Regulations of Regenerative Medicine Including Clinical Application of iPS Cells in Japan
Hikari Inoue1, Tatsuaki Tsuruyama1,2*
1Tissue Research Project, Center for Anatomical, Pathological, and Forensic Medical Research, Graduate School of Medicine, Kyoto University, Japan.
2 Department of Drug Discovery Medicine and Pathology, Graduate School of Medicine, Kyoto University, Japan.
*Corresponding Author
Tatsuaki Tsuruyama
Department of Drug Discovery Medicine and Pathology & Tissue Research Project,
Kyoto University Graduate School of Medicine,
Yoshida-Konoe-cho,Sakyo-ku, Kyoto 606-8501, Japan.
Tel: +81-75-753-4427
Fax: +81-75-753-4493
E-mail:tsuruyam@kuhp.kyoto-u.ac.jp
Received: March 21, 2016; Accepted: April 12, 2016; Published: April 15, 2016
Citation: Hikari Inoue, Tatsuaki Tsuruyama (2016) Regulations of Regenerative Medicine Including Clinical Application of iPS Cells in Japan. Int J Stem Cell Res Transplant. 04(4), 179-181.DOI : dx.doi.org/10.19070/2328-3548-1600029
Copyright: Tatsuaki Tsuruyama© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Clinical studies of regenerative medicine using induced pluripotent stem (iPS) cells have recently been performed, especially in Japan. To promote regenerative medicine research using iPS cells, the related laws have been enacted in Japan, leading to the use of other bioresources. Here, we overview the legislation of regenerative medicine. In parallel with this legislation, Kyoto University Hospital and the Center for iPS Cell Research and Application (CiRA) at Kyoto University, Japan, have rapidly established a bioresource stocking system for the purpose of clinical study and therapy using iPS cells. Kyoto University Hospital and CiRA are now preparing for the use of stocked iPS cells and other bioresources based on joint research contracts between Kyoto University and external institutions.
2.Background
4.Guidelines and laws on human stem cell use in Japan
5.Acceleration of legislation from 2010 onwards
6.Discussion
7.Summary
8.References
Keywords
Act on the Safety of Regenerative Medicine; Clinical application of iPS Cells; Material Transfer Agreement.
Background
Since the discovery of reprogramming somatic cells, there have been extensive debates on the clinical application of induced pluripotent stem (iPS) cells [1]. The potential of this novel technique includes establishing disease models [25], screening candidate drug [6], and cell transplant therapies [7]. Consequently, there has been great interest in using iPS cell repositories to advance translational medicine research. Repositories of a variety of human resources are also in the process of being established to facilitate their use in clinical research globally (www.isber.org/). The cell and tissue stocking system will ensure the prospective procurement and collection of bioresources for this field of research, with appropriate Informed Consent (IC) and sufficient quality control. Kyoto University in Japan is one of several core institutes worldwide that promote the use of iPS cells for future research in regenerative medicine [1,6].
Japanese policy has developed unique regulations with respect to clinical research using human bioresources and stem cells. Researchers are subject to reviews by Institutional Review Boards (IRBs), according to the guidelines of the Ministry of Education, Culture, Sports, Science and Technology (MEXT), the Ministry of Health, Labour and Welfare (MHLW), and the Ministry of Economy, Trade and Industry (METI) (www.lifescience.mext.go.jp/files/pdf/43_137.pdf) in Japan. Guidelinesregulating specific procedures for embryo handling also exist with respect to research using embryo (http://www.lifescience.mext.go.jp/files/pdf/n1553_01r2.pdf ; http://www.lifescience.mext.go.jp/files/pdf/n1553_02r2.pdf ). The relevant ministries and agencies may, for example, suspend subsidy payments to researchers at institutions when they violate guidelines, with these guidelines being indirectly enforced on researchers and their institutes by the ministries. In addition to the guidelines, a special law (Law on Regulation of Human Cloning Techniques) was enacted as early as 2000 (www.lifescience.mext.go.jp/files/pdf/43_137.pdf) to prohibit the production of human clones and embryonic cells, in direct response to publicized advances in cloning technology.
