Gonorrhea infection and sexual behaviors-A qualitative study of South African women
Ndwanya TW*, Kumar V, Panas R
Walden University, Minneapolis, MN, USA.
*Corresponding Author
Takiyah White Ndwanya Ph.D., MPH,
Walden University,
Minneapolis, MN, USA 55401.
Tel: +27 073 696 5214
E-mail: Takiyah.White@gmail.com
Received: February 16, 2016; Accepted: March 11, 2016; Published: March 18, 2016
Citation: Ndwanya TW, Kumar V, Panas R (2016) Gonorrhea Infection and Sexual Behaviors-A Qualitative Study of South African Women. Int J Reprod Fertil Sex Health. 3(1), 57-65. http://dx.doi.org/10.19070/2377-1887-1600011
Copyright: Ndwanya TW© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
In South Africa, the incidence of gonorrhea is highest among Black women due to their high co-infection rates with HIV and other sexually transmitted infections (STIs). This is alarming because of the emergency of antibiotic-resistant forms of the disease. This study examined the psychosocial determinants of gonorrhea among Black women aged 18 – 35 in the Langa township in Cape Town, South Africa. All participants reported at least one sexual experience and one positive test for gonorrhea in the past two years. Participant recruitment was flyer distribution at Love Life, the community partner to the research study. After an initial screening call, 12 women were considered eligible and participated in the study. Interview data were gathered, transcribed, then hand-coded for emergent themes, guided by the tenets of the information-motivationbehavioral (IMB) skills conceptual framework. The study contributes to existing literature on psychosocial determinants that have a positive relationship to the etiology of gonorrhea among African Black women and to form the basis of larger quantitative studies. Findings in this study were that the access to risk reduction information with consistency and motivation to change risky behaviors are affected by a woman’s sense of how much control she has in her relationship. Interpersonal factors such as sexual inequalities where the males have prevalence of sexual power and control tend to take risk-reduction information and motivation out of the hands of the women. Environmental and cultural limitations caused pressure to engage in risky behaviors that led to heightened risk of gonorrhea.
2.Introduction
3.Materials and Methods
4. Results and Discussion
4.1. Individual Factors/Information
4.2. Individual Factors/Motivation
4.3. Relationship Factors/Behavioral Skills
4.4. Social Factors/Behavioral Skills
5. Acknowledgement & Declaration
6.References
Keywords
Depression; Pain; Endometriosis; Family History; Grades.
Introduction
Gonorrhea is the most common bacterial STI (sexually transmitted infection) in the world. It affects women at an alarming rate compared to men and is mostly contracted through heterosexual sex. In the beginning of the 21st century, an increase in gonorrhea incidence has been observed globally due to the emergence of antibiotic-resistant strains of the disease. The incidence of gonorrhea is highest in developing countries although more than 300,000 cases are annually reported in the United States [1]. Coinfection with HIV is currently a concern with distribution of gonorrhea among teenagers and young adults. Young women in South Africa are at greatest risk of being infected with HIV, the prevalence in the age group 15 to 24 is 16.9% in women and 4.4% in men in 2005 [2]. The high prevalence among women is thought to be because of “poverty, violence against women, cultural limitations that promote intergenerational sex, non-condom use and preference for ‘dry sex’ (sex without lubrication and with inanimate objects), political factors and challenges that possibly prevented an aggressive response against HIV, recreational drug use, and biological factors such as high prevalence of STIs” [2].
According to the Centers for Disease Control and Prevention [3] overall in 2009, 23.5% of isolates collected in the United States from 29 Gonococcal Isolate Surveillance Project (GISP) sites (established in 1986) “were resistant to penicillin, tetracycline, ciprofloxacin, or some combination of those antibiotics.” Antimicrobial resistance (AMR) to gonorrhea is the main bacterial agent that is an issue in South Africa. Because of the high degree of infectiousness, South Africa has the most active antibiotic surveillance of any African country, which is done by the STI Reference Centre in collaboration with the National Department of Health (NDoH). AMR is driven by factors such as inappropriate antibiotic management and consumption, the regulatory environment, knowledge of health care workers, and patient expectations [4]. In 2006 in South Africa, medical practitioners warned of growing resistance to gonorrhea drug therapy, as a study found that 60% of gonorrhea patients in a Durban clinic showed resistance to ciprofloxacin, a 43% increase over the 42% resistance level in 2005 [5]. Researchers also found that 29% of patients at a clinic in Johannesburg failed to respond to ciprofloxacin, compared to a 16% resistance level in 2005 [5]. These statistics are important because they highlight a growing rate of antibiotic-resistant gonorrhea that has the potential to affect the most sexually at-risk groups inclusive of Black women in South Africa.
The worldwide incidence of curable sexually transmitted infections (STIs), those with established treatment methods, has been estimated only from prevalence data and the estimated duration of infection because few countries outside Western Europe and North America have accurate reporting systems for STIs [6]. Surveillance to monitor susceptibility of patterns of the bacterium N. gonorrhoeae is also not a regular feature of the national STI control program in South Africa, as surveillance occurs mainly in research settings [7]. It is a regular feature in the United States, as the CDC has both monitoring and evaluation of gonorrhea that is to be reported in all clinical and community health facilities, and the data are available as a public feature on their website stratified according to demographics and geographic locations within the United States.
