occur frequently on the maxillary lateral incisors, but less frequently on central incisors [15]. Also it has been found that most of the grooves exhibit a length of more than 5 mm. The origin of PRG has been explained as a result of the alteration in the growth of inner enamel epithelium and Hertwig’s epithelial root sheath (HERS). Along with having numerous similarities to dens invaginatus, it has also been considered as an aborted attempt for the formation of an additional root [12]. Some authors have also suggested a genetic preponderance of this groove [13]. For the sake of understanding, PRGs have been classified as simple and complex [12]. While simple groove results from partial infolding of HERS, the complex one is characterized by direct communication with pulp. The most complex form of groove may even separate an accessory root from the main root trunk. Based on location they are classified as distal, mesial and central pattern. The groove is more likely to form on the lateral surfaces (60 percent) than in the mid-palatal region (40 percent) [16]. The distal pattern is most common and has been witnessed in approximately 70% of cases [15]. However, Kogon [15] found the groove to be more frequently present on the mid- palatal regions. Hou [10] and Bacicet [16], postulated the distal and mesial locations of the groove to be more harmful than a midpalatal groove. This was because far more plaque accumulates in these regions, where it is difficult to remove. The occurrence of grooves extending from cingulum to apex, as in this case, appears to be extremely rare [7]. The diagnosis of the PRG may sometimes present a diagnostic dilemma because the patient usually presents with myriad signs and symptoms related to a true periodontal lesion or a true endodontic problem or sometimes a combination of both i.e., endo-periodontal lesion. Use of a disclosing agent may prove valuable because it can fill up the depressed groove area and visually differentiate the groove from sound tooth structure. In many cases it has been reported that delayed or improper treatment of a pathological groove was the consequence of an improper diagnosis. As suggested by Robinson, early diagnosis of PRG requiring periodontal treatment would simplify the treatment and improve the prognosis [16].
Various treatment modalities have been suggested that depend on the severity of the periodontal defect and type of groove (deep or shallow). Ramirez [17], Holem [18] and Everett and Kramer [7] suggested a curettage procedure with or without a flap and odontoplasty for shallow grooves. But the use of this method in deep grooves is questionable because of the excessive wear and tear of dentin which is obvious. Lee et al., [19] recommended doing an apically repositioned flap and placing amalgam in the groove. Rankow and Krasner [20] advocated surgical exposure of the defect and flattening of the groove by grinding with a highspeed diamond bur or fine stone, with or without application of the guided tissue regeneration (GTR) technique. Everett and Kramer [7] advised that if the groove is very deep, the prognosis is usually hopeless. On the other hand, if the groove is not deep with only shallow periodontal pocket, closed curettage is usually recommended to prevent attachment loss. If an open flap curettage is used to treat this condition, then expect a loss of periodontal attachment rather than a gain. When dealing with pockets of moderate depth, a flap surgery is advised along with sealing of the groove with a restorative material such as glass ionomer cement, dental amalgam, or a light-activated, resinbased composite. The principal disadvantage of these procedures may be the formation of a long junctional epithelium instead of a true regeneration of the lost attachment apparatus. This is because it also has been shown that when restorative materials are used to seal the groove, the result typically is a reduced epithelial attachment in that region. However, the advantages of using a sealant like glass ionomer cement are this material’s ability to provide a tight seal and its antibacterial property. When a sealant of some type is used, it prevents the formation of a dead space between the gingival flap and the depressed groove.
The rationale for using antibiotics in this case was to support individual host defenses in overcoming periodontal infections by eliminating subgingival pathogens that remain after periodontal instrumentation [21] and to prevent the systemic complications that may arise from a transient bacteremia following the surgical procedure. In this case, bone graft was used to fill the bone defect. The grooves were sealed with glass ionomer cement. This restorative material is known to have many advantages, such as the ability to bond chemically to enamel and dentin, biocompatibility, good cavity seal, as well as ease of use and low cost [22, 23]. Apart from these advantages, glass ionomers have a unique antibacterial property [20].
