Insights into Chronic Postsurgical Pain
Prgolizzi JV 1,2, Zampogna G 1, Robert Taylor Jr1*, Raffa RB3,4
1 NEMA Research, Inc., Naples, FL, USA.
2 Naples Anesthesia and Pain Associates , Naples, FL, USA.
3 Professor Emeritus, Department of Pharmaceutical Sciences, Temple University School of Pharmacy, Philadelphia PA, USA.
4 Adjunct Professor, Department of Pharmacology and Toxicology, University of Arizona College of Pharmacy, Tucson, AZ, USA.
*Corresponding Author
Robert Taylor Jr., PhD,
NEMA Research Inc., Naples, FL 34108 USA.
Tel: 239.908.4442/239.597.3662
Fax: 239.908.4432
E-mail: rtaylor@nemaresearch.com
www.nemaresearch.com
Received: January 21, 2016; Accepted: October 27, 2016; Published: October 31, 2016
Citation: Pergolizzi JV, Zampogna G, Robert Taylor Jr, Raffa RB (2016) Insights into Chronic Postsurgical Pain. Int J Surg Res. 3(5), 55-60. doi: dx.doi.org/10.19070/2379-156X-1600012
Copyright: Taylor R© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Most postsurgical patients experience moderate to severe acute pain which, in some patients, transitions to chronic postsurgical pain (CPSP). Optimal pain control of acute surgical pain will likely blunt or prevent the transition of acute postsurgical pain (APSP) to CPSP. While there are known risk factors for such chronification of pain type, and certain surgeries (such as limb amputation) and approaches (open versus laparoscopic) are associated with higher rates, it is impossible to predict which patients will transition to CPSP. Additionally, despite knowledge and an armamentarium of analgesics, APSP may be suboptimally controlled. Opioid analgesics can be safe and effective for APSP, but there are legal, social, governmental, clinical, and even cultural barriers to their use. Patients may be reluctant to take opioid agents even when available. Effective APSP control is essential to promote speedy recovery, rapid ambulation, good rehabilitation, and, ultimately, hospital discharge. Since, pain can be multimechanistic, multimodal or combination therapy may be required. Fixed-dose combination products are available that may reduce total opioid consumption by combining a small amount of opioid with an NSAID or paracetamol (acetaminophen). For CPSP, transdermal buprenorphine appears to offer certain advantages in that it is an effective analgesic, can be safely used without dosage adjustment in the elderly and in those with compromised renal function, and the patch delivery system reduces pill burden and reduces the problem of non-compliance. Since tolerability is an important consideration for any pain relievers, side effects should be managed proactively and promptly.
2.Consequences of Unrelieved Surgical Pain
3.Barriers to Effective Analgesia in the Immediate Postoperative Period
4.The Fifth Vital Signt
5.Combination Therapy
6.Barriers to Opioid Therapy
7.The Potential Role of Transdermal Buprenorphine for CPSP
8.Managing Side Effects
9.Strategies and Tactics for Chronic Postoperative Pain Control
10.Conclusion
11.References
Introduction
More than 80% of postsurgical patients report pain, and 86% of them describe the pain as moderate to very severe [1]. While most patients are realistic and accept that pain will occur following surgery, dealing with postoperative pain is the primary concern of 59% of surgical patients. For many patients, postsurgical pain follows an expected and predictable trajectory, and is most intense in the first postoperative day and diminishes slowly over the following days. However, sometimes acute postsurgical pain (APSP) transitions to chronic pain syndromes[2]. Chronic postsurgical pain (CPSP) is not rare; in a survey of 5,000 chronic pain patients, 22.5% reported that their chronic pain originated with surgical pain [3]. Depending on the type of surgery and individual patient factors, CPSP may occur in up to one-third of patients after surgery[4]. CPSP has been defined as pain that lasts three months or more after surgery.[5] Another proposed definition of CPSP is pain that lasts two or more months after surgery and for which causes other than surgery can be excluded [4]. There is no consensus definition of CPSP or the point at which APSP transitions into CPSP.
Pain management should be individualized, because no one analgesic product provides 100% pain relief 100% of the time in 100% of patients without side effects. In fact, virtually all analgesic agents have tolerability and toxicity issues which must be weighed against their potential therapeutic benefits. For patients already on pharmacological therapy, drug-drug interactions must be considered when prescribing pain relievers. Fortunately, there are several analgesic options available today.