Here, we describe the main guidelines on research using human bioresources, with a special focus on the unique regulations on clinical research in Japan. After that, we introduce Japanese policies on regenerative medicine that has been recently developed iPS cells and cell transplantation. Thus, this study aimed to provide an overview of issues that exist with respect to the use of iPS cells and other bioresources in clinical research. Furthermore, we propose ethical management and the use of certain procedures to be met in contracts for the use of iPS cells in clinical research.
Guidelines and laws on human stem cell use in Japan
In 2006, Guidelines for Clinical Research Using Human Stem Cells was publicly issued in Japan (revised in 2013). The guidelines request researchers in Japan to obtain permission from the MHLW to conduct clinical research using stem cells. After that, the Act on the Safety of Regenerative Medicine (or the so-called Regenerative Medicine Law[RML]) was enacted to integrate the guidelines for stem cell research (www.mhlw.go.jp/english/policy/health-medical/medical-care/dl/150407-01.pdf).A well-known example of clinical research approved in 2013 is the clinical trial for transplanting iPS cell-derived retinal pigment epithelium for the therapy of patients with age-related maculopathy [8, 9]. The transplantation of iPS cells that develop into retinal epithelial cells was first performed on September 12, 2014 [10]. The IRB of RIKEN (/www.riken.jp/en/) based on the Guidelines for Clinical Research Using Human Stem Cells decided to approve this project. Therefore, the MHLW officially approved the project, which was the world’s first clinical trial using material from patient-derived iPS cells at that time.
Acceleration of Legislation from 2010 onwards
Since 2010, legislation concerning medical research has increased to an unprecedented extent. In response to the recent developments in regenerative medicine using techniques involving ES cells and iPS cells, the standardization of treatment outcomes was proposed by Prof. Yamanaka, our colleague in Kyoto University, and the Japanese Society of Regenerative Medicine, as a crucial issue for the appropriate development of regenerative medicine. The Expert Committee on Promotion and Ensuring the Safety of Regenerative Medicine (since September 2012) of the MHLW considered the legal framework of the RML, with the aim to promote appropriate provision of cells for transplantation therapy. In parallel, Japanese Pharmaceutical Affairs Law was drastically revised. RMLrequires a license for the establishment of cord blood and bone marrow banks, and provides measures to ensure the quality control of bioresources. This law regulates treatments using cells that have unknown risk and that may have long-term risks, in addition to regulating cosmetic medicine. Thus, the RML comprehensively regulates cell-transplantation medicines involving activated lymphocytes against cancer cells. These regulations encompass the administration of human stem cells (ES cells, iPS cells, and somatic stem cells [e.g., adipose-derived stem cells]). Cell processing for administration to patients and in research is also regulated. Therefore, RML integrates objectives that have been regulated by Guidelines on the Derivation of Human Embryonic Stem Cells.
The RML separates clinical research using cells into three categories. The first category, which is the most high-risk, includes autologous transplantation or transplantation of ES/iPS-derived cell products. Non-homologous transplantation using lymphocytes transfected with artificial gene expression vectors is also included in this category. The second category includes post-mastectomy therapy for breast rebuilding by using adipose-derived stem cells. The third category includes anticancer therapy by the transfusion of lymphocytes that have been activated using cytokines, such as interleukins. The cells in the third category are essentially heterogeneous, with quality control being generally difficult. Thus, this law regulates immunotherapy that has not yet been established with respect to clinical interventions. Consequently, Japanese patients are not supported by national insurance coverage for these procedures. The MHLW aims to balance the safety and promotion of regenerative medical research by estimating the risks and benefits of this research (Figure 1). Details of the RML were publicized in August 2014, and came into effect in November 2014.
