Correlation of symptoms of infertile patients with endometriosis with the classification of the American Society for Reproductive Medicine
L.L.G. Cunha, B.E.S. Canto, R. de Oliveira*, M.B. Magalhães, C.P. Barbosa and F.L. Vilarino.
Human Reproduction and Genetics Center – Faculdade de Medicina do ABC, Santo André/SP, Brazil
*Corresponding Author
Renato de Oliveira,
Faculdade de Medicina do ABC,
Av. Príncipe de Gales, 821 – Santo André/SP,
CEP 09060-650, Brazil.
Tel/Fax: +55 11 4993-5464
E-mail: oliveiraxl@hotmail.com
Article Type: Review Article
Recieved: January 27, 2015; Accepted: March 12, 2015; Published: March 14, 2015
Citation: R. de Oliveira, et al., (2015) Correlation of symptoms of infertile patients with endometriosis with the classification of the AmericanSociety for Reproductive Medicine. Int J Reprod Fertil Sex Health, 2(2) 41-45. doi: dx.doi.org/10.19070/2377-1887-150008
Copyright: R. de Oliveira© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Endometriosis is a common gynecological disease associated with pelvic pain and infertility. There are discrepancies between the clinical presentation and the degree of the disease, suggesting the necessity of a better understanding of the pathophysiological mechanisms of endometriosis, besides highlighting the lack of a classification that considers the clinical picture of this disease. So, profiling the infertile patients with endometriosis in relation to their symptomatology becomes fundamental in the advancement of knowledge.
Methodology: Retrospective cross-sectional study of 450 medical records of infertile women with endometriosis. Symptoms were correlated with the degree of endometriosis and it with personal and obstetric history.
Results: The prevalence of dysmenorrhea was higher in more severe forms of the disease. Being in grades I, II, III and IV, respectively, 101 (74.3%), 56 (81.2%), 82 (87%) and 140 (92.7%), with P = 0.001. The intestinal disorders were more common with increasing grades of the disease: the grades I, II, III and IV, respectively, 60 (44.1%), 32 (46.4%), 56 (59.6%) and 97 (64.2%) P = 0.002. Family history of endometriosis was associated with grade III (P = 0.017), while depression, with grade I (P = 0.032).
Conclusion: Dysmenorrhea, intestinal disorders and the presence of a family history of endometriosis were associated with higher degrees of endometriosis. In contrast, depression interestingly presented significant correlation with the grade I. Understanding the correlation of infertility with endometriosis and the impact on the symptoms of these patients could help in designing a new and more comprehensive classification for endometriosis
2.Introduction
3.Methodology
4. Results
5. Discussion
6. Conclusion
7. Acknowledgement
8. Authors’ contribution
9.References
Keywords
Depression; Pain; Endometriosis; Family History; Grades.
Introduction
Endometriosis is a common gynecological disease that affects 6-10% of women of reproductive age, which 30-50% are infertile. In addition, endometriosis induces a chronic inflammatory reaction that can distort the female pelvis, justifying the association with infertility and pain [1, 2].
It affects in general, ovaries, fallopian tubes and uterine ligaments, peritoneum and vaginal septum; and less common, bladder, kidney, herniation sacs and intestine [3, 4]. It affects rarely pericardium, pleura and central nervous system. However, it is worth noting that 16% of patients are asymptomatic [5].
Being that 40% of symptomatic women cases are related with pelvic pain [6]. While 40 to 60% of affected women have dysmenorrhea and dyspareunia [7, 8].
A study with Brazilian patients identified an average time between onset symptoms and diagnosis of 3.5 years, which was lower when compared to international data [9]. Even so, the delay in diagnosis seems to stem from a false idea of a physiological dysmenorrhea, especially when there is a family history. This could retard the diagnosis by some professionals that minimize such complains. Consequently, psychological losses can occur, such as depression and decreased wellness [10].
The grade of endometriosis is established through surgery, as recommended by the American Society for Reproductive Medicine (ASRM) [11]. Although being the most widely used classification,this presents limitations because didn’t correlate with the severity of symptoms and have limited value in prognosis infertility and medical management [12, 13]. Even with the establishment of a relation between the depth of the lesions and pelvic pain, the ability of classification and symptoms correlation is smaller when endometriosis is correlated to infertility [14, 15].