Clinicians need better knowledge about these options in order to better match appropriate drugs to the right patients to control both APSP and CPSP. Without such knowledge, pain control is often suboptimal. Oligoanalgesia, i.e.,inadequate analgesia, can occur at any point along the continuum of care. It has been reported in emergency departments [6] and postsurgical patients and it is known that certain patients, such as the very young,[7] the elderly, [8] women, [9] and lower socio-economic classes are more at risk for oligoanalgesia.In short, postsurgical pain often goes undertreated [1,10] The objective of our narrative review is to raise awareness about chronic postsurgical pain syndromes and explore their possible association with acute postsurgical pain and discuss therapeutic options to better control chronic postsurgical pain.
Consequences of Unrelieved Surgical Pain
Acute surgical pain may not only cause suffering, it may also cause distress, leading to fear, anxiety, and sleep disruptions, which, in turn, can delay ambulation and adversely delay rehabilitation. Acute pain syndromes, such as APSP, can lead to disordered breathing patterns, resulting in atelectasis, hypercarbia, and hypoxia, setting the stage for pneumonia. Unrelieved postsurgical pain can increase sympathetic activity, which may lead to, or exacerbate, pre-existing hypertension or tachycardia. Unrelieved acute pain of any etiology can lead to peripheral and central sensitization, leading to impaired pain signal processing and chronic pain syndromes [11,12] The exact transition of acute-tochronic pain syndromes remains incompletely elucidated [13]. While CPSP is not uncommon,[4,5,14] fortunately most patients do not transition from APSP to CPSP. It is not entirely clear why some APSP resolves completely and other transitions to chronic pain. The risk factors for persistent postsurgical pain have been proposed to include preoperative factors (such as anxiety, catastrophizing, depression, comorbid pain syndromes, stress, and impaired sleep), intraoperative and immediate postoperative factors (the extent of nerve and tissue injury, type of surgery, anesthetic technique, and analgesia), and factors associated with the delayed postoperative period (subsequent therapies such as chemotherapy or radiation, psychosocial factors, surgical revisions)[15]. Despite risk stratifications, it is not possible to predict which specific patients will develop CPSP.
The incidence of CPSP varies depending on the type of surgical procedure. Limb amputation and breast surgery are associated with high rates of CPSP (30%-83% and 31%-83%, respectively), while laparoscopic procedures are associated with lower rates of chronic pain, even compared to similar, but open, procedures. For example, laparoscopic gallbladder surgery is associated with a 6% - 26% incidence of chronic pain versus 21% - 60% with open cholecystectomy [16]. The intensity of APSP is one predictor of CPSP, but multiple factors are likely involved [16]. If CPSP is indeed the chronification of APSP, then effective analgesia in the immediate postoperative phase is crucial to preventing chronic pain syndromes.
Barriers to Effective Analgesia in the Immediate Postoperative Period
Ineffective or incomplete pain control immediately following surgery may occur for any of several reasons. First, clinicians may not have adequate knowledge of pain control, which includes the ability to assess and measure pain and effectively treat it. Despite the fact that pain is a common complaint, physicians may not be up-to-date in terms of current and growing knowledge of pain perception and appropriate, multimechanistic treatments. Many clinicians are not experienced in the use of new analgesic products, novel delivery systems, and combination therapies for pain control. In general, medical education does not emphasize pain management, and physicians and other healthcare professionals may have little to no training in the appropriate role of opioid and nonopioid analgesics following surgery. As our understanding of pain and analgesic agents evolves, this increased knowledge creates the unintended consequence of “information overload.” Clinicians can be overwhelmed by innovative products, new understandings of pain mechanisms, novel formulations and routes of administration, and new adjuvant agents. This can instill reticence rather than confidence when making prescribing choices.
Uncontrolled or under-treated APSP is not only distressing to patients and their families; it is expensive to the healthcare system. Pain accounts for 38% of unanticipated admissions and readmissions following ambulatory surgery at a mean cost of US$1,869 ± $4,553 per visit[17]. Suboptimally managed APSP can prolong hospital stays, delay ambulation, adversely affect rehabilitation, and be a reason for patients to report dissatisfaction with their care.
The Fifth Vital Sign
Pain should be assessed as the “fifth vital sign” following surgery. Pain rating scales can be useful tools to quantify and compare pain metrics; such scales include numeric rating scales (NRS)and visual analog scales (VAS) [18, 19].There is no perfect pain assessment tool, but there are many validated instruments that are reliable and easy to use. It is more important that pain be frequently assessed using a validated instrument than that a particular tool be used. The clinician should not only document pain intensity but also pain location, its nature (e.g., incisional, muscular, bone, neurogenic, etc.), and how long it has lasted. Patients should be encouraged to describe their pain, report changes in their pain, and request pain medicine as needed.