The reason for the review of the gonococcus N. gonorrheae in this particular study is because Black women are disproportionately affected by the STI. This study addressed the perceptions of Black women in South Africa and the psychosocial determinants of gonorrhea. The demographics and psychosocial factors of this particular test group are associated with a higher susceptibility to STIs. The qualitative study design allowed study participants to speak freely and without restrictions concerning the experiences and motivations that may have led to their increased risk of STIs, in particular gonorrhea. The research question was: What is the experience of South African women regarding the psychosocial determinants of gonorrhea?
The purpose of this research was to detemine the psychosocial factors and intrapersonal aspects among women from Cape Town, South Africa regarding the incidence of gonorrhea. The psychosocial determinants found in literature that have an effect on incidence of gonorrhea in South Africa are identified as per the IMB conceptual framework is found on the individual level, in partner relationships, and in society. Individual factors include information (knowledge of risk), substance abuse, and mental health. Partner relationship dynamics include sexual power and gender based violence. Society is inclusive of socio-economic status (SES) and cultural limitations.
South Africa, the geographic target of this study was a sentinel area for study because even now there is no national surveillance being done in regards to gonorrhea rates to coincide with HIV and syphilis epidemiological rates, although it is drastically necessary because of the impending pandemic crisis of quinolone resistant N. gonorrhoeae (QRNG) currently being seen in the United States and other countries abroad. A method to prevention that can be done to assist in deterring QRNG from affecting Black women in high risk environments and populations specifically in the Western Cape of South Africa (Cape Town area) is to focus on psychosocial aspects that can have an impact on burden of disease, whether they are on an individual, relational, or social level.
Psychosocial conditions began as a result of the need for epidemiologists to understand how disease and social experiences affect health outcomes. These factors are found around the world as affects to STIs and in particular, gonorrhea. This study addressed the factors sentinel to risk of gonorrhea among Black women in Cape Town, South Africa and will contribute to literature concerning tailoring interventions among populations at high risk of gonorrhea.
Materials and Methods
Qualitative methods was chosen after reviewing the literature with an emphasis on Black women regardless of geographic location because it allowed the participant to feel more at ease with the process of the research being in their home area. The data collection methods applied individual interviews to allow the women study participants to share their ideas on the psychosocial and behavioral manifestations that affect their sexual habits.
The IMB skills theory was the framework to help construct the interview questions and frame the results. The theory defines the constructs in which women can share their ideas on the psychosocial and behavioral manifestations that affect their sexual habits to examine similarities with Black women (Figure 1). In order to do this, themes from open-ended questionnaires and focus groups that are characteristic of qualitative methodology was the theoretically ideal structure for this study.
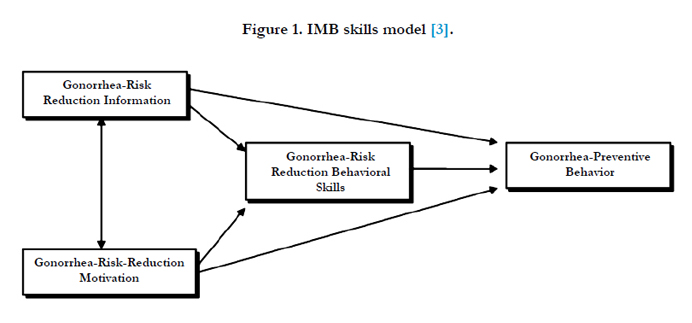
Figure 1. IMB skills model [3]
Results and Discussion
The data collection of the study was based in Langa, a suburb township in Cape Town that is well known for its history during the Apartheid. Langa means “sun” and is one of the oldest townships in Cape Town. Out of the research participants (Table 1), 92% of the women were unemployed, 58% were high school graduates (25% had less than a grade 12 education, and 17% were university students). All of the participants considered themselves single, but 67% were in a relationship, and 33% were single, not in a relationship. The average age of the study participants was 21.7 years old. Antimicrobial resistance was found to be the case in three of the participants interviewed or 25% of the subject population. Though not probed with questioning, three of the women stated that they had to be retreated at the local clinic due to the first round of antibiotics not working. One of the women said that it was probably due to her partner refusing to seek treatment and inferred that her being retreated was probably due to re-infection by her untreated partner. For the other two cases, the women were given another round of antibiotics (presumably ceftriaxone) whose disease failed to respond to the first-line treatment of ciprofloxacin.
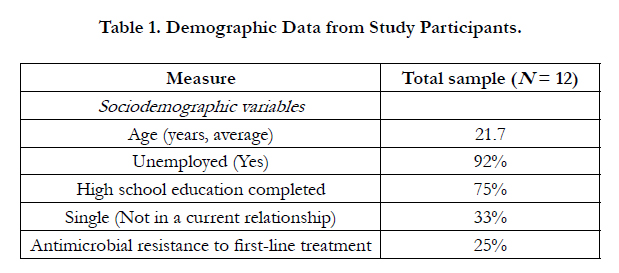

Table 1. Demographic Data from Study Participants.
