Trend of Cancer Incidence in an Oncology Centre in Nigeria
Sowunmi AC1*, Alabi AO1, Fatiregun OA2, Olatunji TA1, Okoro US1, Durosinmi-Etti FA1
1 Department of Radiotherapy, Lagos University Teaching Hospital, Idi-araba, Lagos, Nigeria.
2 Oncology Unit, Department of Radiology, Lagos State University Teaching Hospital, Lagos, Nigeria.
*Corresponding Author
Sowunmi Anthonia C,
Department of Radiotherapy, Lagos University Teaching Hospital,
Idi-araba, Lagos, Nigeria.
Tel: +234 8037216723
E-mail: asowumi@unilag.edu.ng and toniasow@yahoo.com
Received: June 03, 2016; Accepted: June 09, 2016; Published: June 13, 2016
Citation: Sowunmi AC, et al., (2016) Trend of Cancer Incidence in an Oncology Centre in Nigeria. J Translational Clin Exp Oncology. 1(1), 1-5.
Copyright: Sowunmi AC© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Globally, 24.6 million people live with cancer of which 6.7 million deaths occur annually and 10.9 million new cases are recorded every year. World Health Organization (WHO) reported that 12.5% of all deaths are attributable to cancer and if the trend continues, it is estimated that by 2020, 16 million new cases will be diagnosed per annum out of which 70% will be in developing countries. Cancer is the second most common cause of death in developed countries following cardiovascular disease. The percentage increase in cancer in many African countries is higher than developed countries this can be attributed to lack of awareness about the risk factors and changes in lifestyle. The most common cancer diagnosed worldwide is lung (1.8 million, 13%) breast (1.7million 11.9%) and colorectal (1.4 million, 9.7%), while the most common causes of cancer deaths are lung (1.6 million, 19.4%), liver (0.8 million, 9.1%) and stomach (0.7 million, 8.8%), due to growth and ageing of the global population.
Aim and Objectives: To review the trend of cancer incidence in Lagos University Teaching Hospital (LUTH) from January 2004 – December 2013.
Methodology: This is a retrospective study of histologically confirmed malignancies seen at the Department of Radiotherapy, LUTH from January 2004 – December 2013. Case files were retrieved through the record department and the information required was extracted with the aid of a data extraction form.
Results: A total of 3,314 new cases of cancer were recorded in LUTH during the study period. The mean age of cancer presentation is 48.52(+/- 16.44). The median age is 49.00 years with an age range of 1-100 years. The peak age incidence for males was 50-54 years accounting for 10% of all male presentation while females had a peak age incidence of 40-44 years accounting for 14% of female cases. The male to female ratio was 1:3. Breast cancer was the most common cancer (38.1%) followed by cervical cancer (17.0%) and colorectal cancer (3.3%). Prostate cancer, eye cancer and ovarian cancer accounted for 3.1%, 2.0% and 1.4% respectively. In males, the commonest cancer was prostate cancer (12.8%) followed by colorectal cancer (4.5%).
Conclusion: Generally, cancer incidence in Nigeria appears low compared to developed countries, which may not truly reflect the burden of the disease. This could be due to poor population based statistics and poor health patronage of orthodox medical care.
2.Introduction
3.Material and Methods
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Trend; Cancer; Incidence; Nigeria.
