Tackling Cancer Stem Cell: From Science to Medicine
Chen D1*, Zhang X2
1 Research Institute of Biological Medicine, Yiling Pharmaceutical, Shijiazhuang, Hebei, P. R. China.
2 State Key Laboratory of Oncology, Biotherapy Center, Sun Yat-sen University Cancer Center; State Key Laboratory of Oncology in South China,
Collaborative Innovation Center for Cancer Medicine, Guangzhou, Guangdong, P. R. China.
*Corresponding Author
Daohong Chen,
Research Institute of Biological Medicine,
Yiling Pharmaceutical, Shijiazhuang, Hebei 050035, P. R. China.
E-mail: daohong@hotmail.com
Received: September 28, 2016; Accepted: October 20, 2016; Published: October 24, 2016
Citation: Chen D, Zhang X (2016) Tackling Cancer Stem Cell: From Science to Medicine. J Translational Clin Exp Oncology. 1(2), 6-11.
Copyright: Chen D© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
In spite of being a minor cellular subset, cancer stem cells (CSCs) fundamentally contribute to intra-tumor heterogeneity. With the biological features of self-renewal and differentiation, CSCs confer a driving force for malignant recurrence and anti-cancer drug resistance in oncologic patients, which highlight an unmet clinical need calling for innovative medicine to Come up. Due to the elusiveness of specific biomarkers and biological regulation for CSCs, a number of precisely targeted therapeutic approaches against CSCs are at their infancy far from reaching the clinic. However, we have herein been able to sort out three groups of CSC inhibitors which are clinically available, and proposed to take the advantages of these drugs to improve the therapeutic efficacy of existing anti-cancer treatments.
2.Background
3.Biological Properties
4.Clinical Implications
5.Drug Repositioning
6.CSC - Signaling Inhibitors
7.Herb Medicines
8.Perspective
9.References
Keywords
Cancer Stem Cells; Drug Repositioning; Signaling Inhibitor.
Background
It has been well known that cancer represents a highly heterogeneous disease owning to significant advances in cellular and molecular biology since the twenty first century. Although arising from a single cell or a few cells initially, all tumors inevitably undergo a series of patho-biological processes including clonal expansion, genetic diversification and macro-/micro-environment selection, consequently evolving into neoplastic disorders with profound heterogeneity at clinical phases [1, 2]. Tumor cell heterogeneity may present differential subtypes between individual cases with a same neoplasm as evidenced by distinct molecular signatures such as epidermal growth factor receptor (EGFR) and K-RAS, thus being referred as inter-tumor heterogeneity [3, 4] which has recently inspired the conceptual emergence of precision (or personalized) medicine. On the other hand, intra-tumor heterogeneity defines a hierarchical organization of cellular subpopulations within a given cancer tissue, of which one minor subset at the apex is termed cancer stem cells (CSCs) [2, 5]. The latter have been increasingly concerned in the fields of both cancer biology and innovational medicine because CSCs are believed to provide a fundamental driving force for malignant progression and therapeutic resistance [5, 6].
CSC subpopulation was originally discovered from a hematologic malignancy two decades ago. Acute myeloid leukemia (AML) cells were surprisingly revealed to be a heterogeneous population, in which a subset bearing CD34+CD38-, the biomarker of hematopoietic stem cells (HSC), exerted a hundred fold higher oncogenic activity than that of CD34+CD38+and CD34- fractions [7]. Moreover, the study with xenografted animals demonstrated that CD34+CD38- cells were able to expand and to differentiate into a heterogeneous AML cell population mimicking the pattern of the patient’s primary disease [6]. Later on, fractional heterogeneity and CSC activities were further uncovered in CD34- or CD38+ AML cells, suggesting that there may be multiple CSC subsets with divergent genetic background besides HSC source [8]. Likewise, CSC subsets have been subsequently determined in other types of leukemia beyond AML. In fields of solid tumors, breast CSCs were firstly identified and well characterized as CD44+CD24- cell subpopulation, which has undergone a number of genetic alterations linked to the malignant pathogenesis while still sharing certain functional properties with those of normal breast stem cells [6, 9]. In similar scenarios, CSCs have been accumulatively identified in many more types of solid tumors such as CD44+CD24+ cells for pancreatic malignancy, CD133+ cells for brain/colon/lung cancer, among others [10].