LoveLife, a non-profit organization was the community partner in Langa that was the site of the participant interviews and where participant flyers were housed and distributed for recruitment.
This research confirmed that addressing social and structural barriers that increase risk to STI infection-two of the key strategic objectives for the South African National AIDS Council’s National Strategic Plan [11]--is critical to decreasing sexual disease epidemics that affect the country, in particular impoverished areas that have limited basic resources. The research supports and confirms that there is a need for more nationally representative STI prevalence studies to monitor trends and success of STI treatment facilities and initiatives, especially in township clinics. Many of the women were treated and sent away with no follow-up on at-risk behavior changes and risk of reoccurrence of gonorrhea, as some of the women claimed that their partner would not go to receive treatment due to the unbelief that they had contracted gonorrhea out of the relationship or that they were given the disease by their partner.
The individual factors that affect women - the access to risk reduction information (from the IMB model) their motivation (from the IMB model) to change risky behaviors that are affected by how much control they have in their relationship, which for many women is high because of high unemployment and dependence on their partner. Some of the women with an association of higher education - currently in tertiary education, tend to have more information, self-esteem, and knowledge of preventive behaviors, resulting in positive motivation for providing contraception for HIV/STI preventive behavior especially after having a positive diagnosis of gonorrhea. Other individual factors such as alcohol dependence especially during social activities, and stress and depression from relationship woes tend to negatively affect risk-reduction behaviors (from the IMB model) increasing risk of gonorrhea among other STIs and HIV.
Partnership factors such as sexual inequalities where the males have prevalence of sexual power and control, tend to make riskreduction information and motivation out of the hands of the women also lowering risk-reduction sexual behaviors in women creating preventive behavior null and void. Gender based violence in the African Black township community is so pervasive that most women know or have experienced this in their relationship. The result of this violence is reoccurrence and increased risk to women for basic needs and thus, lack of motivation to practice preventive sexual behaviors.
Social factors of the environment consist of many pressures found among the women, i.e. friends and family that influence women to maintain a relationship in order to have personal needs or family needs met when poverty runs rampant in her community. Cultural limitations still prevail in the African Black townships and this was also seen among the women where men are seen as dominant and of the greatest power in the relationship. Women look to them as being responsible for contraception, although culturally and spiritually, pre-marital sex is not favorable. Even though this was seen among some women, there were some that felt more emancipated and independent and felt that high self-esteem and education are important in being motivated to make preventative decisions about sexual behavior.
The findings of this research are delineated within the three fundamental determinants of gonorrhea: risk-reduction information, gonorrhea risk-reduction motivation, and gonorrhea risk-reduction behavioral skills. The framework is not linear, as the modules work synergistically with each other to obtain the desired result of no disease within an at-risk population.
This refers to the means of disease transmission and information concerning methods of preventing infections as a requisite of risk-reduction behavior.
Theme 1: Knowledge of risk. South African women were knowledgeable about STIs, but not specific STIs, including gonorrhea. The respondents frequent LoveLife, a non-profit organization that promotes positive sexual choices and prevention of sexually transmitted diseases in underrepresented communities in South Africa. The organization is well funded by overseas donors and has a broad reach in many untouched township areas that are devoid of many resources that are offered in more affluent communities in South Africa, in particular Cape Town. Although the participants were well aware of the publications, activities, and services offered by LoveLife, including a television soap opera that nationally promotes safe sex to avoid HIV/AIDs, the women were still very susceptible to STIs, in particular gonorrhea.
Gonorrhea is not a household word used; and even at LoveLife, gonorrhea is grouped under the heading of STIs. The women were shocked and did not feel at risk for this disease because they were unaware of the burden of the disease other than it could be cured through antibiotics. In the township clinics, the nurses do not typically give statistics and risk factors for gonorrhea, which poses a significant threat to this population becoming sentinel to resistant forms of gonorrhea due to the lack of understanding and knowledge of the disease.
Most of the women did not speak to their partners whether casual or in exclusive relationships, and, in most cases, the conversation only began after receiving a positive diagnosis and subsequenttreatment. Many of the women were trusting of their partner and felt that contraception should be his responsibility, and if protection was not used, it was a sign of commitment or exclusivity. This false sense of knowledge of STIs led to a false sense of risk of infection.
Based on the interviews, few women understood their risk of gonorrhea. One of the participants commented that although prevention information is given at local clinics and NGOs, the knowledge is not practiced.
Yes, we do [get education on gonorrhea and HIV] and no one takes it seriously. Or they know and don’t really want to practice it in their lives. It passes through their mind.
The women found that the relationships and casual encounters that they obtained gonorrhea from were not conducive to a constant reminder and communication about the possibility of the risk of any diseases.
Not much [to the type of discussion had regarding STIs before the positive result]. Nothing like that we talked about. STIs, we literally didn’t talk about it.
The conversation in many of the cases was delayed and tended to occur after the positive diagnosis and subsequent treatment.
No, [did your partner ever tell you that he had gonorrhea or any STIs] and I didn’t ask as well.
“No, we didn’t talk about it. Didn’t think about it actually. I didn’t know we would get to that stage so soon. So it just happened.”