That way, endometriosis seems to be a gynecological manifestation of a systemic disease, possibly associated with a number of other health problems [16]. And among the associations, stands out infertility.
A proper understanding of the correlation of symptoms and associated diseases of infertile women with endometriosis considering its extension cannot be put aside.
The impact of infertility in women's life is undeniable. When it is associated with endometriosis, another important factor limiting the quality of life of these patients, it’s essential to understand the aspects of this relationship in order to increase the possibilities for therapeutic strategies that can benefit these women.
Methodology
This is a retrospective cross-sectional study of 450 medical records of infertile patients cared for at the Human Reproduction Service, in the city of Santo André, Brazil, from October 2006 to May 2012.
We considered the age, duration of infertility, the presence of dysmenorrhea, dyspareunia, acyclic pain, changes in intestinal functions and urinary habits, in addition to obstetric history of pregnancy, childbirth, spontaneus abortion, and ectopic pregnancy.
Regarding family history, it was considered first grade relatives who had endometriosis, depression, rheumatic disease, lupus and fibromyalgia.
The grade of endometriosis was established from the reports of laparoscopy, with histopathologic confirmation, as recommended by the American Society for Reproductive Medicine (ASRM) [11], classifying them into grades I, II, III and IV, respectively, minimal, mild, moderate and severe.
Dysmenorrhea intensity was assessed by a visual analogue scale and pain intensity followed categorized standardization: 0 no pain; 1-3 as mild pain; 4 to 6, moderate pain; 7-9, severe pain and 10, disable pain [17].
Quantitative data were analyzed based on median, 25th percentile and 75th. The comparison of age and duration of infertility was performed by Kruskal-Wallis test. In the qualitative variables, was used absolute and relative frequency and the association was estimated using the chi-square test. The software used was Stata 11.0.
Results
The sample was based on medical records of 450 patients with endometriosis and infertility of endometriosis outpatient clinic of the Faculty of Medicine of ABC. Patients were classified as having endometriosis grade I (30.2%), grade II (15.3%), grade III (20.9%) and grade IV (33.6%).
The median age was 34 years for grades I, II and III; however the grade IV was 33 years old (P = 0.447), showing that there was no change in age in relation to disease severity. The same was observed for the duration of infertility, whose median was four years in all stages of the disease (Table 1).
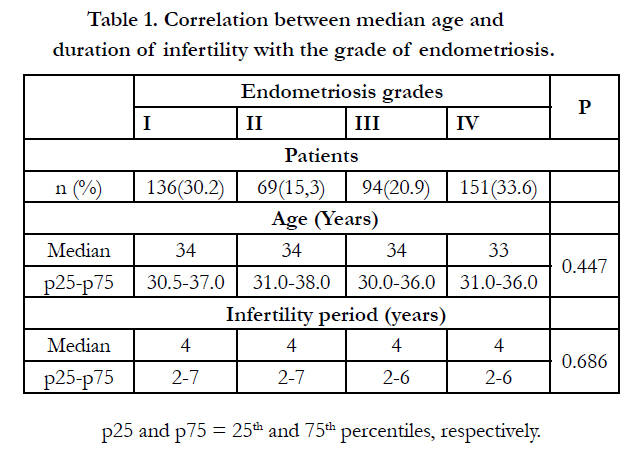

Table 1. Correlation between median age and duration of infertility with the grade of endometriosis.
p25 and p75 = 25th and 75th percentiles, respectively.
As for symptoms, it is realized that the prevalence of dysmenorrhea was higher in the more severe stages of the disease. In grade I, 101 (74.3%) had dysmenorrhea, grade II 56 (81.2%), grade III 82 (87%) and grade IV 140 (92.7%), with P = 0.001.
Dyspareunia was more frequent in grade IV with 67 (44.4%) than in patients on grade I with 40 (29.4%), II 27 (39.1%) and III 32 (34%). However, no significant progression of the percentage of prevalence of minimal to severe grades (P = 0.061) was observed.
The report of acyclic pain and urinary disorders also showed no statistical significance, respectively, P = 0.220 and P = 0.078.