Biological Properties
In spite of substantial progress in cancer biology during recent years, the biological origin of CSCs is yet to be precisely delineated. To date, it has been generally noticed that, while stem cells in normal tissues can be malignantly transformed to CSCs and in turn to initiate neoplasms, conversely differentiated tumor cells display considerable plasticity to resume certain stemness features under certain pathological circumstances such as molecular alterations in cancer cells or in the adjacent microenvironment [6, 10]. These phenomena help to understand that CSCs present divergent cues of genetic background and highly variable frequencies from 0.0001% to 25% depending upon distinct tumor types and biological contexts within tumors [11]. However, there is a consensus that CSCs share several critical properties biologically with normal stem cells, including self-renewal and differentiation into multiple lineages of progeny cells [10, 11]. CSCs hold the capacity to renew themselves indefinitely in an undifferentiated state, to play a role of the “seeds” in tumor growth. In addition, CSCs can undergo asymmetric division to differentiate into more matured progeny cancer cells which mainly contribute to bulk building up of tumors [11, 12].
Not surprisingly, there are complex cellular/molecular regulating networks that contribute to promoting CSC phenotypes. Binding of cytokines to their cognate receptors activates the signaling cascades of Janus kinases-signal transducers and activators of transcription (JAK-STATs), among which JAK2 activation and STAT3 phosphorylation have been revealed to augment survival in myelo-proliferative neoplasms and solid tumors, respectively [13, 14]. Impressively, hyper-activity of EGFR (EGFRvIII in particular) –AKT pathway has been identified as the key signaling cascade for up-regulation of glioma CSCs, being linked to poor clinical prognosis [15]. Besides some shared biomarkers with normal stem cells, the key functional phenotypes of CSCs, such as self-renewal, are driven by several common stemness signaling pathways which have been inactivated or minimized in matured tissue physiologically. For example, Wnt/β-catenin signaling is upregulated in the CSCs of breast, colon and liver, whereas Hedgehog or/and Notch pathways are activated in the CSCs of brain, lung, pancreas and prostate [12, 14, 16]. Moreover, several core transcriptional factors for pluri-potency, such as sex determining region Y-box 2 (SOX2) and octamer-binding transcription factor 4 (OCT4), have been demonstrated to contribute to driving CSCs in a wide variety of tumors [14, 16]. In addition, the components in tumor microenvironment, including hypoxia inducible factor-1α (HIF-1α/nuclear factor-kB (NF-kB) activation under hypoxic conditions and transformation growth factor (TGF-β secreted from stromal cells, substantially augment CSC activities [5, 17].
Clinical Implications
Metastasis distinguishes malignancies from benign tumors pathologically, and represents a significant cause of patients’ mortality in clinical oncology. It has been recognized that cancer metastasis is driven by comprehensive contributing forces, including invasion capability of malignant cells and the responsive microenvironment (metastatic niche) [8, 17]. Whereas, only a small portion of cancer cells with the stemness features are able to detach from the primary tumor, and migrate to distant organs, to form metastatic malignancies [6, 18]. Accumulated evidence demonstrates that CSCs from a broad spectrum of cancer types bear highly up-regulated signaling activity of C-X-C motif chemokine 12 (CXCL12)/C-X-C chemokine receptor type 4 (CXCR4) axis, which is known to play a central role in cancer cell migration and dissemination [12, 19]. In cases of epithelial malignancies (carcinomas), a pathological alteration termed epithelial-to-mesenchymal transition (EMT) of cancer cells can be induced, at least in part, by a variety of stressful conditions in tumor microenvironment [12, 20]. Upon EMT, the malignant cells are noticed to have acquired biological features of CSCs such as constitutive activation of Wnt signaling cascade, and thus been conferred the capacity of detaching from primary tissue to commit metastasis [6, 20].
Although targeted therapeutic approaches developed in the last two decades have improved clinical efficacy and minimized adverse effects compared with conventional treatments, the emerging drug-resistant problems still present a challenging issue [21]. A growing body of evidence indicates that CSCs play a significant role in the resistance to both traditional treatments and targeted therapy, thus making most malignant diseases at advanced stages un-curable by available drugs [1, 5]. It has been revealed that CSCs may consist of a quiescent or dormant subset with slowcycling cellular process, to escape traditional chemotherapeutic compounds that kill rapidly dividing cells within a tumor mass through DNA damage or the related enzymatic inhibition [6]. Meanwhile, multiple drug resistance (MDR) gene-encoded protein transporters are highly up-regulated in CSCs in a wide variety of tumor types, and therefore lead to diminished therapeutic efficacy upon the dysregulated pharmacokinetic processes such as increased drug efflux out of responding cells [6, 22]. On the other hand, disease gene mutations and redundant activation of additional pro-survival signaling pathways have been identified as the major mechanisms of resistance to targeted therapeutic agents [21], which frequently occur in CSCs, including K-RAS mutations in colorectal tumors [12] and Wnt/β-catenin activation in breast cancer [9, 14], respectively.