The participants who tended to have more education, that is, those who were currently in varsity or receiving formal tertiary education, were more vocal on the impact that having consistent conversations with partner(s) have on positive, gonorrhea reinfection free relationships.
Not, very much [confidence with using condoms and condom negotiation]. It’s very important to use condoms, especially after that experience at a very young age. After that, I was like condoms all the way. If there are no condoms, there is no sex. It’s just like that. We don’t even have to discuss it.
Although the participants were well aware of the publications, activities, and services offered by LoveLife, including a television soap opera that nationally promotes safe sex to avoid HIV/AIDs, the women were still unaware that they were at risk of getting gonorrhea.
These findings extend the knowledge of what we know about this target population and also confirm that the lack of constant exposure to information of STIs, which makes the population more susceptible to the disease. Even tertiary level education participants are in need of constant information exposure to eliminate the risk of gonorrhea and could be used as a resource to spread preventable behavior information to the less educated and younger groups in the townships to help to eliminate the potential epidemic of the microbial resistant form of gonorrhea.
The desire to change at-risk behavior in order to prevent STI transmission and prevention. A majority of women in the study were adamant that after having a positive gonorrhea diagnosis, they are fully confident and motivated to practice safer sex.
Theme #2: Alcohol consumption. The motivation to change risky behaviors because it encourages sexual risk taking. In the Langa Township, a predominately Black African township, alcohol use is significantly high among women [13]. The main question used to find out use of substances and their influence on sexual behavior during the interview was “Could you tell me about any contact you have had with substance abuse (alcohol or drugs) and how that might have affected your sexual activities?”Conversely to the research by Myers and Wechsberg [13, 14] the women did not report drug use with heavy drinking, but mostly social drinking. The drinking did, however, contribute to risky sexual behavior, and the women did get gonorrhea because of this behavior. One woman in particular was placed in a dangerous position of almost being
raped as a result of becoming weak while drinking, and another reported that she has seen many women in informal taverns or bars get taken advantage of while drinking heavily.
This was found to be an issue with some of the women who participated in the study. One of the participants admitted that the contact she has had with alcohol has had an ill effect on sexual behavior.
With alcohol, I am weak when I drink. I can drink one cider and that is enough for me. [They] caught him before he took advantage of me.Another participant made the association with alcohol substance abuse with women in her community that attend taverns (informal bars that are located in the township).
Because some other girls are weak, so they get drunk and become weak, so people get their chances to take the, go with them, do things with them like rape them.
A final participant explained that she and her partner use alcohol frequently and attend taverns together. According to her, this has limited the amount of cheating that occur in the relationship according to her accounts and that when they used to drink independent of each other, it influenced and affected their relationship negatively. Based on the interviews, there were no issues with other drug use (AOD).
In this particular theme, there was no finding that extends the research but concurs with the notion that alcohol consumption does have an effect on motivation to engage in risky behaviors that have led to gonorrhea.
Theme #3: Stress or depression.This affects the mental health of women because relationship issues and mistreatment influences the motivation of whether a woman will prevent risky behavior or not. These stressors led to depression and low self-esteem among many of the participants. Questions in the interview relating to this psychosocial factor were the following:
- Have you ever had feelings of depression due to individual stress from your relationship? Tell me how depression was a cause for engaging in sexual behavior.
- Has low self-esteem ever been a reason to engaging in sexual behavior? How have you made this connection?
- What type of things stress you out at home?
- How does this stress affect your relationships?
- How have feelings of loneliness or depression affected your sex life?
The women noted that they are often not asked about coping mechanisms and ways of dealing with stress and depression, as also found in literature that this phenomenon is often neglected in South African women. Women were found to be significantly more likely than men to suffer from depressive disorders, and this research can conclude that a majority of the women deal with depression and anxiety because of poverty, lack of a stable home structure, and issues in their relationship [15].
Mental health concerns were found to be true with some of the women in the study. Mainly as a result of relationship issues and mistreatment by their partner were the main causes of stress leading to depression and low self-esteem. When asked if the participant (#12) ever felt depressed or stressed in her relationship with her boyfriend, she responded by saying,
Yes [because of depression or stress] that time when I had gonorrhea and he left and didn’t come back. When he came back, he shouted and said he didn’t want me. And then I go and then sometimes when you love a person, you love serious. And I go and ask him, please come back with me I love you, but he came for that time and left and left and stayed with me when he saw that I love him. We are in a good relationship now.
Some of the depression came as a result of the positive gonorrhea result at the clinic:
I was depressed when I heard that I’ve got—when I went to the clinic and found out that I had gonorrhea. So I was very depressed because I trusted him a lot and now to have this like it was very painful and stressful.
Feelings of depression or sadness affected progress while in school:
I think so at some point [stress or feelings of depression or sadness] there is cheating. I felt betrayed because he said so many things and when you are in love, you believe. So I believed him and trusted him with my life by not using a condom. I could have contracted anything and I did. I wasn’t depressed to the max. Imagine if it was HIV, I would still have it. So, I was like okay and couldn’t concentrate in school, but was able to pass that year. Not with the marks I wanted, but I did make it through.