Perhaps the best technique or treatment option can be the use of GTR or enamel matrix derivatives, which usually show true regeneration of the lost attachment apparatus. In spite of all these treatment procedures, if periodontal maintenance at regular intervals is not carried out following any or all of these treatments, there is a greater likelihood of failure.
References
- Van Dyke TE, Lester MA, Shapira L (1993) The role of the host response in periodontal disease progression: implications for the future treatment strategies. J Periodontol 64(8 Suppl): 792-806.
- Offenbacher S (1996) Periodontal diseases: pathogenesis. Ann Periodontol 1(1): 821-878.
- Matthews DC, Tabesh M (2000) Detection of localized tooth-related factors that predispose to periodontal infections. Periodontol 34: 136-150.
- Prichard JS (1965) Advanced Periodontal Therapy. WB Saunders Co, Philadelphia.
- Lee KW, Lee EC, Poon KY (1968) Palato-gingival grooves in maxillary incisors. A possible predisposing factor to localised periodontal disease. Br Dent J 124(1): 14-18.
- Simon JH, Glick DH, Frank AL (1971) Predictable endodontic and periodontal failures as a result of radicular anomalies. Oral Surg Oral Med Oral Pathol 31(6): 823-826.
- Everett FG, Kramer GM (1972) The disto-lingual groove in the maxillary lateral incisor: a periodontal hazard. J Periodontol 43(6): 352-361.
- Peikoff MD, Trot JR (1977) An endodontic failure caused by an unusual anatomical anomaly. J Endod 3(9): 356-359.
- Kovacs I (1971) A systemic description of dental roots. In Dental Morphology and Evolution. University of Chicago Press, Chicago. 223-225.
- Hou GL, Tsai CC (1993) Relationship between palate-radicular grooves and localised periodontitis. J Clin Periodontol 20(9): 678-682.
- Schwartz SA, Koch MA, Deas DE, Powell CA (2006) Combined endodontic- periodontic treatment of a palatal groove: A case report. J Endod 32(6):573-578.
- Goon WW, Carpenter WM, Brace NM, Ahlfeld RJ (1991) Complex facial radicular groove in a maxillary lateral incisor. J Endod 17(5): 244-248.
- Ennes JP, Lara VS (2004) Comparative morphological analysis of the root developmental groove with the palato-gingival groove. Oral Dis 10(6): 378-382.
- Withers JA, Brunsvold MA, Killoy WJ, Rahe AJ (1981) The relationship of palato-gingival grooves to localized periodontal disease. J Periodontal 52(1):41-44.
- Kogon SL (1986) The prevalence, location and conformation of palatoradicular grooves in maxillary incisors. J Periodontol 57(4): 231-234.
- Bacic M, Karakas Z, Kaic Z, Sutalo J (1990) The association between palatal grooves in upper incisors and periodontal complications. J Periodontol 61(3): 197-199.
- Ramirez JM (1984) Management of a periodontal lesion associated with a lingual groove. Oral Health 74: 23-25.
- Holem S (1978) The radicular groove. J Am Dent Assoc 97: 441-444.
- Rankow HJ, Krasner PR (1996) Endodontic applications of guided tissue regeneration in endodontic surgery. J Endod 22(1): 34-43.
- Schäfer E, Cankay R, Ott K (2000) Malformations in maxillary incisors: case report of radicular palatal groove. Endod Dent Traumatol 16(3): 132-137.
- Slots J, Research, Science and Therapy Committee (2004) Systemic antibiotics in periodontics. J Periodontol 75(11): 1553-1565.
- Vanessa SL, Alberto C, Robert SB (2000) Macroscopic and microscopic analysis of the palato-gingival groove. J Endodontics 26(6): 345-350.
- Robinson SF, Cooley RL (1988) Palatogingival groove lesion: recognition and treatment. Gen Dent 36(4): 340-342.