Drug Repositioning
Metformin is a frequently prescribed medicine for type 2 diabetes and metabolic syndrome, through multiple mechanisms of action including insulin sensitization of muscle and adipocytes. In particular, epidemiological investigations have revealed the lower morbidity and mortality of cancer in diabetic patients treated with metformin, due at least partially to activation of 5-adenosine monophosphate activated protein kinase (AMPK) and inhibition of mammalian target of rapamycin (mTOR) pathway [23]. Moreover, metformin was found to suppress CSC phenotypes in various tumors such as CD133+ and CD44+/CD24 cells in pancreatic and breast cancers, respectively [23, 24]. In recent years, several clinical trials are ongoing to test metformin as a potential anti-cancer agent. There has been some evidence suggesting that metformin suppresses cancer proliferation biomarkers in patients [25], and improves the survival of resectable pancreatic cancer [26].
Aspirin has been historically utilized to control pain, fever, various inflammatory disorders, and later on to prevent inflammation-associated malignancies such as colorectal cancer. For instance, lowdose aspirin application for over 3 years was capable of reducing colon cancer incidence by 25% in the clinic [17]. Interestingly,aspirin has recently been discovered to inhibit CSC phenotypes in pancreatic cancer via suppressing an array of stemness signaling molecules including NF-kB and SOX2, to subsequently re-sensitize the malignant cells to gemcitabine [27]. As a result, it has also been noticed that dosing aspirin can minimize local spread and distant metastasis of cancer. Impressively, long-term daily use of aspirin was observed to reduce the systemically spreading cancer by 31%-55% [17, 28].
Disulfiram is an inhibitor of the aldehyde dehydrogenase (ALDH), and has been clinically used for over a half century to treat alcoholism. Given that up-regulation of ALDH represents one of the biochemical hallmarks of CSCs [9], disulfiram was lately explored further for potential effects on oncologic biology. It has been demonstrated that disulfiram diminishes growth and self-renewal of CSCs in brain tumors, by means of inhibiting ALDH, NF-kB, polo-like kinase 1 and modulating B-cell lymphoma (Bcl-2) family proteins [25, 29]. Meanwhile, disulfiram was also found to suppress CSCs and to overcome anti-cancer drug resistance in triplenegative breast cancer cells [30]. Moreover in a phase IIb clinical trial, the addition of disulfiram to an existing chemo-therapeutic regimen was well tolerated and able to improve survival of patients with newly diagnosed non-small cell lung cancer [31].
Salinomycin was originally developed as a veterinary drug to control coccidial infection in poultry feed, and to improve nutrient absorption in farmed pigs. Interestingly, salinomycin has been recently discovered to be preferentially toxic to CSCs in a broad spectrum of cancer types, such as CD44+/CD24- cells in breast cancer and CD133+ cells in pancreatic cancer [32, 33]. In terms of the underlying mechanisms, it has been noticed that salinomycin suppresses MDR protein function and induce CSC death upon impairment of mitochondrial function, excessive reactive oxygen species (ROS) generation [6, 22]. Besides, salinomycin is also capable of inhibiting several stemness-signaling pathways including Wnt/β- catenin and Akt/mTOR cascades [14, 23]. Moreover, clinical studies demonstrate that salinomycin can deliver marked therapeutic benefits to oncologic patients, as evidenced by inducing a regression of metastatic lesions in triple-negative breast cancer and extending progression free time in drug-resistant squamous cell carcinoma [33].
CSC - Signaling Inhibitors
The phosphatidylinositol-3-kinase (PI3K)/Akt/mTOR signaling pathways are frequently activated in a number of cancer types, and play a master regulating role in many aspects of onco-pathogenesis, such as proliferation/survival, angiogenesis, metabolism and differentiation [5, 34]. Moreover, activation of mTOR complex has been linked to tumorigenicity of glioblastoma stem-like cells, ALDH1 activity in colorectal CSCs, epithelial-mesenchymal transition (EMT) in prostate cancer, and resistance to conventional medicines [12, 34]. In this regard, PI3K/mTOR cascade is emerging as one of the attractive targets for pharmaceutical innovation, and a few mTOR inhibitors have so far been approved by FDA of USA to treat renal cell cancer. In particular, everolimus appeared to confer better overall survival (OS) benefits than tersirolimus, to progressed renal cell carcinoma [35].