Although none of the participants stated that they suffer from clinical mental disorders, they do however have stress and anxiety because of instances concerning their relationships and lack of home structure and security (poverty). One participant (#9) stated:
Me, yes [things at home that stress you out] there is a lot. Which is why I don’t think a relationship is good for me right now. If someone passes away, like my grandmother, we got split up and that caused a lot of issues and fights in my family. With my boyfriend, I felt safe and happy to be there. When it was time to go home, I wasn’t happy because there were fights about food, who must cook and clean and you become tense. When I go home I keep quiet, I go to my room, lock the door and keep to myself. I have a diary and write in it. I took my problems out in the diary and no one can read it. When I read it, I cry, and listen to my music, but it helps me. At least I’m taking stress out in my diary. I am coping.
Another participant (#10) noted stress from home due to family concerns:
I have a brother in gangsterism, whenever there is a dead person reported, you wonder where he is because he is not home and that is the stress that I get.
The findings from this study add to the literature that mental health among this population is important to further explore in relation to sexual behaviors. The women have stressors that should not be ignored in the home and in her relationships. Once her mental health has been evaluated by trained health practitioners through caring networks, support structures among peer groups and family should be instituted to help with establishing coping mechanisms that can raise self-esteem and empowerment among this high risk group.
Behavior skills refer to performing specific gonorrhea preventive acts. The women felt that better communication and insistence of monogamy in her relationship were factors that allowed for more positive preventive sexual behaviors. For the majority of women, when diagnosed with gonorrhea, they refrained from sexual contact with their partner unless he was tested and treated (if a positive diagnosis) for the disease. This was only observed in the women that showed sexual power within her relationship.
Theme #4: Sexual inequalities. A woman’s status or power in the household and in relationships and their effects on contraceptive use. Participants in the study were either very confident and had high self-esteem and self-efficacy when it came to condom negotiation and use after receiving a positive gonorrhea diagnosis or had a lack of sexual power in the relationship resulting in low self-esteem and low self-efficacy in condom negotiation. It was certain that women were taking more responsibility for contraception than before the diagnosis because it became aware that although the majority did not feel at risk initially for STIs, they are actually susceptible to sexually transmitted infections and are now fearful of getting an untreatable disease that could affect their lives, thus behavior change is greater than before getting gonorrhea. In those relationships where sexual inequality was identified, issues in partner controlling behavior and relationship dynamics where physical violence was evident, infidelity was found to be common in the interviews. Questions in the interview to identify sexual inequalities were as follows:
- What sexual practices would you refrain from performing if you or your partner had gonorrhea?
- How confident are you with using condoms and are you able to negotiate with your partner to use condoms if you are not in a monogamous relationship?
- How confident are you to refuse sexual intercourse with your partner if they choose not to use a condom?
- What are your feelings of personal control in your relationship or with sexual partners?
Gender-based sexual power inequality was observed through the study participants that included issues with infidelity with partners and lack of relationship control leading to inconsistency in condom use. One participant (#9) stated when asked “How confident are you with using condoms? Are you able to talk to your partner about using them” that:
I’m 100% confident. I have been taught at school and at home, but it becomes a challenge when it is you and your boyfriend when he doesn’t want to use a condom and then you have to settle with him and you don’t want him to leave you. If he doesn’t want to use one, then maybe you should go for a contraception, but the chance for getting HIV and STI is 100%, but only the pregnancy will be safe with contraception.
Another participant realized that with lack of sexual power in the relationship can cause a lack of self-esteem:
Participant (#7):
Sometimes we fight about using condoms because he doesn’t want to use condoms most of the time. [Why is that? Is it because you are in a relationship?] Yes because we are in a relationship. There is no use in using condoms. [Do you have high self-esteem or low self-esteem? What type of person are you?] Low self-esteem. I really don’t know. [What were your feelings of control in the relationship? Did you feel in control of the relationship?] He is very controlling.
The lack of fidelity in relationship dynamics caused physical violence.
Participant (#12):
I did get it from him [gonorrhea from my boy friend] because he was cheating with the neighbor next to me. That girl used to be in taverns and when I told him it was him, we started fighting. [Before getting gonorrhea, did you ever talk about using condoms or STIs?] We always talk about it and use condoms. When he say no condoms today, I say no and we fight about it. And when I say no, I say no. Even when I don’t want to have sex and he wants, I say no I don’t want. No is no. [Is he fine with that now?] Yes, he was not fine before, but now he ends up knowing me when I say no I mean no.
The findings in this study confirm that gender-based sexual power inequality is found among the women and does affect sexual behavior in casual and monogamous relationships. Infidelity was found to be common among the women’s partners but not for them, and if the women questioned the behavior, in some cases, violence and other abuses occurred [9]. It was also found that women who tested positive for gonorrhea had more lifetime sexual partners, had the average age of 21, and were unemployed. An association of sexual power and reliability of condom use and gonorrhea infection was discovered. With low condom use, selfefficacy was an increased risk of inconsistent condom use. After a positive diagnosis among women, more educated (students in tertiary institutions) women tended to have more confidence in sexual condom negotiation and stronger choices about whether or not to stay in dysfunctional relationships than women who did not complete high school or did not further their education after high school.