While pain intensity is not the only dimension of pain, it is an important measure and one on which the World Health Organization (WHO) built its now-famous “Pain Ladder”, describing how pain control therapy should change as pain persists or worsens. The WHO Pain Ladder recommends nonopioids with or without adjuvant agents for treating mild pain, adding so-called “weak” opioids as pain intensifies and, finally, relying on strong opioid for severe pain [20] The WHO pain ladder was designed as a simple treatment paradigm for cancer pain, but it is widely used around the world to treat other chronic pain syndromes. The fundamental concern is that pain is treated effectively [21] and safely rather than be ignored.
Combination Therapy
Acute and chronic postsurgical pains may involve more than one physiologic mechanism, including neuropathic components, which means that a single agent alone is unlikely to be sufficient to control them [22] Combination analgesic therapy involves using two or more agents that have different, complementary, mechanisms of action [23]. Pharmacological agents to address pain include nonopioid agents (such as acetaminophen and nonsteroidal anti-inflammatory drugs or NSAIDs), opioid analgesics, and adjuvant agents (such an anticonvulsants, muscle relaxants, and antidepressant agents).
When two or more agents are taken together, they may produce an additive result (equal to the sum of the individual components) or a synergistic result (greater than the sum of the parts)[24]. Note that additive and synergistic effects may apply to adverse events as well asanalgesia, therefore, it is important to combine drugs rationally [25]
The goal in management of APSP is to achieve optimal pain control (which is not necessarily complete pain relief) with minimal or at least tolerable side effects. Selecting pain relievers should be based on the patient’s response to therapy, the patient’s own risk factors for adverse reactions, potential drug-drug interactions, the type of surgery, and the acute postsurgical pain trajectory, that is, the reasonable assumptions about how pain immediately after surgery will progress. Not all analgesic therapies are appropriate for all patients, even similar patients undergoing the same surgery.
For patients dealing with CPSP, the analgesic therapy must be appropriate for long-term use. Patients must be comfortable with the agent and compliant about taking their medications as directed. Patients dealing with any form of chronic pain syndrome must be educated that pain management is a lifestyle rather than a short-term, defined period of therapy. For most CPSP patients, nonopioid and opioid agents are the primary analgesics, with antidepressants, anticonvulsive agents, and muscle relaxants as possible adjuvant agents. Topical agents may be appropriate in some cases [26].
Interventional treatments may be useful in specific CPSP cases. The literature reports reversal of CPSP in two total knee replacement patients with ultrasonography-guided pulsed radiofrequency (PRF) of nerves to the knee together with socalled “dry needling” to relax myofascial bands that were causing stiffness and physical therapy [27]
Pain perception involves both peripheral and central activity. For example, pain is perceived when a noxious stimulus in the periphery travels via primary afferents to the dorsal root ganglia and then via the spinal cord to the brain. Pain pathways in the spinal cord have the ability to modulate the signals’ transmissions, blunting or amplifying them. Since pain involves a cerebral component, pain has emotional as well as purely physical aspects. Pain control can be exerted at the peripheral level (such as local injections), at the central level (such as central analgesics), or both (such as opioids, NSAIDs, and acetaminophen). Opioids act through 7-transmembrane G protein-coupled opioid receptors (mu, kappa, and delta) to inhibit the transmission of nociceptive signals from the periphery to the spinal cordand by activating inhibitory pathways that modulate pain signal transmissionsat the spinal cord.
Chronic pain is fundamentally different than acute pain. Typically, acute pain has a well-defined cause and follows a reasonably predictable course based on its etiology. Acute pain usually resolves progressively, being most intense at first and diminishing gradually. Chronic pain often seems dissociated from its source; it may be perceived by the patient as diffuse, changing, or migrating [28]. Chronic pain is often multimechanistic and may have a neuropathic component that requires multimodal therapy. The most challenging aspect for any chronic pain syndrome is that chronic pain is essentially an aberrant pain transmission; it occurs when pain signaling is abnormal [11]. Thus, APSP may be treated by allowing the patient to heal; “healing” is not helpful to the chronic pain patient.