Binding of cytokines, such as interleukine-6 (IL-6), to their cognate receptors activates JAK-STAT signaling network, which in turn promotes certain malignant behaviors and therapeutic resistance in an array of tumor types [13, 17, 36]. In particular, Stat3 has been noticed to enhance survival and proliferation of CSCs in breast, colon and prostate, while IL-6 was revealed to augment cancer cell resistance to conventional treatments through activating cell cycle-regulating proteins [14, 17]. Interestingly, tocilizumab, an IL-6 blocking antibody originally approved for treatment of auto-immunity-mediated inflammatory disorders, appeared to be capable of improving therapeutic outcomes of progressed malignancies in the clinic [37]. Moreover, the JAK inhibitor ruxolitinib has been recently shown to deliver a survival benefit to the patients with metastatic pancreatic cancer [38].
Wnt/-catenin, Hedgehog and Notch signaling cascades represent three of the fundamental regulating pathways for proper embryonic development, and are physiologically inactivated in most adult tissues except maintenance of certain normal stem cells [14]. To date, hyper-activities of these signaling events have been increasingly identified in CSCs, and linked to therapeutic resistance and metastasis, in a variety of malignant disorders including breast, colon and pancreatic cancers [5, 9, 12]. Intriguingly, niclosamide, a traditional anti-helminthic medicine, has been rediscovered to suppress several CSC-signaling pathways such as Wnt/β-catenin, STAT3 and mTOR, therefore diminishing cancer metastasis [17, 39]. On the other hand, vismodegib, a hedgehog inhibitor approved for basal cell carcinoma, has been demonstrated to improve clinical outcomes of patients with medulloblastoma [40]. Lately, an antibody-drug conjugate rovalpituzumab tesirine (SC16LD 6.5) targeting the Notch activator delta-like protein 3 (DLL3) has been noticed to exert an impressive response rate in the patients with refractory / drug-resistant small-cell lung cancer in a phase 1 clinical trial [41].
Chemokine CXCL12 produced by the stromal tissue recruits the responding receptor CXCR4-expressing cancer cells through chemo-attraction, thereby promoting malignant cell migration and metastasis [21]. While CXCL12 protein appears highly expressed in organs that are noticed to be the common sites of malignant metastasis including liver, lung and bone marrow, CXCR4 is significantly up-regulated in CSCs of a wide variety of neoplasms, such as CD44+/CD24- cells and CD133+ cells in breast and pancreatic cancers, respectively [11, 12]. In this regard, plerixaflor, a CXCR4 inhibitor initially approved to mobilize hematopoietic stem cells to the peripheral blood for collection and subsequent autologous transplantation, has recently been revealed to re-sensitize refractory leukemic cells to the chemotherapy, and therefore improve an overall complete remission [42].
Herb Medicines
Ginseng (Ren-shen) represents one of the most popularly used herb medicines in the clinic, exerting a wide array of therapeutic effects including immune modulation, anti-oxidation, anti-inflammation, and anti-oncogenesis [43]. In particular, ginseng has been utilized to prevent the occurrence or recurrence of several gastroenterological cancers, and to minimize toxicities of traditional radio-/chemo-therapies in clinical oncology [44]. Impressively, ginseng extracts, confer numerous biological effects, of which ginsenoside Rg3 inhibits NF-kB and in turn down-regulates a number of pro-survival proteins including Bcl-2 and cyclin D1, whereas ginsenoside Rh1 diminishes JAK1-STAT3 signaling activities. In addition, ginseng extracts can also enhance the sensitivity of malignant cells to several anti-cancer compounds via suppressing MDR gene expression [43].
Turmeric (Jiang-huang) represents an herbaceous plant of the ginger family which has been historically used to treat inflammatory disorders in Asia [44, 45]. As the major active compound in Turmeric, curcumin is a traditionally known cooking spice, and intriguingly able to exert a number of pharmacological efficacies against several pathological conditions of human [45]. Particularly, curcumin has been recently noticed to deliver clinical benefits to the patients with some types of malignancies such as enhancing progression free survival (PFS) in pancreatic cancer and improving histological grades bladder cancer [46]. The potential anti-cancer mechanisms by curcumin impact on many facets of onco-pathogenesis including inhibition of cyclin D1, STAT3 and vascular endothelial growth factor (VEGF) [45]. Moreover, it has been revealed that curcumin reduces malignant metastasis depending upon suppressing CSCs in breast cancer [47].
