Metastatic Adenocarcinoma of Unknown Primary Origin Presenting with Severe Lumbar Neuropathic Pain in a Dog
Menchetti M*, Sabattini S, Gandini G, Gagliardo T, Ruffini A, Asti M, Bettini G
Department of Veterinary Medical Sciences (UNI EN ISO 9001:2008), University of Bologna, Ozzano dell’Emilia (BO), Italy.
*Corresponding Author
Marika Menchetti,
Department of Veterinary Medical Science,
University of Bologna, Ozzano dell’Emilia (BO), 40064, Italy.
Tel: +39/051/2097431
Fax: +39/051/2097687
E-mail: marika.menchetti3@unibo.it
Received: October 01, 2015; Accepted: October 28, 2015; Published: November 02, 2015
Citation: Menchetti M, et al., (2015) Metastatic Adenocarcinoma of Unknown Primary Origin Presenting with Severe Lumbar NeuropathicPain in a Dog. Int J Vet Health Sci Res. 3(7), 70-74. doi: dx.doi.org/10.19070/2332-2748-1500018
Copyright: Menchetti M© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
An eleven year-old, male, beagle was presented with a two-month history of progressive stiff gait and spinal hyperalgesia. On the basis of clinical and magnetic resonance images features, an extensive bilateral paraspinal myopathy was diagnosed. Two weeks later, the dog was euthanized due to the worsening of pain. At post-mortem examination, multiple nodules of variable size were detected along the lumbar paraspinal musculature and the diaphragm pillars. Histologically, nodules were composed by fibroconnectival proliferation arranged around cores of atypical neoplastic cells which were positive for cytokeratine 19, demonstrating a glandular origin. A primary lesion was not found. Here we report an atypical case of adenocarcinoma of unknown primary origin metastasizing to the lumbar muscles and presenting with severe neuropathic pain.
2.Introduction
3.Case History
4.Discussion
5.References
Keywords
Cancer of Unknown Primary; CUP; Dog; Metastases; Neuropathic Pain.
Introduction
The term “cancer of unknown primary” (CUP) is applied to histologically-proven metastatic malignant tumours whose primary site cannot be identified during pre-treatment evaluation, including history, physical examination, laboratory and imaging studies and detailed histological evaluation [1].
In human medicine, CUP represents a real diagnostic problem, with lack of treatment guidelines [2, 3]. In USA, CUP accounts for 3-5% of all human cancers, it is reported to be the seventh to eighth most frequent malignant tumour, and it is the fourth most common cause of cancer death [4].
In veterinary oncology there are no large studies focusing on CUPs. Recently, Rossi et al. (2013) published a review with description of clinical features, treatment and outcome of 21 dogs with metastatic cancer of unknown primary [5]. Furthermore, Amati et al. (2012) described a case of disseminated carcinoma with extensive bone marrow involvement and carcinocythaemia whose primary site was not identified [6].
We report an atypical case of adenocarcinoma of unknown primary site metastasizing to the lumbar muscles and presenting with severe neuropathic pain.
Case History
An eleven year-old, castrated male, beagle was presented with a two-month chronic-progressive history of stiff gait on the hind limbs, kyphosis and hyperalgesia of the back. The owner noticed progressive reluctance to walk and jump. Efficacy of previous analgesic symptomatic treatments was unremarkable and, in the last two days, the dog was very hesitant to perform any movement, possibly due to the worsening of the painful condition.
On neurological examination, gait abnormalities consisted of mild paraparesis and reluctance to walk. The dog showed dramatic painful reactions (defensive behaviour and vocalization) after gentle palpation of the lumbar region. Other findings included slightly delayed postural reactions on the pelvic limbs.
Clinical signs allowed to localize the lesion at the level of the lumbar spine. Clinical differential diagnoses included degenerative intervertebral disk disease, discospondylitis, meningomyelitis, myositis and neoplastic disorders.
Complete blood cell count and urinalysis were unremarkable. Blood biochemistry only showed minor abnormalities, rather a specific or consistent with mild muscular damage (Table 1). Abdominal ultrasound and chest radiographs were normal.
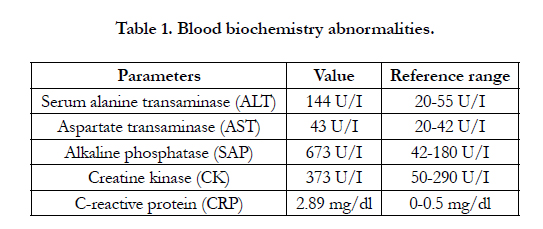

Table 1. Blood biochemistry abnormalities.