Short-term opioid therapy isfrequently prescribed to control APSP. The new CDC guidelines for opioid therapy recommend such pain control be limited to three days [29]. Opioids can also be used effectively to treat chronic pain syndromes [30], but their use in this setting should be carefully considered and closely monitored [29] In addition, the response to opioid analgesia may vary by patient. Opioid variability is known to occur due to both biological and psychosocial factors [31] Patient age, sex, previous opioid experience, pre-existing pain syndromes, and ethnicity may also play a role. Thus, opioids are not equally effective or equally well tolerated in all patients. However, when appropriately prescribed and monitored, opioid therapy can be highly effective for both APSP and CPSP.
Whenever opioid analgesics are prescribed, patients should be closely monitored, and both pain levels and adverse events assessed frequently. If necessary, opioid agents may be changed to achieve optimal pain control with tolerable side effects.
Barriers to Opioid Therapy
Despite the fact that opioids are known to be safe and effective pain relievers for APSP and CPSP, they may no be used . There are multiple reasons why opioid analgesics may not be used, even in appropriate patients with indications for opioid therapy. Physicians and prescribers can be concerned about legal issues, fear of prosecution, or other liabilities, which in many parts of the world are not trivial [32]. In some regions, there may be governmental or local regulations that limit or prohibit the use of opioids. Physicians may also be concerned that prescribing opioids might allow for opioid diversion or abuse [33]. Many prescribers are not confident in their own training about opioid titration, opioid tapering, and other factors associated with opioid therapy, [34] and thus prefer to prescribe more familiar agents.
Patients may also be reluctant to take opioids, even when prescribed by a trusted physician. Patients may refuse opioid therapy because they have fears about drug tolerance, addiction risks, and the side effects associated with opioids [35, 36]. Cultural attitudes about pain as a necessary part of life or a notion that it is noble to endure suffering without complaint can also affect a patient’s willingness to take pain relievers [37].
However, in the acute postsurgical period, unrelieved pain may delay recovery and possibly transition to persistent, long-term pain or CPSP, which can become a lifelong condition that can adversely affect quality of life, productivity, and function.
The Potential Role of Transdermal Buprenorphine for CPSP
There are numerous opioid analgesic products on the market, including fast-acting and controlled-release formulations and products that offer different routes of administration (e.g., oral, intramuscular, intravenous, rectal, sublingual, transmucosal, transdermal, etc.). It is beyond the scope of this paper to discuss all opioid analgesic options, particularly for control of APSP. For the treatment of CPSP, it is worth discussing transdermal buprenorphine as an agent of particular interest. Although it is not the only agent that can be safely and effectively used in this setting, it offers certain unique advantages [38].
Buprenorphine has been described as a “partial agonist” in pharmacological terms, but that may be misleading in that it does not act as a “partial agonist” in terms of analgesia [39,40] Its dosing range for analgesic effect is 0.2 - 7 mg. There is no ceiling for analgesic effect, but there is a ceiling effect for respiratory depression [38].
In the United States, there are several buprenorphine formulations approved: an injectable buprenorphine (Buprenex® approved in 1981),a sublingual formulation (Subutex® approved in 2002), a sublingual formulation combined with naloxone (Suboxone® approved in 2002), and a transdermal patch (Butrans® approved in 2010). It should be noted that both of the sublingual formulations are indicated for treating opioid dependence rather than pain syndromes.
Transdermal buprenorphine is available in a patch that allows for seven-day drug delivery (steady state is achieved by day three). The transdermal delivery system allows for convenient dosing and reduces issues of patient compliance. Because buprenorphine is highly potent and highly lipophilic, it is well suited for patch systems and has been shown effective in clinical studies [41-43]. It is metabolized primarily hepatically via the CYP3A4,-2C8, -3A5, and -3A7 systems to norbuprenorphine and via CYP3A4, -3A5, and -3A7 isoforms to OH-buprenorphine. Norbuprenorphine is, in turn, metabolized to the 3-O-glucuronide and OHnorbuprenorphine.
Buprenorphine is the recommended first-line opioid analgesic for geriatric patients and for those with compromised renal function, because there is no drug accumulation in the system [38,44] Excretion of buprenorphine is mainly biliary with only about 30% excreted through the kidneys. Buprenorphine is equally effective and well tolerated among patients <50 years and those > 65 years [45] With other opioids, the drug half-life and the half-life of active metabolites can build up, making them unsuitable for use in the elderly and/or those with reduced renal function.