Nevertheless the intestinal disorders were more frequent and statistically significant with the increase of the grades of the disease, 60 grade I (44.1%), grade II 32 (46.4%), grade III 56 (59.6%) and grade IV 97 (64.2 %), with P = 0.002 (table 2).
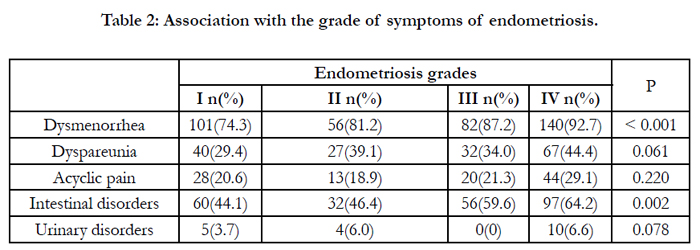
Table 2: Association with the grade of symptoms of endometriosis.
About dysmenorrhea, 147 patients had this complain which was evaluated according to visual analogue scale, with the following distribution: mild, moderate, severe and disabling. It is noteworthy that of the 140 patients with stage IV endometriosis with dysmenorrhea, 70 reported severe intensity (scale score 7-9). The graphical distribution of pain intensity according to the degree of endometriosis can be observed in Figure 1.
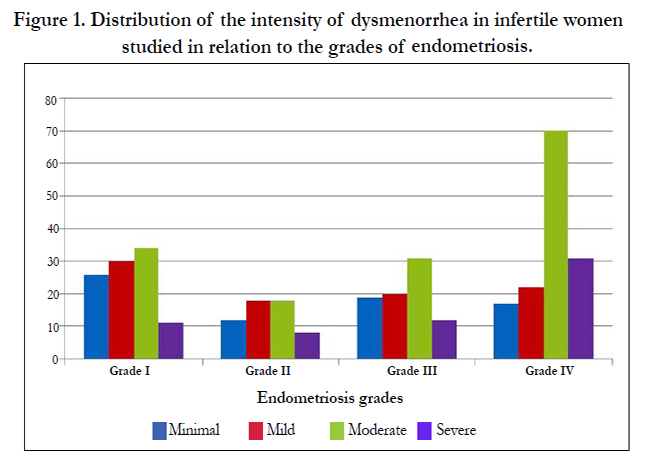
Figure 1. Distribution of the intensity of dysmenorrhea in infertile women studied in relation to the grades of endometriosis.
Considering obstetric history: pregnancy (P = 0.399), term labor (P = 0.103) and spontaneous abortion (P = 0.546), no statistically significant difference between groups was found. About a history of ectopic pregnancy revealed a statistically significant relationship with the severity of disease, but its validity is questionable due to the small sample of women in this group, total of 8 women, distributed as grade I 6 (4.4%), grade II 1 (1.4%) grade III 0 (0) and grade IV 1 (0.7%) (Table 3).
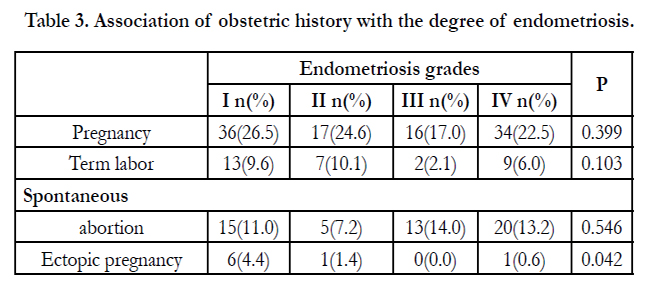
Table 3. Association of obstetric history with the degree of endometriosis.
Analyzing family history, endometriosis was found more frequently in stages III and IV and depression was found more frequently in stage I. Both with statistical significance, respectively, P = 0.017 and P = 0.032. About family history of rheumatic diseases, systemic lupus erythematosus and fibromyalgia, there was no statistical significance (Table 4).
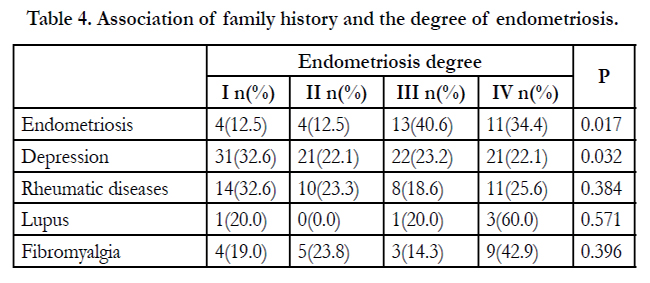
Table 4. Association of family history and the degree of endometriosis.