Theme #5: Gender-based violence (GBV). This was found to be a problem among the women that live in Langa. Langa is an impoverished area and most of the study participants live in informal settlements, where violence is typical of daily life. Relationships are no exception. Similar to what was documented by WHO [17], GBV is ignored in the community and as a result, women continue to suffer health and disease burdens behind closed doors. There was a split among the women in the study. There were some women that are very traditional minded; meaning that they are comfortable with the traditional gender role of staying in the home while their partner or his family provides for the household, where other women were breaking those norms and becoming educated and getting jobs to have independence and more control in decision making [18]. Among those solely dependent on their partner, most cases of GBV were found. As documented in literature, male domination was found in those cases of dependence and alcohol abuse was indicated as well. This was found though the following questions in the interview:
- Have you ever been a product of sexual abuse, or know of anyone that has been abused sexually? Please explain.
- Have you ever experience violence in your relationship? If so, what were some of the things that angered your partner?
Among some of the study participants, violence was observed with physical indicators of this violence. A few of the women had visible marks that they said was due to their partners abusing them after fights and the majority of those said women are still currently with their partners. This was evident in the responses from one participant (#12):
My boyfriend used to cheat with me and when I tried to cheat also he kicked me right. When I tried to defend myself, [he said] no you can’t fight with me although you are cheating. When I tried to get out and go to the police station, he locked me in the house. [Do you live with him?] No, I live with my parent. He left me in his house for 2 days. No one came to see me until I said I’m sorry and it wasn’t my fault. [How long have you been with this boyfriend?] Three years and yes, I am still with him. [When you told him you had gonorrhea, he got upset with you?] I was upset with him when I went to the clinic and was told I had gonorrhea. I came back with the mind that it was him. So we fight and fight and when someone fights with me, I fight strong.
A participant (#8) has tried to coax her boyfriend into violence by saying the following:
Physical violence? Never. He can’t hit me. I don’t know if he can. I’ve tried so much. I wouldn’t lie, I haven’t. But then I know a lot of people around me that have. And every time, I would be amazed because they act so normal and it’s not right. They would say, yeah I got choked today and it’s not right.
At times the violence involves family members interceding on behalf of the abused
Participant #12:
[How does your family feel about your boyfriend?] They don’t want him--serious. Because we are always fighting and one day he stabbed me with a fork in the back and I came home with blood. They said I must leave him and must not stay with him and they said he will kill you. And you see this finger was not working because he bent it backwards and my family was not comfortable. They see we are better now but don’t talk to use about the relationship.
A participant (#10) cited that she knew of someone that experienced violence in a relationship and alcohol was a factor in the abuse:
[Have you ever experienced violence in a relationship or know anyone that has?] Not me, but my friend. I didn’t understand because she would always have blue eyes, but would go back each time. We knew that when it was weekend time and both were drunk, maybe on Saturday, on Sunday there would be something on her face each week. She is still with the same person and she is fine with it. When you talk to her about it, she says you are jealous.[ Alcohol has a big influence on relationships you think?] Yes.
This study identified that GBV is still found to be a concern in the township and women are still suffering from abuse physically and mentally. Although all women had gonorrhea at some point, the behavior change after the diagnosis of more protective contraception was determined by factors such as GBV. Still being able to practice African traditions and respect among the genders is important to continue the culture in the future, but roles should be more defined and respected by both parties to reduce the burden of disease. Unfortunately, women are the effects of the division of the two genders and among the study participants that have visible and mental scars from the abuse they suffer, have no recourse to making their situation better and in most cases, are still with the partner even after countless situations of abuse. Because of this, re-infections occur and women become even more susceptible to other infections like HIV/AIDs and other STIs.
Social factors of community/environment were found to have an influence on sexual behavior among the women. Influences of poverty, unemployment, lack of resources, and Xhosa traditional practices were found at times to increase risk of unprotected sexual encounters.
Theme #6: Community/environment. The community/environment has an influence on the impact on the risk of infection. Langa is a majority African black township community that is riddled with unemployment and poverty. Questions asked in the interview relating to this theme included:
- How do you feel society has an influence on sexual behavior?
- How does the environment that you live in play a part in your sexuality or sexual contact?
The environment that one lives in can have an effect on supporting changing or maintaining safe behaviors especially in underserved communities. Identifying risks within a community can also have an impact on risk of infection. In Langa, many areas are poverty stricken and riddled with unemployment. Some of the informal settlements are without clean water and sanitation, which can place constraints on personal choice and decision making when it comes to safe sexual behavior practices because of a lack of basic needs. Pressures within the community, i.e. pressures among peers and family can also be influential on these practices. One participant (#9) responded to this by saying:
You get pressure from your friends. You may want to put yourself in their situation if they are happy so you will do things you don’t want to do to be on her level. You aren’t satisfied and feel used because you go for anyone that make you happy but that person doesn’t see anything in you but just giving you what you think you want or maybe what you think will be better for you.
Another statement regarding pressure from friends (participant #12):
[Do you feel that your environment has an influence on you sexually? Your behavior? Do you get pressure from your friends, your family to have sex?] Yes, my friends. Since then [after the positive diagnosis], they say you must have sex with your boyfriend when I had the problem. I decided to listen to them. They say I must get another boyfriend and leave my boyfriend. But I really love him (the first time I met him) so I don’t want to leave him.