The equianalgesic dosing of buprenorphine may depend on the route of administration, but as a rule of thumb, buprenorphine should be considered to be about 100-times more potent than morphine. The therapeutic index (defined as the lethal dose for 50% of population divided by the effective dose for 50% of the population) of buprenorphine is 12,313 compared to 464 for morphine [46].
When initiating transdermal buprenorphine, patients taking less than 30 mg oral morphine daily (or oral regimens of 90 mg codeine, 300 mg tramadol, or 15 mg oxycodone) should commence with the 5 μg/hour patch. Patients taking 30 to 80 mg of oral morphine daily (or oral regimens of 90-250 mg codeine, 300-400 mg tramadol, or 15 to 40 mg oxycodone) should start with the 10 μg/hour patch. Transdermal buprenorphine is not appropriate for patients taking over 80 mg morphine or equivalent.
Buprenorphine is a Schedule III drug according to the U.S. [Drug Enforcement Administration (DEA) criteria [47] For reference, heroin is a Schedule I drug while fentanyl, morphine, and oxycodone are Schedule II drugs. Schedule III drugs are considered to have less abuse potential than Schedule I or II drugs. Opioids may vary in their attractiveness to opioid abusers or in terms of so-called “drug liking” [48].In a double-blind, placebo-controlled study of morphine-maintained heroin abusers, buprenorphine injection was described as being only of moderate interest to no interest to abusers [49]
Managing Side Effects
Pain relief must be balanced against tolerability. Optimized analgesia can often be achieved when clinicians proactively or promptly address side effects. Common opioid-associated side effects include nausea and vomiting.. Opioid analgesia should not be avoided because of the risk of nausea and vomiting, since the majority of patients will not experience this effect and it is manageable in patients who do. Nausea and vomiting can be addressed with prophylactically administered antiemetics, with dopamine-receptor antagonists (for instance, metoclopramide or haloperidol), histamine-receptor antagonists (e.g., dimenhydrinate), muscarinic-receptor antagonists (e.g., hyoscine patch), serotonin-receptor antagonists (e.g., ondansetron), and other agents, and even withnonpharmacological treatment (ginger, for example). There is no strong clinical evidence favoring one particular antiemetic over others.
Patients who take opioids for more than a few days should be expected to experience some degree of constipation; about half of patients will likely experience it [30] and this side effect is unlikely to diminish with time. A bowel regimen can be started when opioid therapy begins and patients should be educated about constipation treatment options.
At high doses, opioids are associated with potentially lifethreatening respiratory depression. It should be noted in this connection that buprenorphine, unlike morphine or oxycodone, has a “ceiling effect” for respiratory depression [38]. Ceiling effect occurs when a dosage increase above a certain point no longer has any effect.
Strategies and Tactics for Chronic Postoperative Pain Control
Patients dealing with CPSP require education about the nature of their pain and potential therapies. It is particularly important for the clinician to set realistic patient expectations, that is, chronic pain can be managed and controlled, but it is not always possible to eliminate it entirely. Furthermore, patients should be educated about side effects and encouraged to report them,because in many cases they can be effectively managed. See Figure 1.
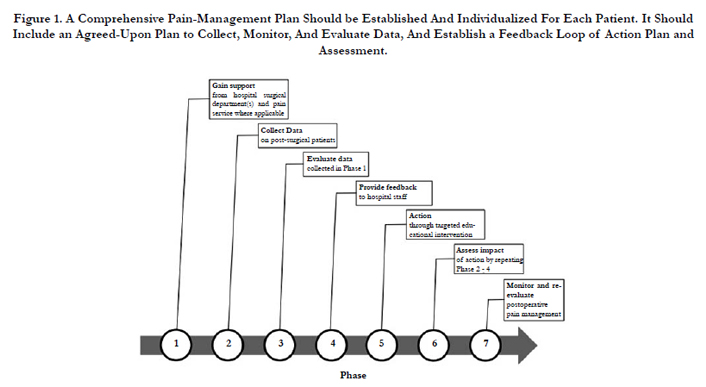
Figure 1. A Comprehensive Pain-Management Plan Should be Established And Individualized For Each Patient. It Should Include an Agreed-Upon Plan to Collect, Monitor, And Evaluate Data, And Establish a Feedback Loop of Action Plan and Assessment.
While opioids are effective pain relievers, clinicians should consider ways to optimize nonopioid pain relievers and even nonpharmacological options for long-term pain therapy. For instance, fixed-dose combination products may reduce overall opioid consumption. Non pharmacological treatments, such as physical therapy, may provide some degree of pain relief that may be sufficient to reduce or eliminate the use of opioid analgesics. It is important that chronic pain patients participate in their pain therapy and recognize that there is no “magic pill” or cure.