Introduction
Globally, 24.6 million people live with cancer, out of this, 6.7 million deaths occur with 10.9 million new cases recorded every year [1]. World Health Organization (WHO) reported that 12.5% of all deaths are attributable to cancer and if the trend continues, it is estimated that by 2020, s16 million new cases will be diagnosed per annum out of which 70% will be in developing countries [2]. Cancer is the second most common cause of death in developed countries following cardiovascular disease, as population aging continues in many countries, cancer will remain a major health problem around the globe as elderly peoples are most susceptible to cancer [2, 3]. The percentage increase in cancer in many African countries is higher than in developed countries this can be attributed to lack of awareness about the risk factors and changesin lifestyle [1]. GLOBOCAN burden rises to 14.1 million new cases and 8.2 million cancer deaths in 2012 compared with 12.7 million new cases and 7.6 million cancer deaths in 2008 [3]. The most common cancer diagnosed worldwide is Lung (1.8 million, 13%), Breast (1.7 million 11.9%) and Colorectal (1.4 million, 9.7%) while the most common cause of cancer deaths were Lung (1.6 million, 19.4%), Liver (0.8 million, 9.1%) and Stomach (0.7 million, 8.8%) due to growth and ageing of the global population [3]. A projection of 19.3 million new cancer cases per year for 2025 has been predicted by GLOBOCAN 2012 [3].
The burden of cancer in Nigeria is unknown due to improper data from poor funded Cancer Registries that produce hospital based data as well as missed diagnosis [1]. Elima et al., in their population based cancer registries from Ibadan and Abuja reported age standardized incidence rate (ASR) for all invasive cancer as 66.4 per 100,000 men and 130.6 per 100,000 women in the Ibadan Population Based Cancer Registry (IBCR) and 58.3 per 100,000 men and 138.6 per 100,000 women in Abuja Population Based Cancer Registry (ABCR) [4]. The earliest report from IBRC by Edington and Maclean in 1960 – 1969 was ASR of 105.1 and 78 per 100,000 females and males respectively [5]. In 1998, Thomas et al., reported 74.5 and 63.9 per 100,000 for female and male respectively [6]. IBCR (2001-2005) reported 115.1 and 81.6 per 100,000 in female and male respectively [7] while ABCR (2009 – 2010) reported 130.6 and 66.4 per 100,000 female and male respectively [4]. In Ghana, ASR was 89.1 and 104.1 per 100,000 for males and female [8]. The mortality rates in Nigeria recorded by WHO from all sites of cancer in 2002 were 72.2% and 76% for male and female respectively [8].
In United kingdom where population based cancer registries have 100% geographic coverage, and effect follow-up mechanisms is in place, 412 and 335 per 100,000 in male and female respectively between 1993 – 1995 and 409 and 348 per 100,000 in male and female respectively were reported between 2002 – 2004 [9]. The aim of this study was to review the trend of cancer incidence in Lagos University Teaching Hospital (LUTH) from January 2000 – December 2014.
Material and Methods
This is a retrospective study of all patients with histologically confirmed malignancies listed in the medical records register and seen at the Department of Radiotherapy, LUTH from January 2004 – December 2013. Case files were retrieved through the record department and the information required was extracted with the aid of a data extraction form. All possible information including patients’ age, sex, occupation, marital status, ethnic group and histology were evaluated. Statistical analysis was done using the SPSS (version 21) program. Analyzed data is presented in the form of frequency tables, charts and cross tabulations. Ethical approval was obtained from the Ethics and Research committee of LUTH, Lagos State where the study was done.
Results
A total of 3,314 new cases of cancer were recorded in Lagos University Teaching Hospital from January 2004 to December 2013.
The highest incidence of 435 new cases was seen in 2005 followedby 429 new cases in 2013 and the third highest incidence of 348 new cases in 2006. The lowest number was 260 cases in 2008 (Figure 1).