Discussion
Endometriosis, in approximately 20% of cases, is diagnosed in women undergoing laparoscopy for infertility with no other symptoms associated [22]. If the subject of laparoscopy is investigation of pelvic pain, endometriosis is found in 24% of cases [10].
It is estimated that the prevalence among asymptomatic patients is 10%, while several studies have observed increased presence of endometriosis in patients with symptoms compatible with the disease, such as infertility, dysmenorrhea, dyspareunia, acyclic pain, urinary and intestinal disorders [9, 10].
We found in our study, a median age of 34 years, consistent with the literature18. The period of infertility was 4 years, with no variations for the different degrees of endometriosis. This time is compatible with studies that suggest a period of 3.5 years from symptoms until disease diagnosis [9].
Vercellini et al [16] evaluated 1054 women with endometriosis, which presented a higher prevalence of this disease in the age range 25-35 years and were classified in grades I and II 43.5% of patients, and 56.5%, grade III and IV. These data were similar to those found in our study.
One of the symptoms of important clinical relevance in patients with endometriosis is dysmenorrhea [9, 16, 18]. This symptom was previously referenced without a significant association with the types of peritoneal implants, volume, number and depth of lesions and even with the degrees of the disease [16]. However, in this study we found a progressively increased prevalence according to the degree of endometriosis, in other words, women with grade I and II complained less about dysmenorrhea when compared to those with grade III and IV. We highlight the peculiarity that it was a group of infertile patients exclusively. Marana et al [19] also outlined this relationship. However, they found a difference in the prevalence of dysmenorrhea between grade I and III without showing a tendency to increase the severity of symptoms with disease progression.
Deep endometriosis is characterized by infiltrative lesions and is more localized in posterior fornix lesions, probably involving the retrocervical region or the rectovaginal fascia. There is a strict relationship between deep endometriosis and the highest prevalence of dyspareunia due to this anatomic distribution of lesions [7, 16, 18]. Although this study do not include a discussion about the exact location of the lesions, the ASRM classification considers as grade IV the most severe cases with multiple superficial and deep implants, endometriomas, dense and firm adhesions and posterior fornix commitment. In this study, dyspareunia was found more frequently in grade IV 67 (44.4%), corroborating such relation.
The same reasoning may be used for intestinal endometriosis which also revealed an increased prevalence proportionally to the severity of grade (P=0.002). Dyspareunia for example, is related to depth injuries that affect the large intestine, correlating with more severe grades of the disease. It is stipulated that intestinal involvement occurs in 6% to 30% of women with deep endometriosis. Bellellis et al [18], on an epidemiological study of patients with severe and disabling symptoms of endometriosis, found intestinal complaints in 48.3% of the women studied.
The relationship between pelvic pain and endometriosis is more complex than a simple comparison between the disease extension and referred pain. To support this assertion, animal trials suggest that the location and innervation of ectopic endometrium are more important for nociception than the extent of disease visually described [20]. Also, deep endometriosis lesions can be neurotrophic and more associated with nerve growth factors than compared to peritoneal and ovarian implants, therefore the greater association with pain [20].
Urinary disorder revealed no statistically significant difference between groups. One explanation would be the interpretation of women of this symptom as secondary. In the literature, the prevalence of urinary disorder is 11.7% of patients with endometriosis, and appointed it as the primary complaint in only 0.1% [18].
The correlation between disease severity with obstetric history is relevant, since many women with grades I, II, II and IV endometriosis who have difficulty in the conception and pregnancy maintenance, have some anatomic obstruction [21, 22]. There is also an association of endometriosis with infertility by cellular and molecular mechanisms affecting ovarian function, oocyte quality, embryo development, implantation and uterine function [21]. However, in the present study, we found no association between women who came to term labor and abortion with the extension of disease. The history of ectopic pregnancy revealed a significant association; however, its validity is questionable due to low sample of women in this group.