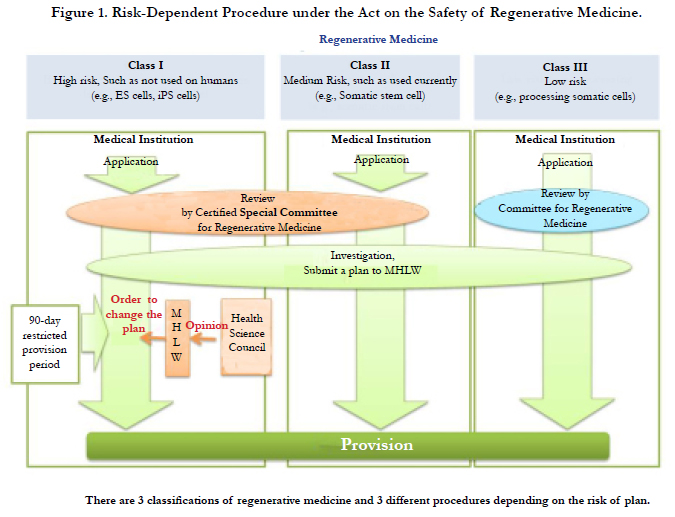
Figure 1. Risk-Dependent Procedure under the Act on the Safety of Regenerative Medicine.
Discussion
Non-legal regulation via guidelines has traditionally been the main form of regulation in Japan. However, this trend has started to change in recent years. RML takes the form of a national strategy for developing regenerative medicine in Japan. The government endorses clinical applications and aims to provide legislation to promote regenerative medicine. The aim of this regulation is absolutely to promote research on regenerative medicine. In 2012, Expert Committee on Promotion and Ensuring the Safety of Regenerative Medicine presented a report detailing that there was no standard protocol for the culturing and processing of cells for clinical applications. Therefore, the RML was enacted to enable medical institutes to culture and process human stem cells. It was also enacted to propose the requirement of a license for the establishment of cell culture-processing facilities, by presenting the necessary conditions on facilitate, staff, and so on, to promote efficient research. Enforcement of the law obliges researchers to submit research plans on the proposed of use human stem cells to the MHLW (article 4, RML), and to follow the criteria for the donation of human stem cells for regenerative medicine or clinical research according to ministerial ordinance (article 3, RML).
The RML generally regulates the use of various types of cells for cell therapy (including lymphocytes that are activated by cytokines, iPS cells, and ES cells) after obtaining them from patients for autologous immune-enhancement therapy against cancers. To realize the use of iPS cells for various therapies, the prompt recruitment of the optimal iPS cells that are adaptable for transplantation without immunological rejection is necessary, with the lining-up homozygous human leukocyte antigens (HLA) [13] requiring speed [14]. At the Center for iPS Cell Research and Application (CiRA)
(www.cira.kyoto-u.ac.jp/e/index.html; www.mhlw.go.jp/stf/shingi/2r9852000002ofeo-att/2r9852000002ofj5.pdf), the donation of iPS cells for regenerative medicine was initiated in August 2015. In addition, disease-specific iPS cells were stocked. Solomon et al. suggested that a moderate-sized bank should be made available to match recipients [14]. Stocking of iPS cell lines with HLA-A, HLA-B, and HLA-DR haplotypes aims to cover a large proportion of the Japanese population [15]. Within the next 5 years, CiRA aims to establish a repository of iPS cells carrying HLA homo-type donor to species that cover 90% of the entire Japanese population. CiRA is planning to research using iPS cells and are applying the research plan to IRB and Certified Special Committee for Regenerative Medicine. Of course, good manufacturing practices (GMP) are required, as well as standards for quality control and regulatory legislation. Furthermore, donor selection, screening, and IC for research use are necessary, with a global GMP ultimately being required [16,17].
Transfer of human bioresources from Kyoto University to other institution, is mainly in a collaborative research contract. It’s be cause we consider that we should manage the use of bioresources even after transfer. From perspective of ethical management for protection of donors of iPS cells, this policy has been maintained.
Summary
Regulation policies for human bioresource research in Japan are constantly evolving, with the national government intervening directly with regenerative medicine legislation in 2014. This enactment aims to promote regenerative medicine research with respect to the therapeutic applications of iPS cells by using highquality human bioresources. iPS cell stocks have been established for the distribution of iPS cells to promote collaborative research between Kyoto University and external institutes, which involves a joint research contract.
Acknowledgments
We thank Dr. Mika Suzuki (CiRA, Kyoto University, Kyoto, Japan) for advice regarding the manuscript. This manuscript was supported by Center of Innovation (COI) Program, JAPAN SCIENCE AND TECHNOLOGY AGENCY.