Nonopioidanalgesics can be important agents in the care of CPSP patients, but all of them, including NSAIDs and paracetamol, have risks [50-52] In all cases, patients should be educated about risks and benefits, and the agents should be taken in as low a dose as possible for the shortest period of time.
Opioid therapy may be needed to address moderate to severe pain [53,54] If oral opioids are prescribed, it may be desirable that the pill burden be minimized as much as possible. When prescribing opioids for CPSP patients, the issue of inappropriate use or abuse must be considered [55] Patients should be educated about appropriate use of opioid agents and monitored closely. Some physicians encourage treatment agreements or contracts which spell out in plain language the terms of opioid therapy [56] These treatment contracts may explain that the patient could be subjected to random urine tests or pill counts [57,58] Transdermal formulations might offer an advantage in this setting [47]. In all cases, thorough documentation is required, but while close clinical supervision is desirable for optimal outcomes, the tendency to “overmanage” should also be avoided, since it takes time for drug steady state to be reached (sometimes even two or three weeks).
Clinicians must also recognize that not all patients are appropriate candidates for opioid therapy [59]
Conclusion
CPSP is prevalent and often suboptimally treated. Patients who have persistent pain following surgery should be evaluated, and their pain managed. This includes considering non pharmacological pain treatments, selecting the optimal pharmacological product(s) if needed, educating the patient, and managing potential adverse events proactively. Transdermal buprenorphine may be a good option for many such patients in that it is an effective analgesic product with convenient dosing, potentially lower abuse potential, and suitability for older and renally-compromised patients. There are many safe and effective analgesic products available, and clinicians should find the optimal nonpharmacologic or pharmacologic therapy, or combination, for the individual patient.
References
- Apfelbaum JL, Chen C, Mehta SS, Gan TJ (2003) Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesthesia and analgesia. 97(2):534-540.
- Reddi D, Curran N (2014) Chronic pain after surgery: pathophysiology, risk factors and prevention. Postgrad Med J. 90(1062): 222-227.
- Crombie I, Davies H, Macrae W (1998) Cut and thrust: antecedent surgery and trauma among patients attending a chronic pain clinic. pain. 76(1-2):167-171.
- Ravindran D (2014) Chronic postsurgical pain: prevention and management. J pain palliat care pharmacother. 28(1): 51-53.
- Gerbershagen HJ (2013) [Transition from acute to chronic postsurgical pain. Physiology, risk factors and prevention]. Schmerz. 27(1): 81-93.
- Albrecht E, Taffe P, Yersin B, Schoettker P, Decosterd I, et al., (2013) Undertreatment of acute pain (oligoanalgesia) and medical practice variation in prehospital analgesia of adult trauma patients: a 10 yr retrospective study. Br J Anaesth.110(1): 96-106.
- Alexander JH, Manno M (2003) Underuse of analgesia in very young pediatric patients with isolated painful injuries. Ann Emerg Med. 41(5): 617-622.
- Cinar O, Ernst R, Fosnocht D, Carey A, Horne B, et al., (2012) Geriatric patients may not experience increased risk of oligoanalgesia in the emergency department. Ann Emerg Med. 60(2): 207-211.
- Chen EH, Shofer FS, Dean AJ, Robey JL, Mills AM, et al., (2008) Gender disparity in analgesic treatment of emergency department patients with acute abdominal pain. Acad Emerg Med.15(5): 414-418.
- Joshi GP, Beck DE, Emerson RH, et al. Defining new directions for more effective management of surgical pain in the United States: highlights of the inaugural surgical pain congress. The American surgeon. Mar 2014;80(3):219-228.
- Voscopoulos C, Lema M (2010) When does acute pain become chronic? BJA.105(1): i69-i85.
- Apkarian AV, Baliki MN, Farmer MA (2013) Predicting transition to chronic pain. Curr opin Neurol. 26(4): 360-367.
- Deumens R, Steyaert A, Forget P, et al., (2013) Prevention of chronic postoperative pain: cellular, molecular, and clinical insights for mechanism-based treatment approaches. Prog Neurobiol.104:1-37.
- Katz J, Seltzer Z (2009) Transition from acute to chronic postsurgical pain: risk factors and protective factors. Expert Rev Neurother. 9(5): 723-744.