Although one participant (#10) mentioned pressure from friends, they maintained self-empowerment despite the pressure:
[The last question is about the environment. And you said you stay in Langa. Does Langa and being in a township setting, have an influence on you and your behavior sexually? Do you get peer pressure from your friends, from family, from your boyfriend to have sex?] Um, from friends--they have children and I don’t, so they tell me not to use a condom so I will have children, but I don’t listen. They want me to have children while I’m still young because I’m 25 with no children. [So do you think it’s a bad thing to have kids?] It’s a bad thing. You are still a child at home and you bring in another child. In our townships, fathers are denying the children which is the most thing happening to us. Or maybe if they agree that that is their child, then his family would cut him off. [So mainly they are doing it because their family doesn’t want to assist them, is this new thing?] It’s not new. It’s been happening for a while. I want a proper job and then I can provide for my child and then I can have a child.
Another (participant #6) cited pressures from the community in regards to sexual behavior:
…in the community you get pressure into things like sexual things. You get pornography and you don’t get concrete information with teaching about STIs. You make an effort to do it. A lot of young people don’t care to study about infections, and just want to enjoy life. That’s what people are in my community. They just want to live life the way they want to.
The majority of the women interviewed was unemployed and live vin the informal settlement area of Langa with no means of finances except for government pensions and vouchers. Most of the informal settlements have shack dwellings without clean water and sanitation which leaves most of the women without resources that are crucial for proper decision making and safe choices [15]. This makes it hard for the women to perceive their environment as supportive and welcoming to positive behaviors when it comes to sexual activity. Women get pressure from family and peers to maintain unhealthy relationships due to community stressors such as adequate housing, violence, insufficient food, and lack of reliable healthcare resources [19]. This research adds to the literature that environment dynamics have a major effect on perception of safety, support, and comfort among high risk women. When there is apathy towards living in impoverished conditions to suppress dire conditions faced with, there can be a major effect on taking risky behaviors with sexual practices to do whatever feels good or right at the moment and not necessarily contemplate consequences of actions.
Theme #7: Cultural limitations. Cultural limitations are placed on women at a very early age. In the Xhosa culture, men are dominant and the providers in the household. Not only this, culture maintains that traditions are the way of life in regards to health, religion, and choices in daily life. As times change and women become more modern and independent comes the power struggle that some of the study participants find to be difficult when navigating through relationships and sexual practices [20] that women are perceived to be less informed about sex and not as knowledgeable in behavior and experience as the men that pursue them. Women are to maintain their virginity for marriage, and most of the women find that this practice is becoming more and more of an old tradition that is sure not to change with time. Some of the questions asked of the women about cultural limitations were:
- Have you ever been considered “inexperienced” when it came to sex with your partner?
- What are some cultural limitations placed on you in regards to sexual activity?
In the Western Cape of Cape Town, South Africa, most African Blacks are of Xhosa descent. Within this culture, there are still many cultural practices that are carried out and traditions that are maintained, especially in township settings. The cultural beliefs are that males are the dominant and that women should be more submissive and maintain that in relationships and subsequently in marriage. The power struggle remains and continues with sexual behavior in most relationships. According to one respondent (participant #3) when asked what kind of things in tradition is she subject to in her relationship, she said,
When my boyfriend wants to have sex now, I must have sex now.
Another stated (participant #9),
When you get married at an early age, or get pregnant before marriage, you will be pressured to get married. Many times they want to have a lot of kids and maybe you aren’t ready for that and do not matter if that is something you want to do.
Traditionally, men at a certain age are sent to “the bush” to learn about becoming a “Xhosa” man and to get circumcised as a reflection of his journey into manhood. One participant (#10) brought this up by saying,
Culture is a very important thing to us. If he is still a boy, it is a problem because it’s like the penis has a thing (foreskin) and I’ve heard it gets dirty and he doesn’t want to use a condom and that dirtiness comes to your vagina, so it’s better if he is a man.[Are there more men doing circumcision in the clinic now, or are they still going to the bush to do it?] Since it’s been introduced (in the clinic), I believe the ones that go to the bush are criticizing the ones that went to the clinic. It’s better to do it in the bush for respect, although it’s much safer in the clinic, but then culturally, better to do in the bush. When a boy becomes a man, they have to sit alone and will compare you to a boy if you do it in the clinic from my own understanding.
With time comes change and women are slowly becoming more independent with education and employment, but in the township, this is still yet to be the standard. This slow shift in the change in tradition was seen in a couple of responses from the participants. One (participant #8) said after being asked if there were limitations on sexual behavior in regards to culture:
At first I thought so, but after having sex for the first time, I’ve lost it-what the hell it’s not coming back. You know you say I want to save it for marriage, and when it happens, it happens and you can’t do anything about it. So now I can’t follow culture and religion. At church they say you should save virginity until marriage, but it is past that now.