As for family history of endometriosis, there is more significant association with the higher grades of disease. One possible explanation to this fact is that it is a polygenic and multifactorial disease caused by the interaction between multiple genes and the environment [23]. It is known that there is an increased risk for disease development [11], even with progression to more advanced stages, in patients with 1st degree relatives with endometriosis [24]. This fact is observed in the present study.
Depression, another characteristic of these patients is known to be associated with infertility [25] and interestingly showed statistically significant association with the group of patients with endometriosis grade I, could be the result of not having previous knowledge about endometriosis. This way, in addition to deal with the frustration of not having achieved pregnancy, discover the presence of a proliferative disease, chronic and recurrent as endometriosis, it occurs in an emotionally exhausting period experienced by the infertile patient. Lawson et al [26] compared female fertility preservation patients with infertile patients in prospective study and related that the first group reported more anxiety and depression than infertile patients at enrollment in treatment, with more than one-third of fertility preservation patients reporting clinically significant depressive symptoms. However, infertile patients' anxiety and depressive symptoms increased across treatment. Besides, the authors suggest provided psychologic consultation before treatment to identify mood and anxiety symptoms and to refer patients for counseling as needed to prevent worsening of symptoms. Recognize the importance of this association would provide for women with endometriosis the benefit of strategies that help to reduce stress and develop confrontation mechanisms, contributing to break the vicious cycle of inflammation, sickness behavior and depression [27].
A limitation of this study is the lack of comparison of the group of infertile patients with endometriosis with a group of fertile patients with the same disease. However, considering that its realization occurred from the evaluation of women who sought a center for human reproduction, place where there is no demand for fertile patients is justified its realization.
Also, we demonstrate some statistically significant associations in this group of only infertile patients that are not a consensus in the literature when evaluating patients with endometriosis in general. We believe that this would justify the need to improve the classification proposed by the ASRM, so that other criteria such as fertility, symptomatology, in addition to personal and obstetric history were considered in order to advance in knowledge and in the best individualization of treatments. Careful meta-analysis would benefit the construction of a new classification for endometriosis. Thus, this study brings the benefit to help in this process, although further studies will be necessary to help building a new classification for endometriosis and fertility treatment.
Conclusion
The group of this study that consisted exclusively of infertile patients with endometriosis, dysmenorrhea, intestinal disorders and the presence of a family history of endometriosis are associated with greater grades of this disease. In contrast, depressionwas significantly correlated with the grade I. Understanding the correlation of infertility with endometriosis and the impact on the symptoms of this patient could help to develop a new wide classification and individualization of advances in treatments for women with endometriosis.
Acknowledgement
We thank the students Mariana Prince Santiago Fontes Ferreira and Deborah dos Santos Musich the important contribution in data collection. Professional of Instituto Idéia Fértil for customer service and follow-up of these patients. To Professor Fernando Adami by statistical evaluation.
Authors’ contribution
Laís Lourenção Garcia da Cunha, Bàrbara Elza Silveira Canto and Marina Brandã o Magalhã es make substancial contributions to acquisition of data, and analysis and interpretation of data, Renato de Oliveira make contributions to acquisition of data, and analysis and interpretation of data, drafting the article or revising it critically for important intellectual content, Caio Parente Barbosa give final approval of the version to be submitted and any revised version and Fãbia Lima Vilarino make substantial contributions to conception and design, in drafting the article or revising it critically for important intellectual content and give final approval of the version to be submitted and any revised version.
References
- Sugihara K, Kobayashi Y, Suzuki A, Tamura N, Motamedchaboki K (2014) Development of pro-apoptotic peptides as potential therapy for peritoneal endometriosis. Nat Commun 5:4478.
- Bulletti C, Coccia M, Battistoni S, Borini A (2010) Endometriosis and infertility. J Assist Reprod Genet 27(8):441-447.
- Minson FP, Abrao MS, Sardá JJ, Kraychete DC, Podgaec S (2012). Importância da avaliação da qualidade de vida em pacientes com endometrioses. Rev Bras Ginecol Obstet 34(1):1-15.
- Vilarino FL, Bianco B, Martins AC, Christofolini DM, Barbosa CP (2011) Endometriose em cicatriz cirúrgica: uma série de 42 pacientes. Rev Bras Ginecol Obstet 33(3):123-7.