Shenqi fuzheng (SQFZ) injection, an herbal formula consisting of Radix astragali (Huang-qi) and Codonopsis pilosula (Dan-shen), has been approved by China’s FDA to treat several major chronic diseases including cancer. The clinical trials have demonstrated that SQFZ improved response rates and alleviated toxicities upon chemo-/radio-therapies in the patients with advanced cancers of lung, breast, colon, and others [44, 45]. The therapeutic mechanisms of active components in this herb formula are complex, and appear going through at least two aspects of augmenting antitumor immunity as well as inhibiting CSC-linked phenotypes. In particular, extracts of Radix astragali was noticed to inhibit lung cancer cell migration via down-regulating NF-kB signaling and IL-6 production [48]. On the other hand, Codonopsis pilosula extracts were revealed to suppress invasion, migration and the CSC marker protein (CD44) expression in ovarian cancer cells [49].
Yangzheng Xiaoji (YZXJ) capsule was developed from a traditional Chinese medicine formula composed of 16 herbs including Radix astragali, Ginseng, among others. To date, YZXJ has been able to deliver clinical benefits to patients with liver, breast, lung and gastrointestinal cancers, as evidenced by improving therapeutic efficacies and reducing adverse events of existing anti-cancer treatments [17, 44]. Whereas the underlying mechanisms of action for YZXJ are yet to be well defined, emerging data support its multiple targeting effects on many aspects of cancer biology. Impressively, it has been revealed that YZXJ diminishes tumor growth and angiogenesis, via down-regulating hepatocyte growth factor (HGF)/c-MET signaling in malignant cells and focal adhension kinase (FAK) activity in endothelial cells [44, 50]. Moreover, YZXJ appears to suppress some CSC-associated pathological processes such as invasion and migration of cancer cells upon inhibiting PI3K/AKT signaling cascade [51].
Perspective
A growing body of evidence demonstrates that oncologic disease is highly heterogeneous at various biological levels, in which CSCs fundamentally drive intra-tumor heterogeneity [1, 5]. Although it has been two decades since the first CSC subpopulation was identified from human leukemia, CSC theory is so far still facing some challenges that need to be solved, such as the precise origin of CSCs and more specific/functional biomarkers [9, 12]. However, there has been a common sense that CSC research will not only confer a better understanding of onco-pathogenesis, but also more importantly wave deep implications in clinical management of oncology. It is well conceived that eliminating CSCs can significantly improve therapeutic outcomes of existing treatments for cancer patients through overcoming drug-resistance and diminishing metastasis/recurrence, to optimally cure cancer [6, 21].
As a recently highlighted concept, precision medicine takes the advantages of selective biomarkers to predict therapeutic sensitivity, and thus enhances the likelihood of right drug(s) for each individual patient [17]. Accordingly, it should be noted that the coverage of surrogate biomarkers needs to go beyond rapidly dividing cells which are the dominant population in a tumor bulk, and to capture CSC signatures which are poorly represented in a whole cancer tissue genome [6]. In this regard, alternative sample sources such as circulating tumor cells and gene/micro-RNA profiling in combination with the clinical situations appear capable of conveniently giving additional information regarding prognosis and therapeutic response [52-54]. Not surprisingly, personalized anti-CSC medicines are increasingly of interest to clinical oncology and pharmaceutical innovation, in order to maximize efficacious outcomes of the existing therapeutic approaches in clinical oncology.
Anti-CSC strategy holds a promise to come up with smarter weapons to support human’s defensive war against cancer. Whereas the known CSC biomarkers are only relatively specific and the comprehensive regulatory machinery of CSC dynamic is yet to be well established, the innovative approaches of highly selective targeting CSCs, such as blocking the cell surface biomarkers or inducing mature differentiation, are still in their infancy far from reaching the clinical practice [6, 8, 12]. To circumvent this issue, we have instead sorted out those anti-CSC medicines clinically available, which are intriguingly from drug repositioning, stemness-associated signaling inhibitors and herb remedies, respectively (Table 1). Hence, insights derived herein renew a lesson that serendipitous/ clinical observations and disease biology-driven innovation can still inspire us with a productive portfolio to advance the therapeutic means against cancer and perhaps beyond [21, 55].