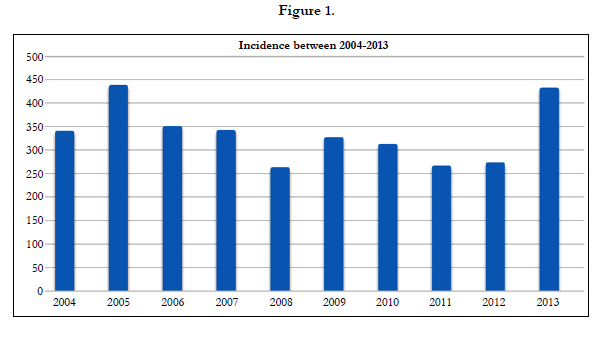
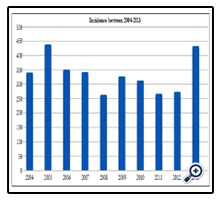
Figure 1
The mean age of cancer presentation is 48.52 (+/- 16.44). The median age is 49.00 years with an age range of between 11months to - 96 years. The peak age incidence for males was 50-54 years accounting for 80 (10%) of all male presentation followed by 60-64 years which accounted for 69 (9%) patients and third highest age incidence in male was between 30-34 years where 64 (8%) were reported. For females, the peak age incidence was 40-44 years accounting for 350 (14%) female new cases. This was followed by 50-54 years where 302 (12%) new female cases were reported and 30-34 years which accounted for 277 (11%) new cases of female cancer presentation (Figure 2).
Figure 2
2,519 (76%) new cases recorded during the period of study were females while 795 (24%) were males, with a male to female ratio of 1:3 (Figure 3). The combined age standardized incidence rate (ASR) for all cancers in males and females were 55.8 and 189.9 per 100 000 respectively.
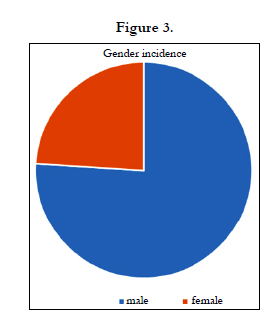
Figure 3
2,459 (74.2%) of patients that presented with cancer within the period under study were married and 456 (13.8%) patients were single. 399 (12.0%) patients were either widowed or separated.
Breast cancer was the most common cancer presentation for both female and males under the period of study accounting for 1263 (38.1%) of patients, cervical cancer was the second most common with 563 (17.0%.) new cases. Colorectal cancer was the third most common accounting for 109 (3.3%) of all cancer presentations. Prostate cancer, eye cancer and ovarian cancer accounted for 103 (3.1%), 66 (2.0%) and 47 (1.4%) of the new cases respectively (Figure 4).
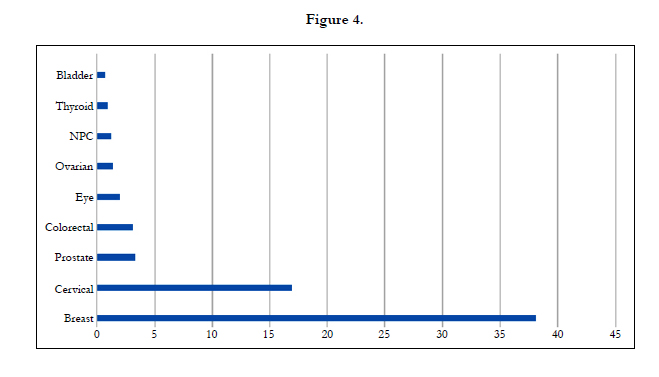
Figure 4
In terms of gender distribution, for males the commonest cancer was Prostate cancer with 12.8% of all presentation, followed by Colorectal cancer 4.5%. Nasopharyngeal cancer and Eye cancer are the third and fourth most common cancer in males accounting for 3.5% and 3.3% of all male cancer presentation. The least common male cancer was parotid and thyroid cancer at 1.5% respectively (Figure 5).
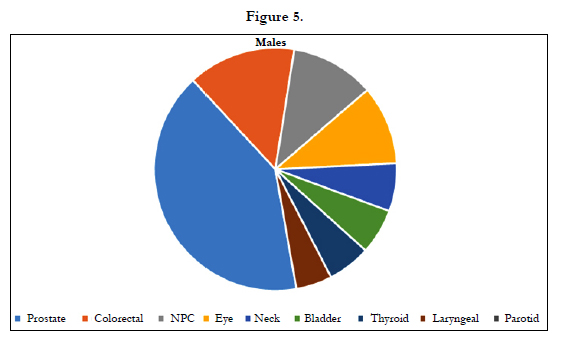
Figure 5
Breast cancer is the most common cancer in females accounting for 49.9%, followed by cervical cancer in 22.4%, others are ovarian 21.9% and colorectal 2.3%. Liver cancer was the least common cancer 1.4% (Figure 6).