References
- Takahashi K, Yamanaka S (2006) Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 126(4): 663-676.
- Ma J, Guo L, Fiene SJ, Anson BD, Thomson JA, et al. (2011) High purity human-induced pluripotent stem cell-derived cardiomyocytes: Electrophysiological properties of action potentials and ionic currents. Am J Physiol Heart Circ Physiol 301(5): H2006-H2017.
- Itzhaki I, Maizels L, Huber I, Zwi-Dantsis L, Caspi O, et al. (2011) Modelling the long QT syndrome with induced pluripotent stem cells. Nature 471(7337): 225-229.
- Urbach A, Bar-Nur O, Daley GQ, Benvenisty N (2010) Differential modeling of fragile X syndrome by human embryonic stem cells and induced pluripotent stem cells. Cell Stem Cell 6(5): 407-411.
- Liras A (2011) Induced human pluripotent stem cells and advanced therapies: Future perspectives for the treatment of haemophilia? Thromb Res 128(1): 8-13.
- Inoue H, Yamanaka S (2011) The use of induced pluripotent stem cells in drug development. Clin Pharmacol Ther 89(5): 655-661.
- Osakada F, Jin ZB, Hirami Y, Ikeda H, Danjyo T, et al. (2009) In vitro differentiation of retinal cells from human pluripotent stem cells by smallmolecule induction. J Cell Sci 122(Pt 17): 3169-3179.
- Song P, Inagaki Y, Sugawara Y, Kokudo N (2013) Perspectives on human clinical trials of therapies using iPS cells in Japan: reaching the forefront of stem-cell therapies. Biosci Trends 7(3): 157-158.
- Kamao H, Mandai M, Wakamiya S, Ishida J, Goto K, et al. (2014) Objective evaluation of the degree of pigmentation in human induced pluripotent stem cell-derived RPE. Invest Ophthalmol Vis Sci 55(12): 8309-8318.
- Nakano-Okuno M, Borah BR, Nakano I (2014) Ethics of iPSC-based clinical research for age-related macular degeneration: patient-centered risk-benefit analysis. Stem Cell Rev 10(6): 743-752.
- Lowenthal J, Lipnick S, Rao M, Hull SC (2012) Specimen collection for induced pluripotent stem cell research: harmonizing the approach to informed consent. Stem Cells Transl Med 1(5): 409-421.
- Kurtz A, Stacey G, Kidane L, Seriola A, Stachelscheid H, et al. (2014) Regulatory insight into the European human pluripotent stem cell registry. Stem Cells Dev 23(Suppl 1): 51-55.
- Frehland E (1980) Current fluctuations in discrete transport systems far from equilibrium. Breakdown of the fluctuation dissipation theorem. Biophys Chem 12(1): 63-71.
- Solomon S, Pitossi F, Rao MS (2015) Banking on iPSC--is it doable and is it worthwhile. Stem Cell Rev 11(1): 1-10.
- Nakatsuji N, Nakajima F, Tokunaga K (2008) HLA-haplotype banking and iPS cells. Nat Biotechnol 26: 739-740.
- de Rham C, Villard J (2014) Potential and limitation of HLA-based banking of human pluripotent stem cells for cell therapy. J Immunol Res 2014: 1-6.
- Barry J, Hyllner J, Stacey G, Taylor C, Turner M (2015) Setting up a Haplobank: Issues and solutions. Curr Stem Cell Rep 1(2): 110-117.
- Medical Research Council (2014) Human Tissue and Biological Samples for Use in Research: Operational and Ethical Guidelines.
- Jeffers B (2001) Human Biological Materials in Research: Ethical Issues and the Role of Stewardship in Minimizing Research Risks. ANS Adv Nurs Sci 24(2): 32-46.
- Crombie S, Karen M, Moussa M, McLachlin M, Hammond R (2015) The Pathology Tissue and Archive Committee: Its Role in Human Tissue Research.Canadian J Pathol 7(3): 15-22.
- Cervo S, De Paoli P, Mestroni E, Perin T, Escoffier L, et al. (2016) Drafting biological material transfer agreement: a ready-to-sign model for biobanks and biorepositories. Int J Biol Markers.