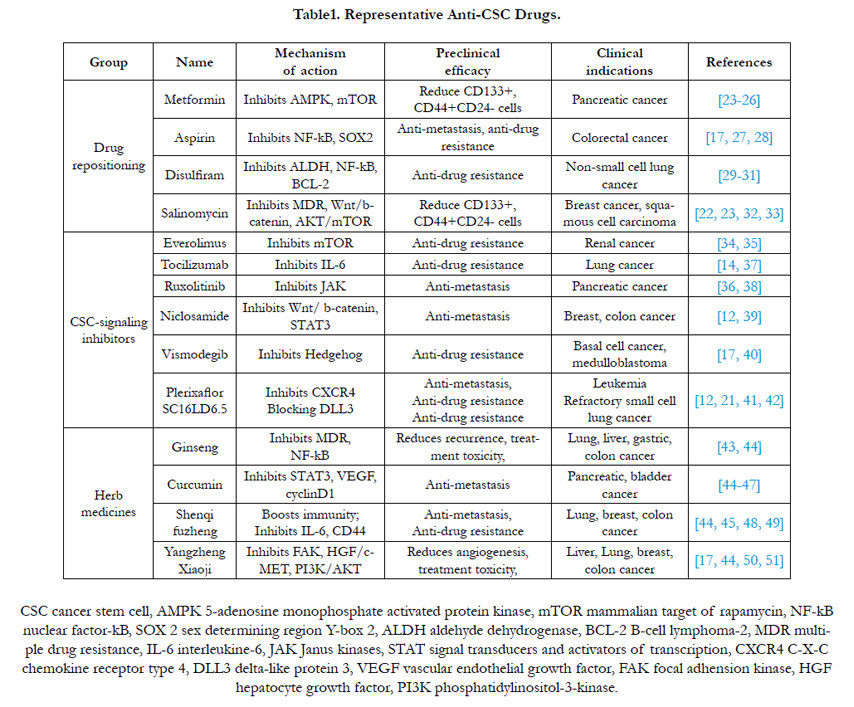

Table1. Representative Anti-CSC Drugs.
References
- Turner NC, Reis-Filho JS (2012) Genetic heterogeneity and cancer drug resistance. Lancet Oncol. 13: e178-185.
- Huang M, Shen A, Ding J, Geng M (2041) Molecularly targeted cancer therapy: some lessons from the past decade. Trends Pharmacol Sci. 35(1): 41-50.
- Fisher R, Pusztai L, Swanton C (2013) Cancer heterogeneity: implications for targeted therapeutics. Br J Cancer. 108(1): 479-85.
- Almendro V, Marusyk A, Polyak K (2013) Cellular heterogeneity and molecular evolution in cancer. Annu Rev Pathol. 8: 277-302.
- Saunders NA, Simpson F, Thompson EW, et al., (2012) Role of intratumoural heterogeneity in cancer drug resistance: molecular and clinical perspectives. EMBO Mol Med. 4(8): 675-684.
- Grotenhuis BA, Wijnhoven BP, van Lanschot JJ (2012) Cancer stem cells and their potential implications for the treatment of solid tumors. J Surg Oncol. 106(2): 209-215.
- Bonnet D, Dick JE (1997) Human acute myeloid leukemia is organized as a hierarchy that originates from a primitive hematopoietic cell. Nat Med. 3: 730-737.
- Yang T, Rycaj K, Liu ZM, Tang DG (2014) Cancer stem cells: constantly evolving and functionally heterogeneous therapeutic targets. Cancer Res. 74(11): 2922-2927.
- Chen D, Bhat-Nakshatri P, Goswami C, Badve S, Nakshatri H (2013) ANTXR1, a stem cell-enriched functional biomarker, connects collagen signaling to cancer stem-like cells and metastasis in breast cancer. Cancer Res. 73(18): 5821-533.
- Chen LS, Wang AX, Dong B, Pu KF, Yuan LH, et al., (2012) A new prospect in cancer therapy: targeting cancer stem cells to eradicate cancer. Chin J Cancer. 31(12): 564-572.
- Wang T, Shigdar S, Gantier MP, Hou Y, Li Y, et al., (2015) Cancer stem cell targeted therapy: progress amid controversies. Oncotarget. 6(42): 44191- 44206.
- Klonisch T, Wiechec E, Hombach-Klonisch S, Ande SR, Wesselborg S, et al., (2008) Cancer stem cell markers in common cancers - therapeutic implications. Trends Mol Med. 14(10): 450-460.
- Sansone P, Bromberg J (2012) Targeting the interleukin-6/Jak/stat pathway in human malignancies. J Clin Oncol. 30(9): 1005-1014.
- Hadjimichael C, Chanoumidou K, Papadopoulou N, Arampatzi P, Krestsovali A, et al., (2015) Common stemness regulators of embryonic and cancer stem cells. World J Stem Cells. 7: 1150-1184.
- Jin X, Yin J, Kim SH, Sohn YW, Beck S, et al., (2011) EGFR-AKT-Smad signaling promotes formation of glioma stem-like cells and tumor angiogenesis by ID3-driven cytokine induction. Cancer Res. 71(22): 7125-7134.