- Wu CL, Raja SN (2011) Treatment of acute postoperative pain. Lancet. 377(9784): 2215-2225.
- Perkins FM, Kehlet H (2000) Chronic pain as an outcome of surgery. A review of predictive factors. Anesthesiology. 93(4):1123-1133.
- Coley KC, Williams BA, DaPos SV, Chen C, Smith RB (2002) Retrospective evaluation of unanticipated admissions and readmissions after same day surgery and associated costs. J clin Anesth. 14(5): 349-353.
- Williamson A, Hoggart B (2005) Pain: a review of three commonly used pain rating scales. J clin Nurs.14(7): 798-804.
- Hjermstad MJ, Fayers PM, Haugen DF, Caraceni A, Hanks Gw, et al., (2011) Studies comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for assessment of pain intensity in adults: a systematicliterature review. J pain symptom Manage. 41(6):1073-1093.
- World Health Organization (1988) WHO's cancer pain ladder for adults, 2013.
- International Pain Summit Of The International Association For The Study Of P (2015) Declaration of Montreal: declaration that access to pain management is a fundamental human right. J pain palliat care pharmacother. 25(1): 29-31.
- Davis MP (2007) What is new in neuropathic pain? Supportive care cancer. 15(4): 363-372.
- Raffa RB (2001) Pharmacology of oral combination analgesics: rational therapy for pain. J clin pharm ther. 26(4): 257-264.
- Tallarida RJ, Raffa RB (1996) Testing for synergism over a range of fixed ratio drug combinations: replacing the isobologram. Life sci. 58(2): 23-28.
- Raffa RB, Clark-Vetri R, Tallarida RJ, Wertheimer AI (2003) Combination strategies for pain management. Expert opin pharmacoth. 4(10): 1697-1708.
- Anitescu M, Benzon HT, Argoff CE (2013) Advances in topical analgesics. Curr opinion Anaesthesiol. 26(5): 555-561.
- Vas L, Khandagale N, Pai R (2014) Successful management of chronic postsurgical pain following total knee replacement. Pain med. 15(10):1781- 1785.
- Phillips K, Clauw DJ (2011) Central pain mechanisms in chronic pain states--maybe it is all in their head. Best Pract Res Clin Rheumatol. 25(2): 141-154.
- Dowell D, Haegerich T, R C (2016) CDC Guideline for prescribing opioids for chronic pain - United States, 2016. MMWR Recomm Rep. 65(1):1-49.
- Lin TC, Hsu CH, Lu CC, Tsai YC, Ho ST (2010) Chronic opioid therapy in patients with chronic noncancer pain in Taiwan. J Anesth. 24(6): 882-887.
- Polomano RC, Heffner SM, Reck DL, Gelnett CM, French D (2001) Evidence for opioid variability, Part 2: Psychosocial influences. Semin perioper Nurs. Oct 10(4):159-166.
- Gilson AM, Maurer MA, Joranson DE (2007) State medical board members' beliefs about pain, addiction, and diversion and abuse: a changing regulatory environment. J Pain. 8(9): 682-691.
- Manchikanti L (2006) Prescription drug abuse: what is being done to address this new drug epidemic? Testimony before the Subcommittee on Criminal Justice, Drug Policy and Human Resources. Pain physician. 9(4): 287-321.
- Mercadante S (2007) Opioid titration in cancer pain: a critical review. Eur J pain.11(8): 823-830.
- McCracken LM, Hoskins J, Eccleston C (2006) Concerns about medication and medication use in chronic pain. J Pain. 7(10): 726-734.
- Schieffer BM, Pham Q, Labus J, Baria A, Davis P, et al., (2005) Pain medication beliefs and medication misuse in chronic pain. J Pain. 6(9): 620-629.
- Ho AH, Chan CL, Leung PP, Pang SM, Tse DM, et al., (2013) Living and dying with dignity in Chinese society: perspectives of older palliative care patients in Hong Kong. Age Ageing. 42(4): 455-461.
- Pergolizzi J, Aloisi AM, Dahan A, Filitz J, Likar R, et al., (2010) Current knowledge of buprenorphine and its unique pharmacological profile. Pain pract. 10(5): 428-450.
- Budd K, Raffa R (2005) Buprenorphine - The unique opioid analgesic: Pharmacology and clinical Application. Stuttgart, Georg Thieme, Germany.
- Raffa R, Ding Z (2007) Examination of the preclinical antinociceptive efficacy of buprenorphine and its designation as full- or partial-agonist. Acute Pain. 9(3): 145-152.