Magnetic Resonance Imaging (MRI) of the thoracolumbar spine was performed using a low-field MR scanner (MrV, Paramed,Genoa, Italy). MRI showed severe abnormalities affecting the entire lumbar dorsal and ventral paraspinal musculature, heterogeneously hyperintense on T2W sequences (data not shown), iso-to mildly hyperintense on T1W (Figure 1A), with marked and uniform post-contrast enhancement (Figure 1B) and markedly hyperintense on STIR (data not shown). MRI findings were suggestive of an inflammatory/infectious lesion of the paraspinal musculature and adjacent soft tissues. Cerebrospinal fluid obtained by lumbar puncture was normal.
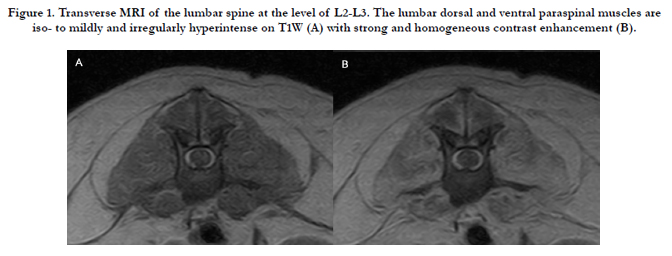
Figure 1. Transverse MRI of the lumbar spine at the level of L2-L3. The lumbar dorsal and ventral paraspinal muscles are iso- to mildly and irregularly hyperintense on T1W (A) with strong and homogeneous contrast enhancement (B).
Surgical biopsies were obtained from the longissimus dorsi muscle and routinely processed for histology and bacteriology. Histopathology showed mild hypertrophy and longitudinal splitting of muscular fibres. Bacterial culture was negative.
The dog was treated with different types of analgesics, consisting on first instance of gabapentin 5 mg/kg OS TID (Gabapentin, Teva Pharma) and robenacoxib 1 mg/kg EV SID (Onsior, Novartis). Subsequently was added methadone 0.2 mg/kg IM q4h (Eptadone, Molteni), replaced, finally, with fentanyl patch 50 μg (Durogesic, Janssen-Cilag).
The dog was minimally responsive to therapy and showed progressive deterioration of the clinical status due to the continuous painful stimulation of the back, that prevented normal locomotion. Two weeks later, the patient was euthanized for humane reasons and a complete necropsy was performed.
At gross examination, the lumbar paraspinal musculature was oedematous, with fatty infiltration and disseminated nodules of variable shape, ranging from 2 mm to 1 cm in diameter. Nodules were well demarcated, whitish and firm, localized in the thickness of the paraspinal muscles deep right up to the vertebral bodies (Figure 2). Similar lesions were also observed in the diaphragm pillars (data not shown). Cross-sections of the muscles of limbs, neck, head and tongue did not evidence further lesions. Lungs showed atelectasis and irregular thickening of the cranial lobes. A post-mortem morphological diagnosis of severe multifocal granulomatous myositis and chronic pneumopathy was made.
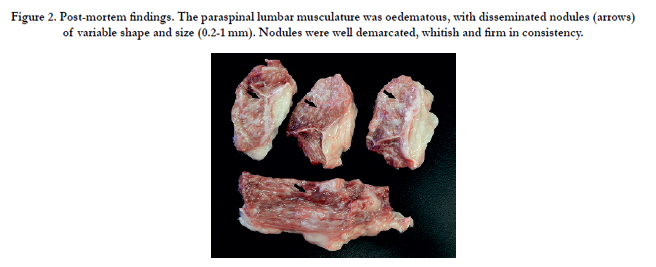
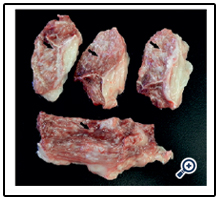
Figure 2. Post-mortem findings. The paraspinal lumbar musculature was oedematous, with disseminated nodules (arrows) of variable shape and size (0.2-1 mm). Nodules were well demarcated, whitish and firm in consistency.
Representative tissue samples were fixed in 10% neutral-buffered formalin and processed for histology. Microscopic examination of haematoxylin and eosin-stained sections showed that the spinal nodules were composed by fibroblasts and dense collagen fibres concentrically arranged around small cores of atypical cells. These cells were voluminous (20-30 μm) and polygonal, with distinct cytoplasmic borders. Cytoplasms were abundant, often containing irregular vacuolations. Nuclei were round, with clumped chromatin and prominent nucleoli (Figure 3A, B). Scattered nerve fibers were seen entrapped within the neoplastic tissue (Figure 3C). Histological appearance was consistent with a poorly differentiated carcinoma.