- Codony-Servat J, Verlicchi A, Rosell R (2016) Cancer stem cells in small cell lung cancer. Transl Lung Cancer Res. 5(1): 16-25.
- Chen D, Zhang X (2015) Tipping tumor microenvironment against drug resistance. J Oncol Trans Res. 1: 1-5.
- Chen S, Hou JH, Feng XY, Zhang XS, Zhou ZW, et al., (2013) Clinicopathologic significance of putative stem cell marker, CD44 and CD133, in human gastric carcinoma. J Surg Oncol. 107(8): 799-806.
- Cojoc M, Peitzsch C, Trautmann F, Polishchuk L, Telegeev GD, et al., (2013) Emerging targets in cancer management: role of the CXCL12/CXCR4 axis. Onco Targets Ther. 6:1347-1361.
- Dave B, Mittal V, Tan NM, Chang JC (2012) Epithelial-mesenchymal transition, cancer stem cells and treatment resistance. Breast Cancer Res. 14(1):202.
- Chen DH, Zhang XS (2015) Targeted therapy: resistance and re-sensitization. Chin J Cancer. 34(11): 496-501.
- Alisi A, Cho WC, Locatelli F, Fruci D (2013) Multidrug resistance and cancer stem cells in neuroblastoma and hepatoblastoma. Int J Mol Sci. 14(12): 24706-24725.
- Würth R, Barbieri F, Florio T (2014) New molecules and old drugs as emerging approaches to selectively target human glioblastoma cancer stem cells. Biomed Res Int. 2014:126586.
- Del Barco S, Vazquez-Martin A, Cufí S, Oliveras-Ferraros C, Joven J, et al., (2011) Metformin: multi-faceted protection against cancer. Oncotarget. 2(12): 896-917.
- Chae YK, Arya A, Malecek MK, Shin DS, Chandra S, et al., (2016) Repurposing metformin for cancer treatment: current clinical studies. Oncotarget. 10: 18632.
- Ambe CM, Mahipal A, Fulp J, Chen L, Malafa MP (2016) Effect of Metformin Use on Survival in Resectable Pancreatic Cancer: A Single-Institution Experience and Review of the Literature. PLoS One. 11(3): e0151632.
- Zhang Y, Liu L, Fan P, Bauer N, Gladkich J, et al., (2015) Aspirin counteracts cancer stem cell features, desmoplasia and gemcitabine resistance in pancreatic cancer. Oncotarget. 6(12): 9999-10015.
- Crawford S (2013) Is it time for a new paradigm for systemic cancer treatment? Lessons from a century of cancer chemotherapy. Front Pharmacol. 4: 68.
- Triscott J, Rose Pambid M, Dunn SE (2015) Concise review: bullseye: targeting cancer stem cells to improve the treatment of gliomas by repurposing disulfiram. Stem Cells. 33(4): 1042-1046.
- P Liu, IS Kumar, S Brown, Tawari PE, Tang JZ, et al., (2013) Disulfiram targets cancer stem-like cells and reverses resistance and cross-resistance in acquired paclitaxel-resistant triple-negative breast cancer cells. Br J Cancer. 109: 1876–1885.
- Nechushtan H, Hamamreh Y, Nidal S, Baron A, Shalev YI, et al., (2015) A phase IIb trial assessing the addition of disulfiram to chemotherapy for the treatment of metastatic non-small cell lung cancer. Oncologist. 20(4):366-367.
- Shi AM, Tao ZQ, Li H, Wang YQ, Zhao J (2015) Cancer stem cells targeting agents--a review. Eur Rev Med Pharmacol Sci. 19(21): 4064-4067.
- Naujokat C, Steinhart R (2012) Salinomycin as a drug for targeting human cancer stem cells. J Biomed Biotechnol. 2012: 950658.
- Xia P, Xu XY (2015) PI3K/Akt/mTOR signaling pathway in cancer stem cells: from basic research to clinical application. Am J Cancer Res. 5(5): 1602-1609.
- Patel SB, Stenehjem DD, Gill DM, Hsu J, Pal SK, et al., (2016) Everolimus Versus Temsirolimus in Metastatic Renal Cell Carcinoma After Progression With Previous Systemic Therapies. Clin Genitourin Cancer. 14(2): 153-159.
- Eichten A, Su J, Adler A, Loffe E, Zhang L, et al., (2016) Resistance to anti- VEGF therapy mediated by autocrine IL-6/STAT3 signaling and overcome by IL-6 blockade. Cancer Res. 76(8): 2327-2339.