Another responded (participant #6) to the question, “Do you feel that your culture has an influence on your sexual behavior,” by stating:
I think it prevents us from having sex. Xhosa women are supposed to get married first and be a virgin. But it’s not happening at all. Now, young women party, have sex and there is definitely a change from what it used to be.
This research adds to the literature that pressures from family and friends within the Xhosa culture did have a small influence on sexual behaviors among a small majority of women, but ultimately they felt that with more modern times, the pressures from these sources were slowly coming to an end albeit it not supported by some of the male partners and family in regards to religion and cultural practices and standards.
These findings extend the knowledge of what we know about this target population and also confirm that the lack of constant exposure to information to not only STIs in the general context but to particular types of STIs will make the population more susceptible to the disease. Even tertiary level education participants are in need of constant information exposure to eliminate the risk of gonorrhea and could be used as a resource to spread preventable behavior information to the less educated and younger groups in the townships to help to eliminate the potential epidemic of the microbial resistant form of gonorrhea.
The limitations thought to be a challenge before the study was conducted was the determination of which psychosocial determinant(s) influenced risky behavior with gonorrhea. The answer to this after conducting the interviews was that most of the determinants whether individual, partnership factors, or within society had some influence on sexual behavior among the women. Once broken down into variables within each context, specific psychosocial factors such as level of education, sexual control, issues in vulnerability, economic status, and social and cultural influences all have an effect on whether preventive measures are taken to reduce incidences of gonorrhea among Black women.
Acknowledgement & Declaration
This research was partially funded by the Presidential Fellowship for Social Change grant awarded from Walden University, MN.
References
- Centers for Disease Control and Prevention (2009) Sexually transmitted disease surveillance 2008.
- Muula AS (2008) HIV infection and AIDS among young women in South Africa. Croat Med J 49(3): 423-435.
- Centers for Disease Control and Prevention (2011) Antibiotic-resistant gonorrhea.
- Duse AG (2011) The Global Antibiotic Resistance Partnership (GARP). S Afr Med J 101(8): 551-596.
- Kahn T (2006) SOUTH AFRICA: Warning of growing resistance to gonorrhea drug therapy. Business Day, Johannesburg.
- Mabey D (2010) Epidemiology of STIs: worldwide. Med 38(5): 216-219.
doi: http://www.sciencedirect.com/science/article/pii/S1357303910000265 - Moodley P, Sturm AW (2005) Ciprofloxacin-resistant gonorrhoea in South Africa. Lancet 366(9492): 1159.
http://www.ncbi.nlm.nih.gov/pubmed/16198757 - Rudestam KE, Newton RR (2007) Surviving your dissertation: A comprehensive guide to content and process. (3rd edtn), Sage Publications, CA.
- Zhang Y, Wildemuth BM (2009) Qualitative analysis of content. In Applications of Social Research Questions in Information and Library Science. Greenwood Press, CA. 308-319.
- Fisher JD, Fisher WA (1992) Changing AIDS-risk behavior. Psychol Bull 111(3): 455-474.
- UNAIDS (2011) South Africa launches its National Strategic Plan on HIV, STIs and TB 2012-2016.
- Johnson L, Budlender D (2002) HIV risk factors: A review of the demographic, socio-economic, biomedical and behavioural determinants of HIV prevalence in South Africa. Care Monograph 8: 1-49. Retrieved from
https://www.commerce.uct.ac.za/Research_Units/CARE/Monographs/Monographs/mono08.pdf - Myers B, Kline TL, Browne FA, Carney T, Parry C, et al. (2013) Ethnic differences in alcohol and drug use and related sexual risks for HIV among vulnerable women in Cape Town, South Africa: implications for interventions. BMC Public Health 13: 174.
- Wechsberg WM, Luseno WK, Karg RS, Young S, Rodman N, et al. (2008) Alcohol, cannabis, and methamphetamine use and other risk behaviours among Black and Colored South African women: A small randomized trial in the Western Cape. Int J Drug Policy 19(2): 130-139.
- Moultries A, Kleintjes S (2006) Women’s mental health in South Africa: women’s health. South African Health Review 347-366.
- Pettifor AE, Measham DM, Rees HV, Padian NS (2004) Sexual power and HIV risk, South Africa. Emerging Infectious Disease 10(11): 1996-2004.
- World Health Organization (2013) Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and non-partner sexual violence. Geneva.
- Strebel A, Crawford M, Shefer T, Cloete A, Henda N, et al. (2006) Social constructions of gender roles, gender-based violence and HIV/AIDS in two communities of the Western Cape, South Africa. SAHARA J 3(3): 516-528.
- Kalichman SC, Simbayi LC, Jooste S, Cherry C, Cain D (2005) Povertyrelated stressors and HIV/AIDs transmission risks in two South Africancommunities. J Urban Health 82(2): 237-249.
- Nzewi O (2009) Exploring gender issues and men’s vulnerability to HIV/ AIDS in Sub-Saharan Africa. Policy Brief 56. Centre for Policy Studies, Johannesburg.
- Reddy P, Frantz J (2011) HIV/AIDS knowledge, behavior and beliefs among South African university students. SAHARA J 8(4): 166-170.
Indexed in





Total Visitors
Copyright © 2019 SciDoc Publishers. All Rights Reserved.