- Barbosa CP, Souza AM, Bianco B, Christofolini D, Bach FA (2009) Frequency of endometriotic lesions in peritoneum samples from asymptomatic fertile women and correlation with CA125 values. Sao Paulo MedJ 127(6):342-5.
- Missmer SA, Cramer DW (2003). The epidemiology of endometriosis. Obstet Gynecol Clin North Am 30: 1-19.
- Fauconnier A, Chapron C (2005) Endometriosis and pelvic pain: epidemiological evidence of the relationship and implications. Human Reproduction 11(6): 595-606.
- Farquhar CM (2000) Extracts from the “clinical evidence”. Endometriosis. BMJ 320:1149-52.
- Santos TM, Pereira Am, Lopes RG, Depes D de B (2012) Lag time between onset of symptoms and diagnosis of endometriosis. Einstein 10(1):39-43.
- Bloski T, Pierson R (2008) Endometriosis and Chronic Pelvic Pain: Unraveling the Mystery Behind this Complex Condition. Nurs Womens Health 12(5):382-95.
- (1997) Revised American Society for Reproductive Medicine classification of endometriosis 1996. Fertil Steril 67(5):817-21.
- Kinkel K, Frei KA, Balleyguier C, Chapron C (2006) Diagnosis of endometriosis with imaging: a review. Eur Radiol 16(2): 285-98.
- Kennedy S, Berqqvist A, Chapron C, D’Hooghe T, Dunselman G (2005) ESHERE guideline for the diagnosis and treatment of endometriosis. Hum Reprod 20(1):2698-2704.
- Hoeger KM, Guzick DS (1999) An update on the classification of endometriosis. Clin Obstet Gynecol 42(3):611-9.
- Roberts CP, Rock JA (2003) The current staging system for endometriosis: doesithelp? Obstet Gynecol Clin North Am 30(1):115-32.
- Vercellini P, Fedele L, Aimi G, Pietropaolo G, Consonni D (2007) Associationbetween endometriosis stage, lesion type, patient characteristics and severity of pelvic pain symptoms: a multivariate analysis of over 1000 patients. Hum Reprod 22(1): 266-71.
- Carvalho DS, Kowacs P (2006) Avaliação da intensidade de dor. Migrâneas cefaleias 9(4): 164-168.
- Bellelis P, Dias Jr JA, Podgaec S, Gonzales M, Baracat EC (2010) Aspectos epidemiológicos e clínicos da endometriose pélvica: uma série de casos. Rev Assoc Med Bras 56(4): 467-71.
- Marana R, Muzii L, Caruana P, Dell'Acqua S, Mancuso S (1991) Evaluation of the correlation between endometriosis extent, age of the patients and associated symptomatology. Acta Eur Fertil 22(4): 209-12.
- Sinaii N, Plumb K, Cotton L, Lambert A, Kennedy S (2008) Differences in characteristics among 1,000 women with endometriosis based on extent of disease. Fertil Steril 89(3):538-45.
- Stilley JAW, Birt JA, Sharpe-Timms KL (2012) Cellular and molecular basis for endometriosis-associated infertility. Cell Tissue Res 349(3):849-62.
- Burns WN, Schenken RS (1999) Pathophysiology of endometriosis associated infertility. Clin Obstet Gynecol 42(3):586-610.
- Bischoff FZ, Simpson JL (2000) Heritability and molecular genetic studies of endometriosis. Hum Reprod Update 6(1):37-44.
- dosReis RM, deSá MF, deMoura MD, Nogueira AA, Ribeiro JU (1999) Familial risk among patients with endometriosis. J Assist Reprod Genet 16(9):500-3.
- Peterson BD, Sejbaek CS, Pirritano M, Schmidt L (2014) Are severed epressive symptoms associated with infertility-related distress in individuals and their partners? Hum Reprod 29(1):76-82.
- Lawson AK, Klock SC, Pavone ME, Hirshfeld-Cytron J, Smith KN, et al. (2014) Prospective study of depression and anxiety in female fertility preservation and infertility patients. Fertil Steril 102(5):1377-84.
- Siedentopf F, Tariverdian N, Rücke M, Kentenich H, Arck PC (2008) Immune status, psychosocial distress and reduced quality of life in infertile patients with endometriosis. Am J Reprod Immunol 60(5) :449-61.