- Ando K, Takahashi F, Kato M, Kaneko N, Ohe K, et al., (2014) Tocilizumab, a proposed therapy for the cachexia of Interleukin6-expressing lung cancer. PLoS One. 9(7): e1024.
- Hurwitz HI, Uppal N, Wagner SA, Bendell JC, Sandor V, et al., (2015) Randomized, double-blind, phase II study of ruxolitinib or placebo in combination with capecitabine in patients with metastatic pancreatic cancer for whom therapy with gemcitabine has failed. J Clin Oncol. 33(34): 4039-4047.
- Pan JX, Ding K, Wang CY (2012)0 Niclosamide, an old antihelminthic agent, demonstrates antitumor activity by blocking multiple signaling pathways of cancer stem cells. Chin J Cancer. 31(4): 178-184.
- Robinson GW, Orr BA, Wu G, et al., (2015) Vismodegib exerts targeted efficacy against recurrent sonic hedgehog-subgroup medulloblastoma: results from phase II pediatric brain tumor consortium studies PBTC-025B and PBTC-032. J Clin Oncol. 33(24): 2646-2654.
- Dylla SJ (2016) Toppling high-grade pulmonary neuroendocrine tumors with a DLL3-targeted trojan horse. Mol Cell Oncol. 3(2): e1101515.
- Uy GL, Rettig MP, Motabi IH, McFarland k, Vij R, et al., (2012) A phase 1/2 study of chemosensitization with the CXCR4 antagonist plerixafor in relapsed or refractory acute myeloid leukemia. Blood. 119(17): 3917-3924.
- Chen S, Wang Z, Huang Y, Wong RA, Chow MS, et al., (2014) Ginseng and anticancer drug combination to improve cancer chemotherapy: a critical review. Evid Based Complement Alternat Med. 2014: 16894.
- Ye L, Jia Y, Ji KE, Sanders AJ, Xue KAN, et al., (2015) Traditional Chinese medicine in the prevention and treatment of cancer and cancer metastasis. Oncol Lett. 10(3): 1240-1250.
- Qi F, Zhao L, Zhou A, Zhang B, Li A, et al., (2015) The advantages of using traditional Chinese medicine as an adjunctive therapy in the whole course of cancer treatment instead of only terminal stage of cancer. Biosci Trends.9(1): 16-34.
- Hosseini A, Ghorbani A (2015) Cancer therapy with phytochemicals: evidence from clinical studies. Avicenna J Phytomed. 5:84-97
- Charpentier MS, Whipple RA, Vitolo MI, Boggs AE, Slovic J, et al., (2014) Curcumin targets breast cancer stem-like cells with microtentacles that persist in mammospheres and promote reattachment. Cancer Res. 74(4): 1250-1260.
- Cheng X, Gu J, Zhang M, Yuan J, Zhao B, et al., (2014) Astragaloside IV inhibits migration and invasion in human lung cancer A549 cells via regulating PKC-α-ERK1/2-NF-κB pathway. Int Immunopharmacol. 23(1): 304-313.
- Xin T, Zhang F, Jiang Q, Chen C, Li Y, et al., (2012) The inhibitory effect of a polysaccharide from Codonopsis pilosula on tumor growth and metastasis in vitro. Int J Biol Macromol. 51(5): 788-793.
- Jiang WG, Ye L, Ruge F, Owen S, Martin TH, et al., (2015) YangZheng XiaoJi exerts anti-tumour growth effects by antagonising the effects of HGF and its receptor, cMET, in human lung cancer cells. J Transl Med. 13: 280.
- Ye L, Ji K, Frewer N, Ji J, Jiang WG, et al., (2012) Impact of Yangzheng Xiaoji on the adhesion and migration of human cancer cells: the role of the AKT signalling pathway. Anticancer Res. 32(7): 2537-2543.
- Mitra A, Mishra L, Li S (2015) EMT, CTCs and CSCs in tumor relapse and drug-resistance. Oncotarget. 6(13): 10697-10671.
- Marín-Aguilera M, Reig Ò, Lozano JJ, Jimenez N, Erill N, et al., (2015) Molecular profiling of peripheral blood is associated with circulating tumor cells content and poor survival in metastatic castration-resistant prostate cancer. Oncotarget. 6(12): 10604-10616.
- Chen D, Goswami CP, Burnett RM, Anjanaapa M, Muller W, et al., (2014) Cancer affects microRNA expression, release, and function in cardiac and skeletal muscle. Cancer Res. 74(16): 4270-4281.
- Hargrave-Thomas E, Yu B, Reynisson J (2012) Serendipity in anticancer drug discovery. World J Clin Oncol. 3(1): 1-6.