- Karlsson M, Berggren AC (2009) Efficacy and safety of low-dose transdermal buprenorphine patches (5, 10, and 20 microg/h) versus prolonged-release tramadol tablets (75, 100, 150, and 200 mg) in patients with chronic osteoarthritis pain: a 12-week, randomized, open-label, controlled, parallelgroup noninferiority study. Clinical Ther. 31(3): 503-513.
- James IG, O'Brien CM, McDonald CJ (2010) A randomized, double-blind, double-dummy comparison of the efficacy and tolerability of low-dose transdermal buprenorphine (BuTrans seven-day patches) with buprenorphine sublingual tablets (Temgesic) in patients with osteoarthritis pain. J pain symptom Manage. 40(2): 266-278.
- Gordon A, Callaghan D, Spink D, Darke Ac, Buckley N, et al., (2010) Buprenorphine transdermal system in adults with chronic low back pain: a randomized, double-blind, placebo-controlled crossover study, followed by an open-label extension phase. Clin Ther. 32(5): 844-860.
- Pergolizzi J, Boger RH, Budd K, Dahan A, Hans G, et al., (2008) Opioids and the management of chronic severe pain in the elderly: consensus statement of an International Expert Panel with focus on the six clinically most often used World Health Organization Step III opioids (buprenorphine, fentanyl, hydromorphone, methadone, morphine, oxycodone). Pain pract.8(4): 287-313.
- Likar R, Vadlau EM, Breschan C, Kager I, Korak-Leiter M, et al., (2008) Comparable analgesic efficacy of transdermal buprenorphine in patients over and under 65 years of age. Clin J pain. 24(6): 536-543.
- Johnson RE, Fudala PJ, Payne R (2005) Buprenorphine: considerations for pain management. J pain Symptom Manage. 29(3): 297-326.
- DEA (2013) Buprenorphine. Drug & Chemical Evaluation Section, 2014.
- Kelley A, Berridge K (2002) The neuroscience of natural rewards: relevance to addictive drugs. J Neurosci. 22(9): 3306-3311.
- Comer SD, Sullivan MA, Whittington RA, Vosburg SK, Kowalczyk WJ (2008) Abuse liability of prescription opioids compared to heroin in morphine- maintained heroin abusers. Neuropsychopharmacology.33(5): 1179-1191.
- Ong HT, Ong LM, Tan TE, Chean KY (2013) Cardiovascular effects of common analgesics. Med J Malaysia. 68(2): 189-194.
- Biskupiak JE, Brixner DI, Howard K, Oderda GM (2006) Gastrointestinal complications of over-the-counter nonsteroidal antiinflammatory drugs. Journal of pain & palliative care pharmacotherapy.20(3): 7-14.
- Yuan L, Kaplowitz N (2013) Mechanisms of Drug-induced Liver Injury. Clin Liver Dis. 17(4): 507-518.
- Opioids for persistent pain: Good practice (2010) The British Pain Society,London.
- Chou R (2009) Clinical Guidelines from the American Pain Society and the American Academy of Pain Medicine on the use of chronic opioid therapy in chronic noncancer pain: what are the key messages for clinical practice? Pol Arch Med Wewn. 119(7-8): 469-477.
- Manchikanti L, Abdi S, Atluri S, Balog CC, Benyamin RM, et al., (2012) American Society of Interventional Pain Physicians (ASIPP) guidelines for responsible opioid prescribing in chronic non-cancer pain: Part 2--guidance.Pain physician. 15(3): S67-116.
- Anderson E, Burris S (2010) Opioid treatment agreements are the answer. What is the question?, Am J Bioethics. 10(11): 15-17.
- Pergolizzi J, Pappagallo M, Stauffer J, Gharibo C, Fortner N, et al., (2010) The role of urine drug testing for patients on opioid therapy. Pain Pract. 10(6): 497-507.
- Katz NP, Sherburne S, Beach M, Rose RJ, Vielguth J, et al., (2003) Behavioral monitoring and urine toxicology testing in patients receiving long-term opioid therapy. Anesth Analg. 97(4): 1097-1102.
- Ho KY, Chua NH, George JM, Yeo SN, Main NB, et al., (2013) Evidencebased guidelines on the use of opioids in chronic non-cancer pain--a consensus statement by the Pain Association of Singapore Task Force. Ann Acad Med Singapore. 42(3): 138-152.