The same findings were also observed in the histological samples from the diaphragm and lungs (data not shown). Additionally, dilated vessels containing tumour cells (neoplastic emboli) were frequently seen in the sections ofparaspinal muscles (Figure 3D), diaphragm and lungs (data not shown). No relevant findings were observed in the other tissues examined microscopically (liver, kidneys, spleen, intestine, spinal cord, lumbar vertebrae).
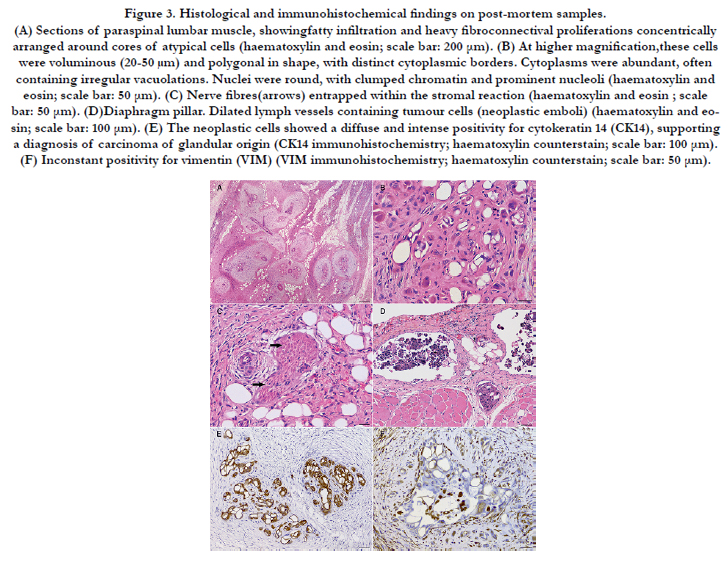
Figure 3. Histological and immunohistochemical findings on post-mortem samples.
(A) Sections of paraspinal lumbar muscle, showingfatty infiltration and heavy fibroconnectival proliferations concentrically arranged around cores of atypical cells (haematoxylin and eosin; scale bar: 200 μm).
(B) At higher magnification,these cells were voluminous (20-50 μm) and polygonal in shape, with distinct cytoplasmic borders. Cytoplasms were abundant, often containing irregular vacuolations. Nuclei were round, with clumped chromatin and prominent nucleoli (haematoxylin and eosin; scale bar: 50 μm).
(C) Nerve fibres(arrows) entrapped within the stromal reaction (haematoxylin and eosin ; scale bar: 50 μm).
(D) Diaphragm pillar. Dilated lymph vessels containing tumour cells (neoplastic emboli) (haematoxylin and eosin; scale bar: 100 μm).
(E) The neoplastic cells showed a diffuse and intense positivity for cytokeratin 14 (CK14), supporting a diagnosis of carcinoma of glandular origin (CK14 immunohistochemistry; haematoxylin counterstain; scale bar: 100 μm).
(F) Inconstant positivity for vimentin (VIM) (VIM immunohistochemistry; haematoxylin counterstain; scale bar: 50 μm).
In order to orient towards the primary tumour location, immunohistochemistry (IHC) was performed applying a broad panel of specific antibodies (Table 2) able to identify tissues of different origin. In particular, to recognize epithelial and glandular cells, the antibodies anti-pan-cytokeratin and-cytokeratin 19 were used, respectively. To identify tissues of mesenchymal and muscular (striated) origin, the antibodies anti-vimentin and desmine were used, respectively. The antibody anti-thyroid transcription factor-1 was employed to identify cells originating from thyroid and lung. To recognize tissues of neuronal origin,the antibodies anti-glial fibrillary acidic protein (glial cells marker), -S100 (peripheral glial cells and melanocytic marker), neuron specific enolase (neurons and neuroendocrine cells marker), and neurofilament 70 kDaprotein (neuronal marker) were used. All antibodies have been already utilized on dog tissues (Table 2) [7-14].
Appropriate positive and negative controls were used to assess the specificity of the reaction. Neoplastic cells were characterized by strong expression of pan-CK- and CK19-immunoreactivity (Figure 3E) and were inconstantly positive for VIM (Figure 3F). Neoplastic cells were negative for S100, TTF-1, NSE, DES, GFAP and NFP.