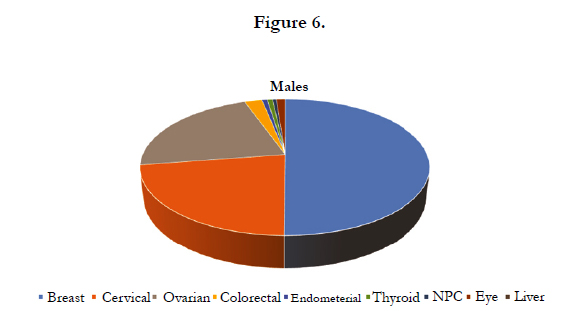
Figure 6
Discussion
Cancer is a global health issue and it is the most common noncommunicable disease. Approximately one third of it is preventable, another third are potentially curable if detected early and the remaining third incurable but managed with palliative care in order to improve quality of life [1]. The incidence of cancer in Nigeria and indeed Africa varies remarkably from that of the rest of the world especially the economically developed countries since only about 1% of worldwide cancer data comes from Africa [10]. This could be due to poor population based statistic and poor health patronage of orthodox medical care [10]. This trend was noted in the number of new cases reported annually in the period being investigated.
The gender incidence of cancer, male to female ratio of 1:3 noted in this study is consistent with a similar study conducted by Elima Jedi-Agba et al in Ibadan and Abuja who reported M: F ratio of 1:2 in both centers [4]. The combined age standardized incidence rate (ASR) for all cancers in males and females were 55.8 and 189.9 per 100 000 respectively.
Anyanwu S.N et al., reported similar findings in Eastern Nigeria of 1:3 which also correlates with the WHO estimated incidence of cancer from all sites in 2002 for Nigeria which was 90.7 and 100.9 per 10,000 for males and females respectively [4, 11]. This is comparable to 89.1 and 104.1/100,000 incidence for males and females and 72.2 and 79.6 crude mortality rates recorded for Ghana [5, 10] but much less than figures recorded for United Kingdom and USA [1].
Generally, cancer incidence in Nigeria appears low compared to developed countries which may not truly reflect the burden. Similar to reports from other parts of the world, it is slightly higher in female, and this may be due to their increased interaction of the health care system i.e. uptake of maternal and child health services, greater population awareness of breast and cervical cancers, better health seeking behavior of women compared to men [12] .
The mean age of 48.52(+/- 16.44) at presentation reported in this study was consistent with similar studies in Lagos by AbdulKareem F. (2009) [12] who reported 49.67(+/- 18.79) however this was lower than that reported by the UK NCI EGRP (2012) [2] for Europe and North America who had mean age of 52.9(16-0). This difference could due to early detection programs and overall better medical services [2].
Breast cancer and Cervical cancer are the commonest cancers in LUTH during the period of this study accounting for 1263 (38.1%) and 563 (17%.) new cases. Prostate cancer was the commonest for men accounting for 424 (12.8%) cases, this was consistent with the results from Ibadan and Abuja cancer registries in 2009 of 40.8%, 24% and 21.7% incidence respectively [3]. This reports appear higher than GLOBOCAN estimates for breast cancer for the whole country which for the period of 1998-2000 is 32.9% [1]. This increasing incidence may be due to improved diagnosis, better access to care and better case reporting [3]. Globally, statistics have shown that the annual incidence of Breast cancer is increasing especially in countries with previous low incidence rates [1].