Based on histological and immunohistochemical findings, the diagnosis was muscle and lung metastases of adenocarcinoma of unknown primary site.
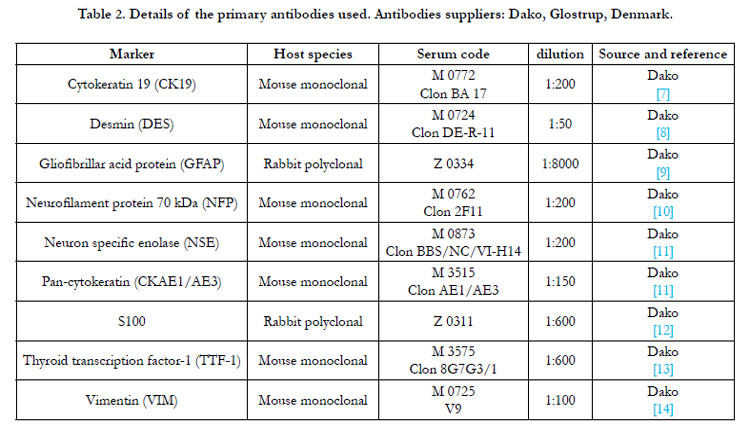
Table 2. Details of the primary antibodies used. Antibodies suppliers: Dako, Glostrup, Denmark.
Discussion
CUPs show common characteristics, such as aggressiveness, early dissemination and silent primary tumour. In human medicine, approximately half the cases are diagnosed as adenocarcinomas, 30% as poorly differentiated carcinomas, 15% as squamous cell carcinomas and the remaining 5% as undifferentiated neoplasms [15]. Identification of the primary tumour occurs before death in less than 20-30% of cases, even when extensive investigations take place. In most cases, the primary tumour remains unidentified even after post-mortem examination, but, if found, it is a small asymptomatic tumour often localized in the lung or pancreas [16, 17].
Some hypotheses have been postulated about the pathogenesis of CUPs. The primary tumour may remain diminutive, thereby escaping clinical detection, or it may undergo immune-mediated regression or dormancy after seeding the metastasis [18]. Other explanations include the angiogenic incompetence of the primary tumour, that may lead to cell apoptosis [19].
Although for several tumour types a specific immunohistochemical marker is not available and specificity and sensitivity of immunohistochemical tests are never absolute, IHC remains the best cost-effective method to identify the origin of CUPs [3].
In the case described here, the diagnosis was post-mortem because of the absence of neoplastic cells in the biopsies, probably due to superficial or intralesional tissue sampling. Even at necroscopic examination, the presence of multifocal sclerotic muscular nodules was more suggestive of a chronic inflammatory infectious or parasitic process. However, lesions were identified as metastases from a tumour of glandular origin, as confirmed by CKAE1/AE3 and CK19 positivity. As in human medicine, the most likely primary sites include stomach, bowel, pancreas, biliary tract or prostate, although extensive diagnostic imaging and postmortem examination failed to identify lesions at these sites.
Paraspinal muscle metastases have been documented in humans with non-small-cell-lung-carcinoma [20]; nevertheless, the case here described was negative to TTF-1, a reliable marker for primary lung carcinoma. Neoplastic cells also showed an inconstant positivity to vimentin. Cytokeratin and vimentin coexpression is not infrequent in poorly differentiated malignancy and is commonly reported in prostatic carcinoma [21].
Characteristic was the dramatic hyperalgesia, minimally responsive to vigorous analgesic treatment. This finding could be explained by the nerve entrapment by the neoplastic tissue, confirmed by histopathological examination. Neuropathic pain is a type of chronic pain well recognized in human medicine. There are several experimental animal models for neuropathic pain and the veterinary patients may react with allodynia (painful reaction to nonpainful stimuli) or with hyperalgesia (exaggerated responses to only mildly painful stimuli). The plasticity of the nervous system following persistent nociceptive processes is still object of study, and, in this case, may explain the unsatisfactory response to pharmacotherapy [22-24].
References
- Pavlidis N, Fizazi K (2009) Carcinoma of unknown primary (CUP). Critical Reviews in oncology/Hematology 69(3): 271-278.
- BalakerAE, Abemayor E, Elashoff D, St Jhon MA (2012) Cancer of unknown primary: does treatment modality make a difference? Laryngoscope 122(6): 1279-1282.
- Natoli C, Ramazzotti V, Nappi O, Giacomini P, Palmieri S, et al. (2011) Unknown primary tumors. Biochimica et Biophysica Acta (BBA)-Reviews on Cancer 1816(1): 13-24.
- Pavlidis N, Pentheroudakis G (2012) Cancer of unknown primary site. Lancet 379(9824): 1428-1435.
- Rossi F, Aresu L, Vignoli M, Buracco P, Bettini G, et al. (2015) Metastatic cancer of unknown primary in 21 dogs. Vet Comp Oncol 13(1): 11-19.
- Amati M, Miele F, Avallone G, Banco B, Bertazzolo W (2012) Carcinocythaemia (carcinoma cell leukaemia) in a dog: an acute leukaemia-like picture due to metastatic carcinoma. J Small Anim Pract 53(8): 476-479.
- Sassi F, Sarli G, Brunetti B, Morandi F, Benazzi C (2008) Immunohistochemical characterization of mammary squamous cell carcinoma of the dog. J Vet Diagn Invest 20(6): 766-773.
- Milovancev M, Hauck M, Keller C, Stranahan LW, Mansoor A, et al. (2015) Comparative pathology of canine soft tissue sarcomas: possible models of human non-rhabdomyosarcoma soft tissue sarcomas. J Comp Pathol 152(1): 22-27.
- Kegler K, Spitzbarth I, Imbschweiler I, Wewetzer K, Baumgartner W, et al. (2015) Contribution of schwann cells to remyelination in a naturally occurring canine model of CNS neuroinflammation. Plos One 10(7): e0133916.
- Nagamine E, Hiramaya K, Matsuda K, Okamoto M, Ohmachi T, et al. (2015) Diversity of histologic patterns and expression of cytoskeletal proteins in canine skeletal osteosarcoma. Vet Pathol 52(5): 977-984.
- Ramirez GA, Rodriguez F, Herraez P, Suarez-Bonnet A, Andrada M, et al. (2014) Morphologic and immunohistochemical features of Merkel cells in the dog. Res Vet Sci 97(3): 475-480.
- Hoinghaus R, Mischke R, Hewicker-Trautwein M (2002) Use of immunocytochemical techniques in canine melanoma. J Vet Med A Physiol Pathol Clin Med 49(4): 198-202.
- Ciaputa R, Nowak M, Kandefer-Gola M, Dziedzic K, Halupka P, et al. (2014) Morphological and immunohistological characteristics of follicularcompact thyroid carcinoma in dog. Folia Histochem Cytobiol 52(2): 157-161.
- Clemente M, Pérez-Alenza MD, Illera JC, Pena L (2010) Histological, immunohistological, and ultrastructural description of vasculogenic mimicry in canine mammary cancer. Vet Pathol 47(2): 265-274.
- Pavlidis N, Briasoulis E, Hainsworth J, Greco FA (2003) Diagnostic and therapeutic management of cancer of an unknown primary. Eur J Cancer 39(14): 1990-2005.
- van de Wouw AJ, Jansen RL, Speel EJ, Hillen HF (2003) The unknown biology of the unknown primary tumour: a literature review. Ann Oncol 14(2): 191-196.
- Pentheroudakis G, Briasoulis E, Pavlidis N (2007) Cancer of unknown primary site: missing primary or missing biology? Oncologist 12(4): 418-425.
- Karlsson M, Lindberg K, Karlén P, Ost A, Thorn M, et al. (2010) Evidence for immunosurveillance in intestinal premalignant lesions. Scand J Immunol 71(5): 362-368.
- Naresh KN (2002) Do metastatic tumours from an unknown primary reflect angiogenic incompetence of the tumour at the primary site? A Hypotheses. Med Hypotheses 59(3): 357-360.
- Strauss JB, Shah AP, Chen SS, Gielda BT, Kim AW (2012) Psoas muscle metastases in non-small cell lung cancer. J Thorac Dis 4(1): 83-87.
- Grieco V, Patton V, Romussi S, Finazzi M (2003) Cytokeratin and vimentin expression in normal and neoplastic canine prostate. J Comp Pathol 129(1): 78-84.
- Schaible HG, Richter F (2004) Pathophysiology of pain. Langenbeck’s Archives of Surgery 389(4): 237-243.
- Mizoguchi H, Watanabe C, Yonezawa A, Sakurada S (2009) New therapy for neuropathic pain. Int Rev Neurobiol 85: 249-260.
- Grubb T (2010) Chronic neuropathic pain in veterinary patients. Top Companion Anim Med 25(1): 45-52.