Carcinoma of the Cervix is second most common cancer noted in the study which is the consistent with the trend reported by Popoola A.O et al., (2013) as well consistent with the GLOBACAN statistics for 2008 reports of 26.7%, [13]. The high incidence of Cervical cancer has been attributed to poor awareness about the risk factors and change in lifestyle. In addition, poor compliance for screening participation and follow up for abnormalities detected is also a major challenge.
Worldwide, incidence and mortality from cervical cancer are second only to breast cancer, and in parts of the developing world, cervical cancer is the major cause of death in women of reproductive age [10]. This geographical disparity is related to the absence of effective screening programs, late presentation and lack of treatment facilities. Epidemiologic and biological studies have not shown significant differences in tumor biology in countries with high rates of cervical cancer [15].
Prostate cancer is the third most common malignancy and the most common cancer in men in Lagos which is similar to figures from Ibadan and Abuja cancer registries [3]. This is similar to reports from other African countries such as Ghana and Tanzania [8, 14] but at variance with cancer incidence studies in Western Europe and America which rated lung cancer as the most common cancer [14]. This can be related to the high incidence of smoking.
Conclusion
Generally, cancer incidence in Nigeria appears low compared to developed countries which may not truly reflect the burden of the disease. This could be due to poor population based statistics and poor health patronage of orthodox medical care.
References
- Akinkugbe OO, Lucas AO, Onyemelukwe GC, Yahaya H, Saka MJ (2010) Non-communicable Diseases in Nigeria: The coming epidermic. Nigerian Health review, Health Reform Foundation of Nigeria (HERFON). 1-25.
- World Health Organization and International Union Against Cancer (2005) Global Action on Cancer-Update version. Geneva 12.
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R,Eser S, et al. (2013) GLOBOCAN 2012 v1.0: Cancer Incidence and Mortality Worldwide. International Agency for Research on Cancer ,Lyon, France.
- Elima JA, Maria PC, Olufemi O, Emmanuel O, Toyin F,Festus I et al., (2012) Cancer Incidence in Nigeria: a report from population-based cancer registries. Cancer Epidemiol 36(5): e271–e278. doi:10.1016/j.canep.2012.04.007.
- Edington GM, Maclean CMV (1965) A cancer rate survey in Ibadan, western Nigeria, 1960-1963. Br. J. Cancer 19(3): 471-481.
- Thomas JO, Aghadiuno PU (1998) Ibadan Cancer Registry, 1985-1992, International incidence of childhood cancer.IARC scientific publication. Lyon 2 : 43-5.
- Ibadan Cancer Registry Data (2001–2005), University College Hospital, Ibadan, Nigeria.
- Naader SB, Archampong EQ (1994) Cancer of the colon and rectum in Ghana: A five year prospective study. BJ of Surg 81(3): 456-459.
- Susan W, Nicola C (2008) Cancer incidence and mortality: trends in the United Kingdom and constituent countries, 1993 to 2004. Office of National Statistics of UK, Health statistics quarterly . 33-46.
- Howlader N, Noone AM, Krapcho M, Neyman N, Aminou R, et al. (2011) SEER Cancer Statistics Review, 1975-2008. National Cancer Institute, Bethesda.
- Anyanwu SN (2000) Breast cancer in Eastern Nigeria: A ten year review. West Afr J Med 19(2): 120-125.
- Fatimah Abdulkareem (2009) Epidemiology and Incidence of Common Cancers in Nigeria. Cancer Reg & Epid wkshop 1-58.
- Popoola AO , Omodele FO , Oludara MA , Ibrahim NA , Igwilo AI , et al., (2013) Prevalence and Pattern of Cancers among Adults Attending a tertiary Health Institution in Lagos, Nigeria. IOSR-JMDS 6(3): 68-73.
- Hsing AW, Tsao L, Devesa SS (2000) International trends and patterns of prostate cancer incidence and mortality. Int J Cancer 85(1): 60-67.
- Janicek MF, Averette HE (2001) Cervical cancer: Prevention, Diagnosis and Therapeutics. CA Cancer J Clin 51(2): 91-114.





